1 prospective studies on celiac disease alessio fasano and carlo catassi center for celiac research...
TRANSCRIPT
1
Prospective Studies on Celiac Disease
Alessio Fasano and Carlo CatassiCenter for Celiac Research
University of Maryland School of Medicine

2
To regulate the food is the main part of treatment…. The allowance of farinaceous food must be small; highly starchy food, rice, sago, corn-flour are unfit. Malted food is better, also rusks or bread cut thin and well toasted on both sides….
There is a kind of chronic indigestion which is met with in persons of all ages, yet is especially apt to affect children between one and five years old….
Signs of the disease are yielded by the faeces; being loose, not formed, but not watery; more bulky than the food taken would seem to account for…
The causes of the disease are obscure. Children who suffer from it are not all weak in constitution. Errors in diet may perhaps be a cause, but what error? Why, out of a family of children all brought up in much the same way, should one alone suffer?
Gee S. On the celiac affection. St Bart Hosp Rep 1890; 24: 17-20.
On the Coeliac Affection
3
Definition
• Celiac disease is an autoimmune condition• Occurs in genetically susceptible individuals
– DQ2 and/or DQ8 positive HLA haplotype is necessary but not sufficient
• A unique autoimmune disorder because:– both the environmental trigger (gluten) and the
autoantigen (tissue Transglutaminase) are known– elimination of the environmental trigger leads to a
complete resolution of the disease
4
Pathogenesis
• Genetic predisposition
• Environmental triggers– Dietary – Non dietary?

5
Treatment OptionsOption #1:
Remove the genesOption #2:
Remove the grains

6
Treatment
• Only treatment for celiac disease is a gluten-free diet (GFD)– Strict, lifelong diet– Avoid:
• Wheat• Rye• Barley

7
Sources of Gluten
• OBVIOUS SOURCES– Bread– Bagels– Cakes– Cereal– Cookies– Pasta / noodles– Pastries / pies– Rolls

8
Sources of Gluten
• POTENTIAL SOURCES– Candy– Communion wafers– Cured Pork Products– Drink mixes– Gravy– Imitation meat / seafood– Sauce– Self-basting turkeys– Soy sauce

9
Other non-Food RelatedItems to Consider
• Lipstick/Gloss/Balms
• Mouthwash/Toothpaste
• Play Dough
• Stamp and Envelope Glues
• Vitamin, Herbal, and
Mineral preparations
• Prescription or OTC Medications

10
• Only 50% of Americans with a chronic illness adhere to their treatment regimen including: – diet– exercise – medication
• Dietary compliance can be the most difficult aspect of treatment
Dietary Adherence:A Common Problem

11
Health Beliefs of Adults with Celiac Disease
• Survey of 100 people in Celiac Disease support group (Buffalo, NY)– Number of people who agreed with following statements:
• “If I eat less gluten I will have less intestinal damage.” –51%
• “I’ve lived this long eating gluten, how much will the gluten- free diet really help me now?” –33%
• “My doctor should be the one to tell me when I need follow up testing.” –26%
• “Scientist/doctors still haven’t proven that gluten really hurts them.” –16%

12
Barriers to Compliance
• Ability to manage emotions – depression, anxiety
• Ability to resist temptation – exercising restraint
• Feelings of deprivation
• Fear generated by
inaccurate information

13
Barriers to Compliance
• Time pressure – time to plan, prepare food is longer
• Planning – work required to plan meals
• Competing priorities – family, job, etc.
• Assessing gluten content in
foods/label reading• Eating out – avoidance, fear,
difficult to ensure food is safe

14
Gluten and treatment of Celiac Disease:How Much is Too
Much?
15
The gluten microchallenge study
Coordinator: Carlo Catassi, M.D.

16
Investigating the dose-effect relationship
the gluten microchallenge• CD patients on long-term, strict GFD• Prospective study design• While the GFD is maintained throughout
the study-period, a given amount of gluten/gliadin is added to the diet
• Clinical, serological and biopsy evaluation before and after the microchallenge
• The background noise caused by possible gluten contamination of the GFD was minimized by inclusion of a control group

17
DOSE-DEPENDENT EFFECTS OF PROTRACTED INGESTION OF SMALL AMOUNTS OF GLIADIN IN
CELIAC CHILDREN
• Positive linear relationship between gliadin daily dose and mucosal damage between 100 and 1000 mg/day
• IEL count is the most sensitive index
• Serological markers are not reliable tools for detecting minimal dietary transgressionsCatassi et al, Gut 1996
18
Why performinging a new microchallenge study
• Need of investigating the effects of lower gluten doses
• Need of prolonging the duration of the microchallenge
• Need of a control group
• Need of investigating gluten rather than gliadin

19
Gluten and Gliadins
• Gluten is the main proteic fraction in wheat (8-14 %);
• The toxicity is mainly due to the gliadins (50 %), however glutenins also contribute to toxicity;
• Daily intake of gluten in adults: ~ 15 g (Dautch data);
• Daily consumption of flower for a typical GFD in celiac subjects: ~ 80 g.
200g
Wheat
Gluten15g
Gliadin
7.5g~52 toxic fragments

20
The new microchallenge study
AIMTo evaluate the consequences of the protracted ingestion of minimal daily gluten intake (either 10 or 50 mg) in a group of adult celiacs on long-term treatment with the gluten-free diet (GFD)
TYPE OF STUDYMulticentre, prospective, randomized, placebo-controlled, double-blind
STUDY PERIODYears 2001-2004
SPONSORItalian Celiac Society (AIC)

21
The “new” Italian microchallenge study
INCLUSION CRITERIA• Patients with
biopsy-proven CD on a GFD for at least 2 years
EXCLUSION CRITERIA• Younger than 18 yrs• Poor compliance to
the GFD• Abnormal results at
the baseline evaluation
• Associated selective IgA deficiency

22
The Italian microchallenge studyStudy-Design
Steps
GFD 2 yrs Running-in Baseline Microchallenge T1
GFD
InterventionInformedconsentStrict monitoringof the GFD
ClinicalSerologySB Biopsy
Patient flow+ 50 mg gluten
+ 10 mg gluten
+ 0 mg gluten
Timeframe
Pre-T0 T0 1 2 3 m
Randomization Clinical Gluten exposure SerologyMonthly check SB biopsy
T0

23
The Italian microchallenge study
Methods• Purified gluten was used for the microchallenge
study (Amygluten 110, Tate & Lyle, UK)• Gluten- or lactose (placebo) containing capsules were
centrally prepared• All laboratory tests were centrally performed• Monthly monitoring of adherence to the protocol• Measurement of gluten contamination in
commercially available GF food by ELISA (Ridascreen Gliadin, R-Biopharm AG, Germany)
• Serum AGA (ELISA) and anti-tTG (ELISA)• Small bowel biopsy and morphometry on 10 villi, IEL
count (CD3+), ab IEL count• Control biopsies from non-celiac GI patients

24
Gluten content in commercially-available gluten free products in Italy where currently
food labeling policies for gluten free products are set at 20 ppm
0 10 20 30
flour
bread & cocereal mixcroissant
biscuits
pasta
Gluten (ppm)
Item

25
The Italian microchallenge studySubjects completing the study
T0 -> T1
n = 39
0 glutenn = 13
10 mg glutenn = 13
50 mg glutenn = 13
26
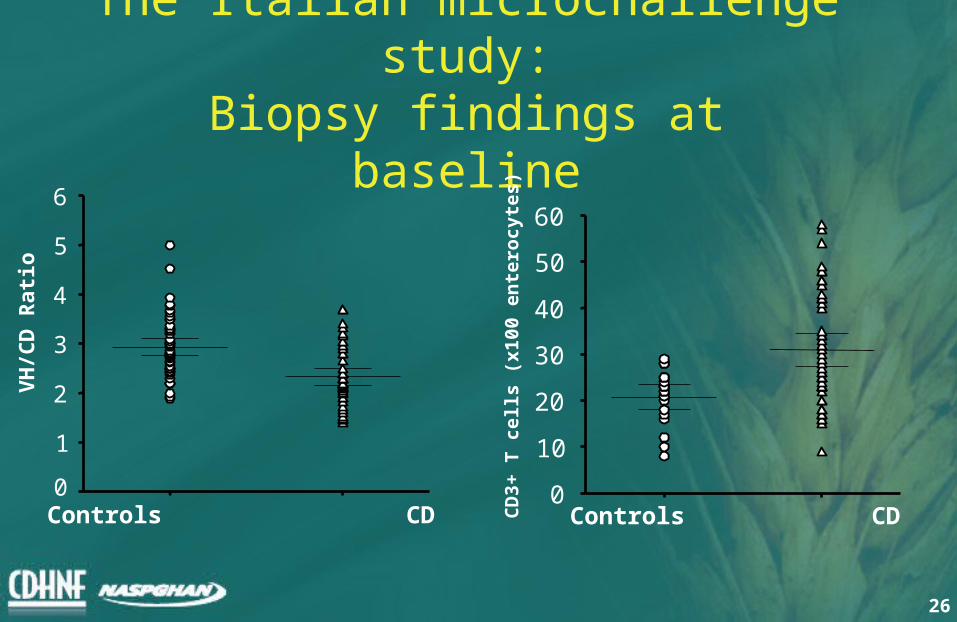
The Italian microchallenge study:
Biopsy findings at baseline
VH
/CD
Rat
io
Controls CD0
1
2
3
4
5
6
Controls CDC
D3+
T c
ell
s (x
100
en
tero
cyte
s)0
10
20
30
40
50
60

27
The Italian microchallenge study
Biopsy findings at baseline IE
L c
ou
nt
(X10
0 en
tero
cyte
s)
VH/CD Ratio
0 1 2 3 40
10
20
30
40
50
60
70
80

28
Symptoms Placebo 10 mg 50 mg
None 6 8 7Abdominal pain and distension 2 1 2Anemia and/or iron deficiency 1 0 0Loss of appetite 0 0 1Bloating, mood changes 2 1 0Apthous stomatitis 0 0 1Constipation 2 0 0Headache, abdominal distention 1 0 0 Weight loss 0 0 1
The Italian microchallenge study
Clinical findings
29
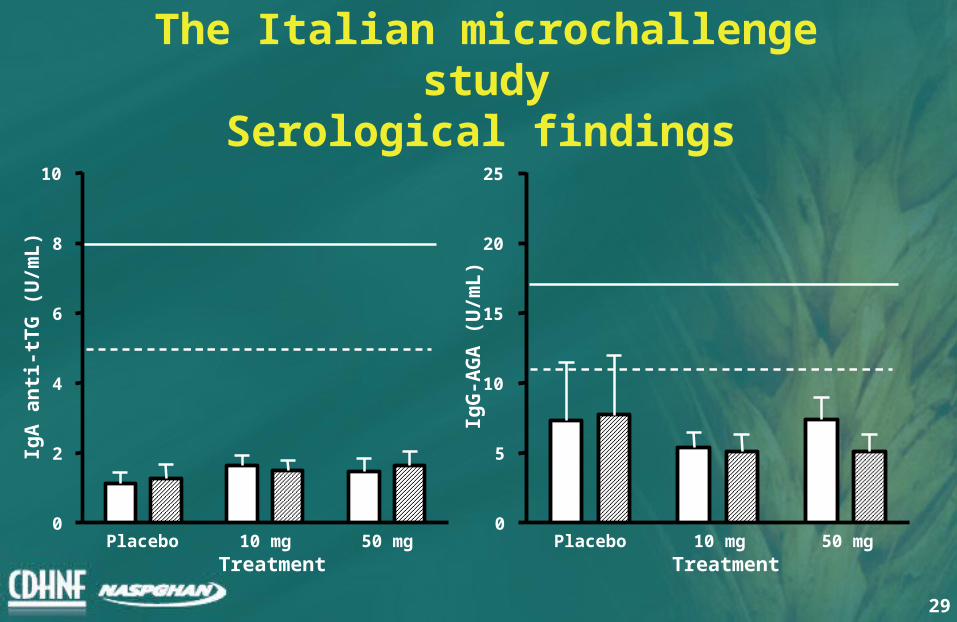
The Italian microchallenge study
Serological findings
Placebo 10 mg 50 mg0
2
4
6
8
10
Treatment
IgA
an
ti-t
TG
(U
/mL
)
Placebo 10 mg 50 mg0
5
10
15
20
25
Treatment
IgG
-AG
A (
U/m
L)

30
The Italian microchallenge study
Morphometry findings1
•50 mg significantly different from placebo (Kruskal-Wallis test)
Placebo 10 mg 50 mg0
1
2
3
Treatment
Vh
/Cd
ra
tio *

31
The Italian microchallenge study
Morphometry findings
Placebo 10 mg 50 mg0
5
10
15
20
25
30
35
40
45
Treatment
IEL
s c
ou
nt
(no
. x
100
ente
rocy
tes)

32
Tolerable daily intake of gluten and ppm of gluten in food for
celiacs50 g 100 g 200 g 300 g
200 ppm 10 mg 20 mg 40 mg 60 mg
100 ppm 5 mg 10 mg 20 mg 30 mg
50 ppm 2.5 mg 5 mg 10 mg 15 mg
20 ppm 1 mg 2 mg 4 mg 6 mg

33
Toxicity of gluten traces:the Italian study on gluten microchallenge
Catassi C1,2, Fabiani E1, Mandolesi A3, Bearzi I3, Iacono G4, D’Agate C5, Francavilla R6, Corazza GR7, Volta U8, Accomando S9, Picarelli A10, De Vitis I11, Bardella MT12, Pucci A13, Fasano A2
1 Department of Pediatrics, Università Politecnica delle Marche, Ancona, Italy; 2 Center For Celiac Research, University of Maryland School of Medicine, Baltimore (USA); 3 Department of Pathology, Università Politecnica delle
Marche, Ancona (Italy); 4 Department of Gastroenterology, Children Hospital, Palermo; 5 University Department of Gastroenterology, Catania; 6 University Department of Pediatrics, Bari; 7 University Department of Gastroenterology,
Pavia; 8 University Department of Internal Medicine, Bologna; 9 University Department of Pediatrics, Palermo; 10 Department of Gastroenterology, “La Sapienza” University, Rome; 11 University Department of Internal Medicine, “Gemelli” University, Rome; 12 University Department of Medical Sciences,
Milan; 13 Italian Celiac Society.