1 ufh is superior to placebo for reducing mortality and reinfarction in mi pts effect / 1,000 pts...
TRANSCRIPT

11
UFH is Superior to Placebo for UFH is Superior to Placebo for Reducing Mortality and Reinfarction in MI PtsReducing Mortality and Reinfarction in MI Pts
-10
-8
-6
-4
-2
0
2
4
Death ReMI CVA PE Major bleed
Eff
ect
/ 1,0
00 P
ts R
x’d
Routine ASARoutine ASA68,000 Pts68,000 Pts
93% Lysis Rx93% Lysis Rx
Collins R, et al. Collins R, et al. N Engl J MedN Engl J Med. 1997;336:847.. 1997;336:847.
P = 0.03 0.04 0.4 0.01 < 0.001

22
33 16,16716,167 387387 ReMIReMI 0.76 (0.62 – 0.93)0.76 (0.62 – 0.93)
33 16,16716,167 1,6871,687 DeathDeath 0.86 (0.62 – 0.93)0.86 (0.62 – 0.93)
LMWH is Superior to Placebo for Reducing LMWH is Superior to Placebo for Reducing Mortality and Reinfarction in STEMIMortality and Reinfarction in STEMI
0.50.5 11 22FavorsFavors LMWH LMWH
FavorsFavors Control Control
LMWHLMWH PlaceboPlacebo
OR
RCTsRCTs TotalTotal TotalTotalPts.Pts. EventsEvents
Eikelboom JW, et al. Eikelboom JW, et al. CirculationCirculation. 2005;112:3855. . 2005;112:3855.

3
EEnonoxxaparin and aparin and TThrombolysis hrombolysis RReperfusion for eperfusion for AAcute cute Myocardial InfarMyocardial Infarctctionion
ExTRACT-ExTRACT-TIMI 25TIMI 25
ACC 2006ACC 2006
Atlanta, GAAtlanta, GADisclosure StatementDisclosure Statement: :
Dr. Antman received research grant support via the Dr. Antman received research grant support via the Brigham and Women’s Hospital from sanofi-aventisBrigham and Women’s Hospital from sanofi-aventis
This presentation reflects the views of the presenter and does not necessarily reflect the views of the American College
of Cardiology. Content Distributed by Cardiosource.

4
BackgroundBackground
• Advantages of ENOX over UFHGreater anti Xa:anti IIa activityReliable A/C without monitoringConvenient sc administration
• Prior trials suggestENOX may be superior to UFH
• Pharmacologic reperfusion remains the most common treatment for STEMI
Definitive evaluation of ENOX vs UFH needed

5
Primary HypothesisPrimary Hypothesis
Compared to UFH, adjunctive antithrombin therapy with ENOX reduces the composite end point of all-cause mortality or non-fatal re-MI within 30 days in patients with STEMI who are eligible to receive fibrinolytic therapy.

6
Trial OrganizationTrial Organization
TIMI Study GroupTIMI Study GroupEugene BraunwaldEugene Braunwald Elliott M. AntmanElliott M. AntmanDavid A. Morrow David A. Morrow Carolyn H. McCabe Carolyn H. McCabeSabina Murphy Sabina Murphy Susan McHale Susan McHale
Sponsor: sanofi-aventis Sponsor: sanofi-aventis Frank JiangFrank Jiang Christophe GaudinChristophe GaudinPaul ChewPaul Chew Sylvie FontecaveSylvie FontecaveLu CuiLu Cui Kim GiordanoKim Giordano
Data Safety Monitoring BoardData Safety Monitoring BoardFrans Van de Werf (chair)Frans Van de Werf (chair) David DeMets David DeMets Desmond Julian Desmond Julian Jean Rouleau Jean Rouleau J. Ward Kennedy J. Ward Kennedy Jeffrey AndersonJeffrey Anderson

7
STEMI < 6 hSTEMI < 6 hLytic eligibleLytic eligible
Lytic choice by MDLytic choice by MD(TNK, tPA, rPA, SK)(TNK, tPA, rPA, SK)
ENOXENOX
< 75 y: 30 mg IV bolus < 75 y: 30 mg IV bolus SC 1.0 mg / kg q 12 h (Hosp DC)SC 1.0 mg / kg q 12 h (Hosp DC)
≥≥ 75 y: No bolus75 y: No bolus
SC 0.75 mg / kg q 12 h (Hosp DCSC 0.75 mg / kg q 12 h (Hosp DC))
CrCl CrCl << 30: 1.0 mg / kg q 24 30: 1.0 mg / kg q 24 hh
Double-blind, double-dummyDouble-blind, double-dummy
ASAASA
Day 30Day 3011°° Efficacy Endpoint: Death or Nonfatal MI Efficacy Endpoint: Death or Nonfatal MI1° Safety Endpoint: TIMI Major Hemorrhage1° Safety Endpoint: TIMI Major Hemorrhage
Protocol DesignProtocol Design
UFHUFH60 U / kg bolus (4000 U) 60 U / kg bolus (4000 U)
Inf 12 U / kg / h (1000 U / h)Inf 12 U / kg / h (1000 U / h)Duration: at least 48 hDuration: at least 48 hCont’d at MD discretionCont’d at MD discretion

8
Enrollment: Enrollment: Oct 2002 - Oct 2005Oct 2002 - Oct 2005N = 20,479 (ITT)N = 20,479 (ITT)
48 Countries48 Countries 674 Sites674 Sites
ArgentinaArgentina FinlandFinland LatviaLatvia SingaporeSingapore
AustraliaAustralia FranceFrance LebanonLebanon SlovakiaSlovakia
AustriaAustria GermanyGermany LithuaniaLithuania South AfricaSouth Africa
BelarusBelarus GreeceGreece MalaysiaMalaysia SpainSpain
BelgiumBelgium Hong KongHong Kong MexicoMexico SwedenSweden
BrazilBrazil HungaryHungary NetherlandsNetherlands SwitzerlandSwitzerland
BulgariaBulgaria IndiaIndia New ZealandNew Zealand ThailandThailand
CanadaCanada IrelandIreland NorwayNorway TurkeyTurkey
ChileChile Israel Israel PolandPoland UkraineUkraine
ChinaChina ItalyItaly PortugalPortugal United KingdomUnited Kingdom
CroatiaCroatia JordanJordan RomaniaRomania United StatesUnited States
EstoniaEstonia Republic of Republic of KoreaKorea
Russian Russian FederationFederation
UruguayUruguay

9
Baseline Characteristics-1Baseline Characteristics-1
44441313151547471818454577775959
ENOXENOX(n=10,256)(n=10,256)
1313Prior MI Prior MI (%)(%)
4444Hypertension Hypertension (%)(%)
1818Hyperlipidemia Hyperlipidemia (%)(%)
4747Current smoker Current smoker (%)(%)
1515Diabetes Diabetes (%)(%)
4444Anterior MI Anterior MI (%)(%)
7777Male Male (%)(%)
5959Age Age (yrs)-median(yrs)-median
UFHUFH(n=10,223)(n=10,223)
CharacteristicCharacteristic
ALL P = NSALL P = NS

10
Baseline Characteristics-2Baseline Characteristics-2
36366464
89890.40.416168282
ENOXENOX(n=10,256)(n=10,256)
3636> 3 > 3 (%)(%)
0.50.5LMWH within 7 d LMWH within 7 d (%)(%)
8989Killip Class I Killip Class I (%)(%)
TIMI Risk Score (STEMI)TIMI Risk Score (STEMI)
6464<< 3 3 (%)(%)
1616UFH within 3 h UFH within 3 h (%)(%)
8282CrCl CrCl (ml/min)-median(ml/min)-median
UFHUFH(n=10,223)(n=10,223)
CharacteristicCharacteristic
ALL P = NSALL P = NS

11
MedicationsMedications
6655551919
80802020
ENOXENOX(n=10,256)(n=10,256)
66rPA rPA (%)(%)
8080Fibrin-specific Fibrin-specific (%)(%)
1919TNK (%)TNK (%)
5555tPA tPA (%)(%)
2020SK SK (%)(%)
FibrinolyticFibrinolytic
UFHUFH(n=10,223)(n=10,223)
CharacteristicCharacteristic
ALL P = NSALL P = NS
12
MedicationsMedications
808086869595
ENOXENOX(n=10,256)(n=10,256)
7979ACEI / ARB ACEI / ARB (%)(%)
9595ASA (%)ASA (%)
8686Beta Blocker Beta Blocker (%)(%)
UFHUFH(n=10,223)(n=10,223)
CharacteristicCharacteristic
7070 7070Statin Statin (%)(%)
ALL P = NSALL P = NS

13
Primary End Point (ITT)Primary End Point (ITT)Death or Nonfatal MIDeath or Nonfatal MI
0
3
6
9
12
15
0 5 10 15 20 25 30
Pri
ma
ry E
nd
Po
int
(%)
Pri
ma
ry E
nd
Po
int
(%)
ENOX
UFH
Relative RiskRelative Risk0.83 (0.77 to 0.90)0.83 (0.77 to 0.90)
P<0.0001P<0.0001
Days Days
9.9%
12.0%
Lost to follow up = 3 Lost to follow up = 3
17% RRR

14
Treatment Benefit over Time (ITT)Treatment Benefit over Time (ITT)Death or Nonfatal MIDeath or Nonfatal MI
0
3
6
9
12
15
0 5 10 15 20 25 30
Pri
ma
ry E
nd
Po
int
(%)
Pri
ma
ry E
nd
Po
int
(%)
ENOX
UFH
Days Days
9.9%(1017)
12.0%(1223)
4.7%
5.2%
RRRR0.90 0.90
(0.80 to 1.01)(0.80 to 1.01)
P=0.08P=0.08
48 h48 h
UFH ENOX
206 events

15
Major Secondary End PointMajor Secondary End PointDeath or Nonfatal MI Death or Nonfatal MI
or Urgent Revascularization (ITT) or Urgent Revascularization (ITT)
Se
con
dar
y E
nd
Po
int
(%)
Se
con
dar
y E
nd
Po
int
(%)
Days Days
0
3
6
9
12
15
0 5 10 15 20 25 30
ENOX
UFH
11.7% (1199)
14.5% (1479)
5.3%
6.1%
RR 0.88 RR 0.88 (0.79 to 0.98)(0.79 to 0.98)
P=0.02P=0.02
48 h48 h
UFH ENOX
280 events
19% RRR
RR 0.81 RR 0.81 (0.75 to 0.87)(0.75 to 0.87)
P<0.0001P<0.0001
12% RRR

16
Outcomes at 30 Days (ITT)Outcomes at 30 Days (ITT)
7.5
4.5
2.8
6.9
3
2.1
0
1
2
3
4
5
6
7
8
Death Nonfatal MI Urg Revasc
RRRR
P valueP value
0.920.92
0.110.11
0.670.67
<0.0001<0.0001
0.740.74
0.00080.0008
%%
8%
33%
26%
UFHUFH
ENOXENOX

17
Outcomes at 48 hours (ITT)Outcomes at 48 hours (ITT)Comparison of DrugsComparison of Drugs
3.8
1.40.9
3.7
0.9 0.7
0
1
2
3
4
5
Death Nonfatal MI Urg Revasc
RRRR
P valueP value
0.980.98
0.760.76
0.670.67
0.0020.002
0.770.77
0.0860.086
%%
2%
33%23%
UFHUFH
ENOXENOX

Death or Nonfatal MI - Day 30 Death or Nonfatal MI - Day 30 Major SubgroupsMajor Subgroups
> Median
< Median
Fibrin-specific
Streptokinase
Prior MI
No Prior MI
DM
No DM
Other
Anterior
0.5 1 2
PRIOR MI
OVERALLOVERALL
DIABETES
FIBRINOLYTIC
INFARCT
LOCATION
ENOX Better UFH BetterRelative Risk
TIME TO Rx
20,479
1123
1721
1720
1318
2312
17
Reduction In Risk (%)
>= 75
< 75AGE (y)
206
Female
MaleSEX 1816
All Interaction TestsAll Interaction TestsP = NSP = NS
P < 0.0001

19
Death or Nonfatal MI - Day 30Death or Nonfatal MI - Day 30Medical Rx vs Any PCIMedical Rx vs Any PCI
0.00040.00040.0010.001
%
% E
ven
tsE
ven
ts
0
5
10
15
PCI Medical Rx
ENOX
UFH
Medical Rx
N = 15,223 (75%) Any PCI
N = 4,676 (23%)
ENOX
UFH
P ValueP Value
9.7
RRR 16%
11.413.8
10.7
RRR 23%

20
Death or Nonfatal MI - Day 30Death or Nonfatal MI - Day 30Clopidogrel UseClopidogrel Use
0.00050.0005 0.00060.0006
%
% E
ven
tsE
ven
ts
0
5
10
15
No Clop Clop
ENOX
UFH
No Clopidogrel
N = 14,752 (78%) Clopidogrel Used N = 5,727 (28%)
ENOX
UFH
P ValueP Value
10.4
RRR15%
12.211.4
8.7
RRR24%

21
Bleeding Endpoints (TIMI) Bleeding Endpoints (TIMI) 30 Days30 Days
1.4
0.40.9 0.7
2.1
0.81.3
0.8
0
1
2
3
4
5 UFHUFHENOXENOX
%
% E
ven
tsE
ven
ts
Major BleedMajor Bleed(Total)(Total)
ICH ICH
ARD 0.7%ARD 0.7%RR 1.53RR 1.53
P<0.0001P<0.0001
ARD 0.1%ARD 0.1%RR 1.27RR 1.27
P = 0.14P = 0.14
NonfatalNonfatalMajor BleedMajor Bleed
ARD 0.4%ARD 0.4%RR 1.39RR 1.39
P = 0.014P = 0.014
ARD 0.4%ARD 0.4%RR 1.84RR 1.84
P = 0.001P = 0.001
FatalFatalMajor BleedMajor Bleed

22
Net Clinical BenefitNet Clinical Benefit at 30 Days at 30 Days
11 1.251.250.90.90.80.8
Death or Nonfatal MI or Death or Nonfatal MI or Nonfatal ICHNonfatal ICH
Death or Nonfatal MI or Death or Nonfatal MI or Nonfatal Major BleedNonfatal Major Bleed
Death or Nonfatal MI orDeath or Nonfatal MI or Nonfatal Disabl. Stroke Nonfatal Disabl. Stroke
ENOX BetterENOX Better UFH BetterUFH BetterRRRR
UFH (%) ENOX (%) RRR (%)
12.3 10.1 18
12.8 11.0 14
12.2 10.1 17
Prespecified DefinitionsPrespecified Definitions
P <0.0001
P <0.0001
P <0.0001

23
For Every 1000 Pts For Every 1000 Pts Treated with EnoxaparinTreated with Enoxaparin
-15
-7 -6
4
-20
-15
-10
-5
0
5
Eve
nts
/ 1
000
Pts
Eve
nts
/ 1
000
Pts
Nonfatal Nonfatal reMIreMI
UrgentUrgent Revasc. Revasc.
DeathDeath Nonfatal TIMI Nonfatal TIMI Major BleedMajor Bleed
(No increase in (No increase in nonfatal ICH)nonfatal ICH)
++
24
Major Findings of Major Findings of ExTRACT-TIMI 25ExTRACT-TIMI 25
• Superiority of Enoxaparin StrategySuperiority of Enoxaparin StrategySignificant reduction of ischemic eventsSignificant reduction of ischemic events
• Management of STEMIManagement of STEMI Beneficial across a wide range of subgroupsBeneficial across a wide range of subgroups Useful for medical Rx or PCI post lysis Useful for medical Rx or PCI post lysis
• Risks of EnoxaparinRisks of EnoxaparinIncrease in major bleedingIncrease in major bleeding
• Net Clinical Benefit (3 Prespecified Definitions)Net Clinical Benefit (3 Prespecified Definitions)Significantly favors enoxaparinSignificantly favors enoxaparin

25
Potential ExplanationsPotential Explanations for Trial Results for Trial Results
• Superior antithrombotic effect of ENOX
• Longer duration of treatment with ENOX
• Rebound increase in thrombotic events after discontinuing UFH

26
Clinical ImplicationClinical Implication
A strategy ofA strategy of ENOXENOX is is clearly preferable to the clearly preferable to the current standard of current standard of UFHUFH as as the antithrombin to support the antithrombin to support fibrinolysis, the most fibrinolysis, the most common form of reperfusion common form of reperfusion for STEMI used worldwide.for STEMI used worldwide.

Publication of Primary ResultsPublication of Primary Results
Slides and Full Listing of Trial Participants at www.TIMI.orgSlides and Full Listing of Trial Participants at www.TIMI.org
www.NEJM.orgwww.NEJM.org

28
Trial Results In Perspective:Trial Results In Perspective: Major Bleeding Rates Major Bleeding Rates
5
2.5
1.40.9
3.3
2.11.3
0
2
4
6
8
10
% P
ts w
ith
Maj
or
Ble
ed%
Pts
wit
h M
ajo
r B
leed
KeeleyKeeleyLancet 2003Lancet 2003
EikelboomEikelboomCirc. 2005Circ. 2005
Major BleedMajor Bleed(Total)(Total)
Lytic ArmsLytic Arms
UFH UFH
LMWHLMWH UFH UFH
UFH UFH ENOX ENOX
UFH UFH ENOX ENOX
NonfatalNonfatal Major BleedMajor Bleed
Major Bleeds in Prior TrialsMajor Bleeds in Prior TrialsPooled DataPooled Data
29
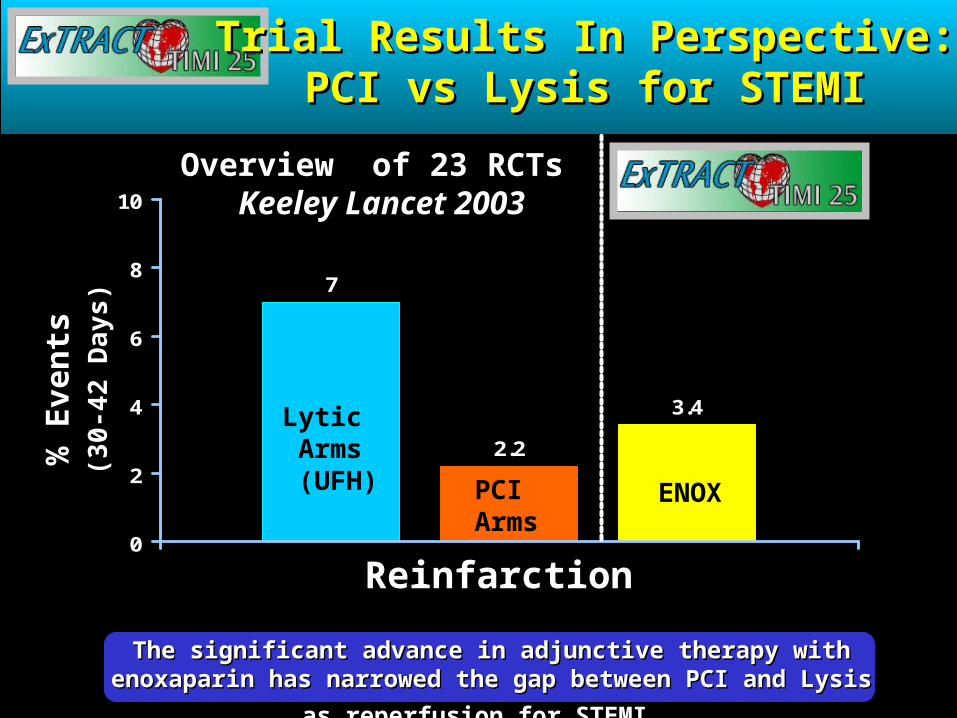
Trial Results In Perspective:Trial Results In Perspective:PCI vs Lysis for STEMIPCI vs Lysis for STEMI
7
2.2
3.4
0
2
4
6
8
10
% E
ven
ts%
Eve
nts
(3
0-42
Da
ys)
(30-
42 D
ays
)
ReinfarctionReinfarction
Lytic Arms (UFH) PCI
ArmsENOX
Overview of 23 RCTs Overview of 23 RCTs Keeley Lancet 2003Keeley Lancet 2003
The significant advance in adjunctive therapy with enoxaparin has The significant advance in adjunctive therapy with enoxaparin has
narrowed the gap between PCI and Lysis as reperfusion for STEMI.narrowed the gap between PCI and Lysis as reperfusion for STEMI.