1 respiratory viruses. 2 categories of respiratory viruses orthomyxoviridae: influenza virus...
TRANSCRIPT

1
Respiratory viruses

2
Categories of Respiratory Viruses
• Orthomyxoviridae: Influenza virus• Paramyxoviridae : Parainfluenza virus;
Mumps virus; Measles; Respiratory syneytical virus
• Togaviridae: Rubella Virus• Coronaviridae: Corona Virus; SARS virus• Adenoviridae : human Adenovirus • picornaviridae: Rhino Virus; • Reoviridae:

3
Influenza virus
Orthomyxoviridae: Influenza virusInfluenza is a disease caused by Influenza virus ,a member of the
Orthomyxoviridae.

4
Genome of Influenza virus
• 8 negative sense RNA nucleocapsid segments
• The 'RNP' (RNA + nucleoprotein) is in a helical form with the 3 polymerase polypeptides associated with each segment.
• The segmented genome promotes genetic diversity caused by mutation and reassortment of segments on infection with two different strains

5
Virion
• spherical/ovoid, 80-120nm diameter,
• The inner side of the envelope is lined by the matrix protein, stable type-specific.

6
Virion
• The outer surface of the particle consists of a lipid envelope from which project prominent glycoprotein spikes of two types, the haemagglutinin, ~135Å trimer (HA), and neuraminidase, ~60Å tetramer (NA).

7
Haemagglutinin (HA)
• Encoded by RNA segment #4 • Can agglutinate red blood cells - hence the
nomenclature • Cleavage by host-cell protease is required (resulting
in HA1 and HA2) for infection to occur
• Hemagglutinin glycoprotein is the viral attachment protein and fusion protein , and it elicits neutralizing , protective antibody responses

8
Neuraminadase (NA)
• Encoded by RNA segment #6 • Enzyme that uses neuraminic (sialic) acid as
a substrate • Important in releasing mature virus from cells

9
ORTHOMYXOVIRUSES
M1 protein
helical nucleocapsid (RNA plus NP protein)
HA - hemagglutinin
polymerase complex
lipid bilayer membrane
NA - neuraminidase
type A, B, C : NP, M1 protein sub-types: HA or NA protein

10
Influenza virus A

11
Replication
• Influenza transcribe and replicates its genome in the target cell nucleus
• assemble and buds from the plasma membrane

12
Influenza virus

13
Antigen
• Soluble antigens: include ribonucleoprotein and M protein which are much stable in antigenicity.
• Surface antigens: include HA and NA which are much variable in antigenicity.

14
Types• Influenza viruses are divided into 3 groups
determined by the ribonucleoprotein (RNP) antigen and M antigen:
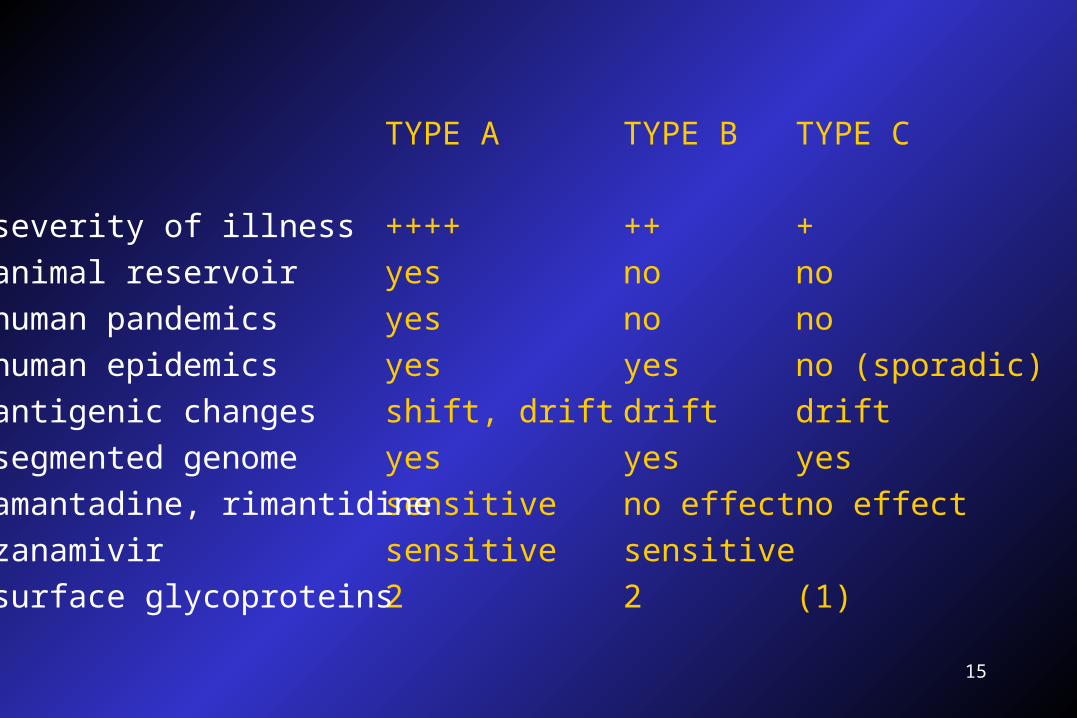
• Group A - This group is the cause of epidemics and pandemics and has an avian intermediate host (IH)Group B - This group causes epidemics and has no IHGroup C - This group does not cause epidemics and causes mild disease
15
TYPE A
++++
yes
yes
yes
shift, drift
yes
sensitive
sensitive
2
severity of illness
animal reservoir
human pandemics
human epidemics
antigenic changes
segmented genome
amantadine, rimantidine
zanamivir
surface glycoproteins
TYPE B
++
no
no
yes
drift
yes
no effect
sensitive
2
TYPE C
+
no
no
no (sporadic)
drift
yes
no effect
(1)

16
Subtypes
• According to antigenicity of HA and NA, influenza virus is divided into subtypes such as HnNm( H1N2, et al )

17
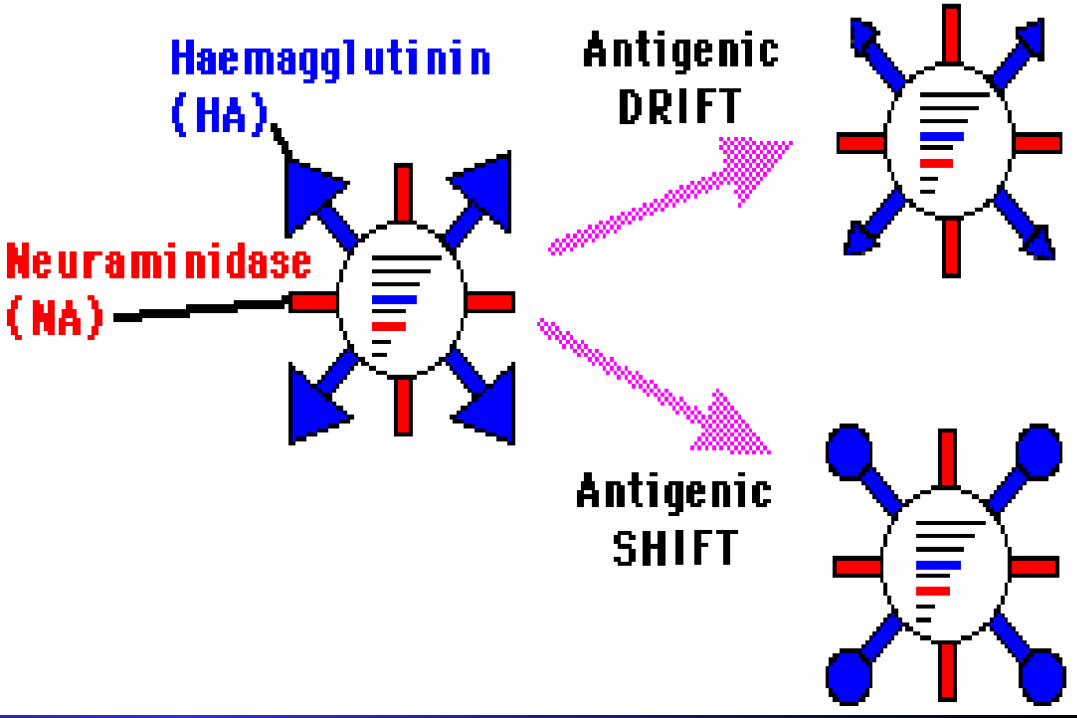
Variation and Epidemiology
Antigenic drift: median or small epidemic.
Antigenic shift:large scale epidemic.

18
Antigenic Shift Of Influenza virus
• Reassortment of genes is a common feature of Influenza A, but not B or C
• When two different "A" viruses infect the same cell, their RNA segments can become mixed during replication
• New viruses produced in this way may survive due to a selective advantage within the population

19
Antigenic Drift of Influenza Virus
•Constant mutations in the RNA of influenza which lead to polypeptide mutations
•Changes are less dramatic than those induced by Shift
•If these mutations affect HA or NA they may cause localized epidemics
20

21
Epidemic

22
where do “new” HA and NA come from?
• 13 types HA• 9 types NA
– all circulate in birds
• pigs– avian and human

23
where do “new” HA and NA come from?

24
why do we not have influenza B pandemics?
• so far no shifts have been recorded
• no animal reservoir known

25
Resistence
• The particles are relative labile ,not resistant to drying, etc.

26
Pathogenesis
• Influenza is characterised by fever, myalgia, headache and pharyngitis. In addition there may be cough and in severe cases, prostration. There is usually not coryza 鼻炎(runny nose) which characterises common cold infections.
• Infection may be very mild, even asymptomatic, moderate or very severe
27
Transmission
• Source of infection: patients and carriers.
• AEROSOL– 100,000 TO 1,000,000 VIRIONS
PER DROPLET
• 18-72 HR INCUBATION

28
AerosolInoculationOf virus

29
NORMAL TRACHEAL MUCOSA
3 DAYS POST-INFECTION 7 DAYS POST-INFECTION
30
SYMPTOMS
• FEVER
• HEADACHE
• MYALGIA( 肌痛 )• COUGH
• RHINITIS( 鼻炎 )• OCULAR SYMPTOMS

31
PULMONARY COMPLICATIONS
• CROUP (YOUNG CHILDREN)
• PRIMARY INFLUENZA VIRUS PNEUMONIA
• SECONDARY BACTERIAL INFECTION– Streptococcus pneumoniae– Staphlyococcus aureus– Hemophilus influenzae

32
NON-PULMONARY COMPLICATIONS
• myositis (rare, > in children, > with type B)
• cardiac complications
• liver and CNS– Reye’s syndrome
• peripheral nervous system

33

34
Immunity

35
Lab Diagnosis
• Viral detection:
Respiratory secretions
( direct aspirate , gargle , nasal washings )
1. Cell culture in primary monkey kidney or madindarby canine kidney cells
2. Hemagglutination (inhibition)
Hemadsorption (inhibition)
3. IFA/ ELISA

36
• Serology
hemagglutination inhibition
Hemadsorption inhibition
ELISA
immunofluoresence
complement fixation.
NT.

37
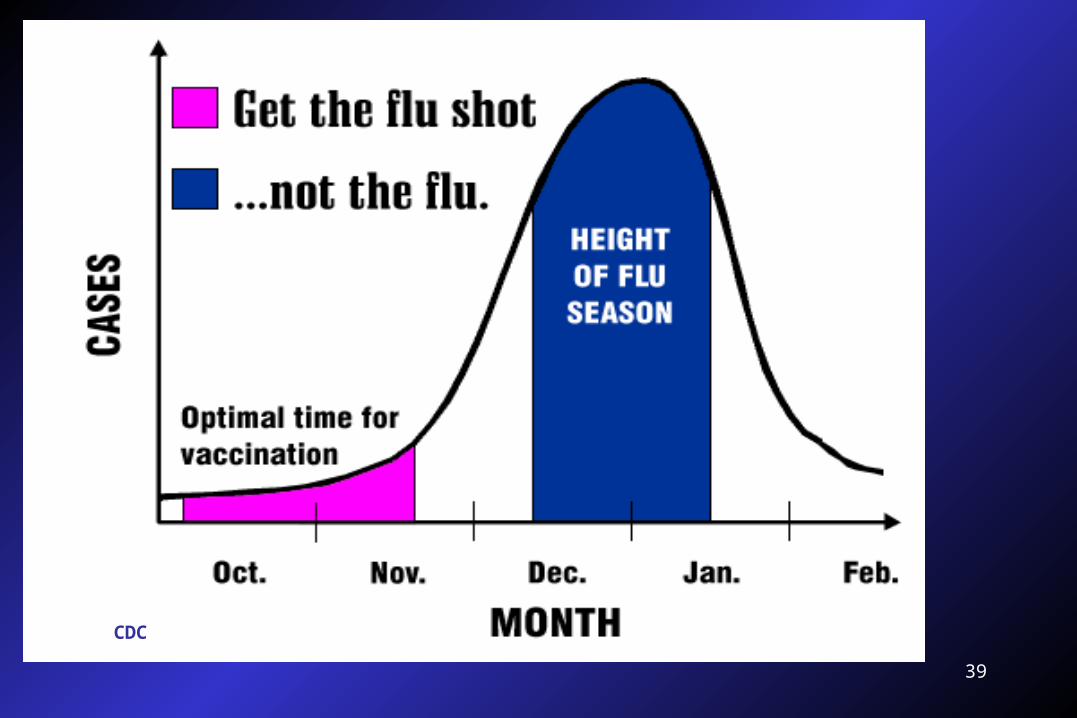
Prevention
• Vaccines at best give about 70% protection. They may sometimes not be effective against the most recently evolved strains because the rate of evolution outpaces the rate at which new vaccines can be manufactured.
• This constant antigenic change down the years means that new vaccines have to be made on a regular basis.

38
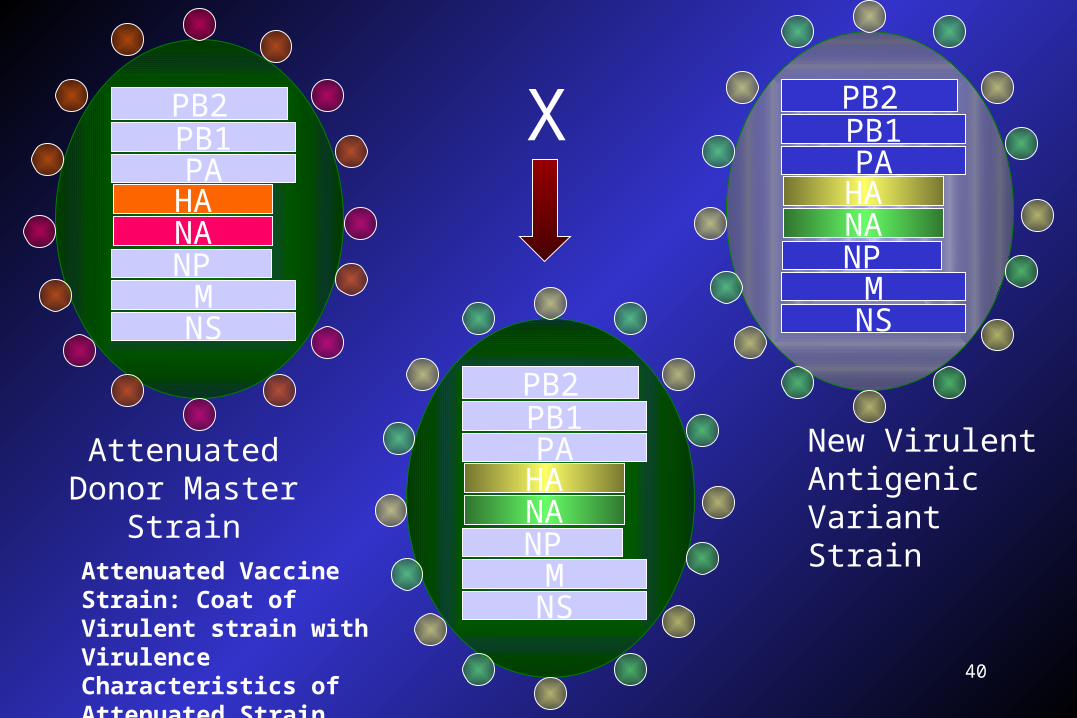
Types of Vaccine • Killed Whole Virus
Rather pyrogenic, not used today. • Live Virus
Attenuated strains were widely used in Russia but not elsewhere.
• Virus SubunitHA extracted from recombinant virus forms the basis of today's vaccines.For example, the WHO Recommendation for Influenza Vaccine, 1995-1996, contains two A strains and one B strain:-[A / Singapore / 6 / 86 (H1N1)+A / Johannesburg / 33 / 94 (H3N2)+B / Beijing / 84 / 93 ]
• SyntheticMuch research is being done to try and find a neutralising epitope that is more stable, and can therefore be used for a universal vaccine.
39
CDC
40
PB2PB1PA
HANANP
MNS
PB2PB1PA
HANANP
MNS
PB2PB1PA
HANANP
MNS
Attenuated Donor Master Strain
New Virulent Antigenic Variant Strain
X
Attenuated Vaccine Strain: Coat of Virulent strain with Virulence Characteristics of Attenuated Strain

41
Treatment
• Amantadine and rimantadine are active against influenza A viruses. The action of these closely related agents is complex and incompletely understood, but they are believed to block cellular membrane ion channels, and inhibit an uncoating step and target the M2 membrane protein

42
PREVENTION - DRUGS
• RIMANTADINE 金刚乙胺 (M2)• type A only
• AMANTADINE 金刚烷胺 (M2)• type A only
• ZANAMIVIR (NA)• types A and B, not yet approved for prevention but
studies show effective
• OSELTAMIVIR (NA)• types A and B

43
TREATMENT - DRUGS
• RIMANTADINE (M2)• type A only, needs to be given early
• AMANTADINE (M2)• type A only, needs to be given early
• ZANAMIVIR (NA)• types A and B, needs to be given early
• OSELTAMIVIR (NA)• types A and B, needs to be given early

44
OTHER TREATMENT
• REST, LIQUIDS, ANTI-FEBRILE AGENTS (NO ASPIRIN FOR AGES 6MTHS-18YRS)
• BE AWARE OF COMPLICATIONS AND TREAT APPROPRIATELY

45
Paramyxoviridae

46
Paramyxoviridae
• Genus Human pathogen
• Morbillivirus Measles virus
• Paramyxovirus Parainfluenza viruses,
Mumps virus
• Pneumovirus Respirtory syncytical
virus

47
VirionVirion
• Large virion consists of a negative RNA genome in a helical nucleocapsid surrounded by an enevlope containing a viral attachment protein
• HN of paramyxovirus and mumps virus has hemagglutinin and neuraminidase.
• H of measles virus has hemagglutinin activity
• G of RSV lacks these activities

48M protein
helical nucleocapsid (RNA plusNP protein)
HN/H/G glycoprotein SPIKES
polymerasecomplex
lipid bilayer membrane
F glycoprotein SPIKES
PARAMYXOVIRUSESpleomorphic

49
PARAMYXOVIRUS FAMILYproperties of attachment protein
GENUS GLYCOPROTEINS TYPICAL MEMBERS
Paramyxovirus
genusHN, F HPIV1, HPIV3
Rubulavirus Genus
HN, F HPIV2, HPIV4 mumps virus
Morbillivirus genus
H, F measles virus
Pneumovirus genus
G, F respiratory syncytial virus

50

51
Replication , Pathogenesis and Immunity • Virus replicates in the cytoplasm• Virions penetrate the cell by fusion with the plasma
membrane• Viruses induce cell-cell fusion, causing
multinucleated giant cells• Paramyxoviridae are transmitted in respiratory
droplets and initiate infection in the respiratory tract• Cell-mediated immunity causes many of the
symptoms but is essential for control of the infection

52
MMR vaccine
• Composition : live attenuated virus
Measles / Mumps / Rubella
• Vaccination schedule: at 15-24 months and at 4 to 6 years or before junior high school
• Efficiency: 95% lifelong immunization with a single dose

53

54
Measles virus(麻疹病毒)

55
Pathogenesis and Immunity
• Childhood infection almost universal, protection resulting from this is probably lifelong. Both man and wild monkeys are commonly infected
• In culture, produces characteristic intranuclear inclusion bodies and syncytial giant cells.
• Transmission and initial stages of disease similar to mumps, but this virus can also infect via the eye and multiply in the conjunctivae. Viraemia following primary local multiplication results in widespread distribution to many organs.
56
Pathogenesis and Immunity
• After a 10-12 day incubation period• Dry cough, sore throat, conjunctivitis (virus may be
excreted during this phase!), followed a few days later by the characteristic red, maculopapular rash and Koplik's spots
• Towards the end of the disease, there is extensive, generalized virus infection in lymphoid tissues and skin.

57
viremia

58
DISSEMINATED SPREAD• LONGER TIME FOR
SYMPTOMS• IMMUNE RESPONSE• IF SYMPTOMS DUE
TO IMMUNE RESPONSE, USUALLY INFECTIOUS PRIOR TO SYMPTOMS
Adapted from Mims, Playfair, Roitt, Wakelin and Williams (1993) Medical Microbiology

59
MEASLES - Koplik’s spots
Murray et al. Medical Microbiology

60
Koplik's spots

61
MEASLES - RASH
CDC - B.Rice Murray et al. Medical Microbiology

62
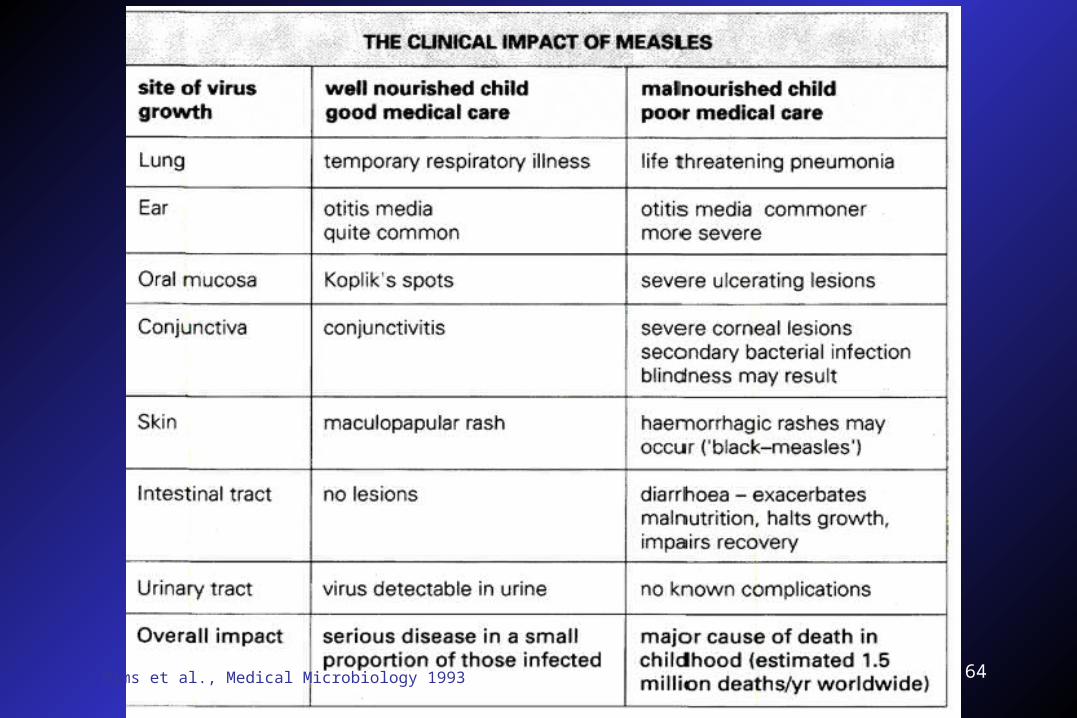
DISEASE• FEVER• RESPIRATORY TRACT SYMPTOMS
• rhinorrhea, cough
• KOPLIK’S SPOTS• MACULOPAPULAR RASH
• T-cells ->endothelial cells
• CONJUNCTIVITIS• epithelial cells

63
MEASLES GIANT CELL PNEUMONIA
Murray et al. Medical Microbiology
64Mims et al., Medical Microbiology 1993

65
MEASLES ENCEPHALITIS
• 1/1000 cases
• sequelae– deafness– seizures– mental disorders

66
SSPE
• sub-acute sclerosing panencephalitis– inflammatory disease– defective virus
• early infection with measles is a risk factor
• rare (7/1,000,000 cases of measles)
• decrease since vaccination program

67

68

69
Treatment
• No
70
Prevention
• Both live and killed vaccines exist. Vaccination with the live attenuated vaccine has been practised since the 1960's with a dramatic decline in the incidence of the disease .
• Trivalent live attenuated vaccine (MMR) usually given - all of these viruses best avoided during pregnancy!

71
Mumps virus(腮腺炎病毒)

72
Mumps virus
• Droplets spread the infection via saliva and secretions from the respiratory tract.
• Incubation period of 2-3 weeks

73
Mumps virus• Malaise and fever is followed within a day by
painful enlargement of one or both of the parotid (salivary) glands
• A possible complication in males after puberty is orchitis - painful swelling of one or both testicles.
• Inflammation of the ovary and pancreas can also occur.
• Disease is usually self-limiting within a few days • Aseptic meningitis (usually resolving without
problems) or postexposure encephalitis (can prove fatal) are the most serious complications associated with mumps.

74
Prevention and treatment
• Treatment: none (passive immunization has been used).
• Prevention: one invariant serotype therefore vaccines are viable - both formalin-inactivated and live attenuated exist, the latter now being widely used- see MMR.

75
MUMPS
CDC - B.Rice

76Mims et al., Medical Microbiology 1993

77
Mims et al., Medical Microbiology 1993

78
Parainfluenza virus(副流感病毒)

79
Important Characteristics
• Typing: Four types (1-4) : distinguished antigenically, by cytopathic effect, and pathogenically
• Hemeagglutinin and fusion F protein is found in the envelope

80
Pathogenesis and Immunity
• Cause acute respiratory infections of man ranging from relatively mild influenza-like illness to bronchitis, croup (narrowing of airways which can result in respiratory distress) and pneumonia; common infection of children.
• Transmitted by aerosols.

81
Lab Diagnosis
• Nasopharynx specimen is culture in a surrogate cell line in AGMK. Infected cell are detected by hemeadsorption or DFA
• DFA also can be done rapidly to identify the agent in direct specimen
• Serotypes 1-3 are comfirmed by hemeagglutination inhibition using standardized antisera

82
Treatment
• No antiviral therapy is available
• Nursing the patient in a humidified atmosphere was commonly advised
• Dexamethasone 地塞米松 and budesonide布德松 have been approved ( for outpatient treatments)

83
Prevention
• No, vaccines is not available

84
Respiratory syncytial virus(呼吸道合胞病毒)

85
Important Characteristics
• RSV is highly infectious, transmission by respiratory secretions.
• Primary multiplication occurs in epithelial cells of URT producing a mild illness. In ~50% children less than 8 months old, virus subsequently spreads into the L.R.T. causing bronchitis, pneumonia and croup.
• Has been suggested as a possible factor in cot death and asthma.

86
Pathogenesis and immunity
Disorder Age
Bronchiolitis Fever, cough, dyspnea, and
pneumonia, cyanosis in children younger
or both than 1 year
Febrile rhinitis Children
and pharyngitis
Common cold Older children and adults

87
Lab Diagnosis
• DFA
• Cell culture of nasopharyngeal specimen
• A rise in antibody titre using ELISA

88
Treatment
• Ribavirin aerosol( 三 ( 氮 ) 唑核苷 , 病毒唑 ) is recommended for pneumonia in infants
• RSV - IGIV has been approved for infants born prematurely
• IFN

89
Prevention
• Currently no effective vaccine! Also, infection does not result in lasting protection (c.f. mumps, measles) therefore repeated infections ('colds') occur throughout life - usually without serious consequences in adults.

90
Adenoviruses(腺病毒)

91
General Concepts
• Most Adenovirus infections involve either the respiratory or gastrointestinal tracts or the eye.Adenovirus infections are very common, most are asymptomatic. Most people have been infected with at least 1 type at age 15.

92
Adenovirus

93
Important Characteristics

94

95
Replication

96
Pathogenesis and Immunity
• Disease: At Risk:• Acute Respiratory Illness Military recruits, boarding schools,
• Pharyngitis Infants• Gastroenteritis Infants• Conjunctivitis All• Pneumonia Infants, military recruits• Keratoconjunctivitis All• Acute Haemorrhagic Cystitis Infants• Hepatitis Infants, liver transplant patients

97
swimming pool conjunctivitis( 游泳池结膜炎 ; 红眼病 )
• Eye infections characterized by a mild conjunctivitis "swimming pool conjunctivitis" are caused by adenoviruses and have been linked to transmission in contaminated swimming pools.

98
swimming pool conjunctivitis

99
Lab Diagnosis
• Isolation of adenovirus can be accomplished in cell cultures derived from epithelial cells
• Immunoassays, including fluorescent antibody and enzyme-linked immunosorbent assays, PCR can be used to detect and type the virus in clinical samples and tissue cultures
• Serological assays such as CFA, HI, EIA and neutralization techniques have been used to detect specific antibodies.

100
Treatment
• No

101
Prevention
• Inactivated vaccines have been developed and are routinely used for military recruits in some countries

102
Rubella Virus(风疹病毒)

103
General Concepts
• Viruses have enveloped single stranded positive-sense RNA.
• Replication in cytoplasm and bud at plasma membrane
• Cause Rubella( german measles, 3-days measles)

104
Epidemiology
• Occurrence: worldwide in prevalence( in winter and spring)
• Reservoir: Humans
• Mode of Transmission: Vertical transmission in case of CRS/ Infection in nonimmune children is usually transmitted by droplet spread or by direct contact with patients
• Who is at risk: Non-immunized children are at risk
• Incubation period: 2-3 weeks
105
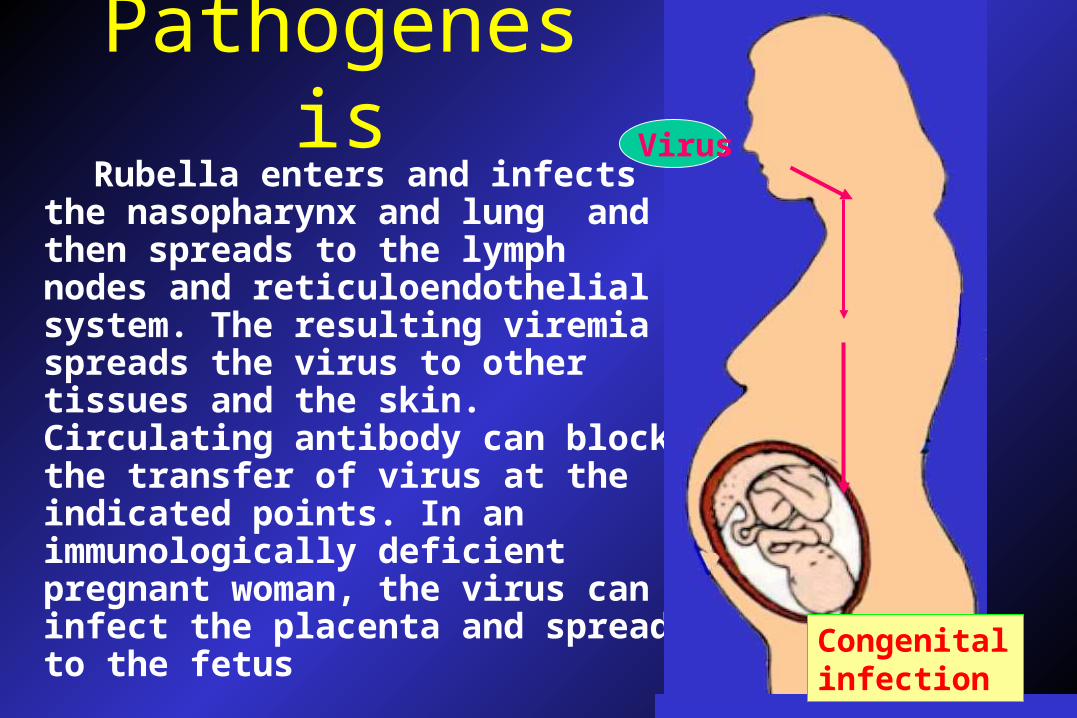
Pathogenesis Rubella enters and infects the
nasopharynx and lung and then spreads to the lymph nodes and reticuloendothelial system. The resulting viremia spreads the virus to other tissues and the skin. Circulating antibody can block the transfer of virus at the indicated points. In an immunologically deficient pregnant woman, the virus can infect the placenta and spread to the fetus
Virus
Congenital infection

106
EFFECTS ON FETUS
• HEARING LOSS
• CONGENITAL HEART DEFECTS
• NEUROLOGICAL– PYSCHOMOTOR AND/OR MENTAL
RETARDATION
• OPHTHALMIC– CATARACT, GLAUCOMA, RETINOPATHY

107
EFFECTS ON FETUS
• thrombocytopenia
• hepatomegaly
• splenomegaly
• intrauterine growth retardation
• bone lesions
• pneumonitis

108
EFFECTS ON FETUS
• First trimester– 65-85% of neonates have sequelae

109
EFFECTS ON FETUS
• 1964– 20,000 infants with permanent problems– 6,000 to 30,000 spontaneous abortions– 5,000 therapeutic abortions
• 1969 to present– maximum of 67 cases congential rubella/yr
• usually fewer than 10

110
CONGENITAL INFECTIONS
• SHED VIRUS FOR A YEAR OR MORE AFTER BIRTH– nasopharynx, urine, feces

111
CONGENITAL INFECTIONS
• EYE PROBLEMS
• GLANDULAR COMPLICATIONS– diabetes, – thyroid problems– deficiency growth hormone

112
CONGENITAL / VERY EARLY INFECTIONS
• PROGRESSIVE RUBELLA PANENCEPHALITIS
113
Lab Diagnosis
• Current rubella infection, in pregnant women can be confirmed by 4-fold rise in specific antibody titer between acute and convalescent-phase serum specimens by ELISA
• The Dx of CRS in the newborn may be confirmed by the presence of specific IgM antibody.

114
Treatment
• There is no antiviral therapy available

115
Prevention
• A single dose of live, attenuated rubella vaccine elicits a significant antibody response in approximately 98%-99% of vaccinated individuals
• It should not be given to immunocompromised patients

116
Coronavirus(冠状病毒)

117
Important Characteristics
• Virion: Spherical, 80-160nm in diameter, helical nucleocapside
• Genome: +ssRNA, linear, nonsegmented, 27-30kb, infectious
• Proteome: two glycoproteins and one phosphoprotein. Some viruses contain a third glycoprotein (hemagglutinin esterase)
• Envelope: contains large, widely spaced, club-or petal- shaped spikes. crown-like

118
Virion structure• S-Spike
glycoprotein: receptor binding, cell fusion, major antigen
• M-Membrane glycoprotein: transmembrane - budding & envelope formation

119
Pathogenesis and Immunity
• These viruses infect a variety of mammals & birds. The exact number of human isolates are not known as many cannot be grown in culture.
• They cause: common colds and have been implicated in gastroenteritis in infants.
• Transmitted by aerosols of respiratory secretions

120
Rhinovirus(鼻病毒)
121
Important Characteristics
• Rhinoviruses are picornaviruses similar to enteroviruses but differ from them in having a buoyant density in cesium chloride of 1.40 g/ml and in being Acid-labile
• Rhinoviruses are isolated commonly from the nose and throat but very rarely from feces.
• These viruses cause upper respiratory tract infections, including the common cold

122
Reovirus( 呼肠孤病毒 )

123
Important Characteristics
• Virion: Icosahedal, 60-80nm in diameter, double capsid shell
• Genome: dsRNA
• Envelope: none
• Diseases: Acute respiratory tract infection and Gastrointestinal infections