1 progressive states network: aca 101 sara rosenbaum, j.d. harold and jane hirsh professor, health...
TRANSCRIPT
1
Progressive States Network:ACA 101
Sara Rosenbaum, J.D.
Harold and Jane Hirsh Professor, Health Law and Policy
June 10, 2013

What Key Problems Was the ACA Designed to Address?
1. The lack of an accessible pathway to affordable insurance coverage for millions who– lack employer coverage– do not qualify for Medicaid because they don’t fit
the traditional coverage pathways and have incomes that are too “high”
– face a broken individual insurance market that barred people on the basis of health, cost, or both
2
What Key Problems Was the ACA Designed to Address?
2. Coverage that lacked value, leaving people without protection against both preventive benefits and catastrophic costs
– At one end, failure to cover high-value preventive benefits such as immunizations and screening for cancer, high blood pressure and other conditions
– At the other end, annual and lifetime limits on coverage that left persons with uncovered catastrophic costs
– Commonwealth Fund: 125 million Americans uninsured or underinsured
3

What Key Problems Was the ACA Designed to Address?
3. Poor access to health care services, especially urban and rural medically underserved communities lacking primary care
4. A health care system characterized by high costs and poor quality
– The highest per capita health spending in the world
– Failure to deliver services of known value in appropriate settings
– Failure to connect patients with medical and health homes
– Insufficient attention to prevention
– Payment systems that incentivize volume over value
– Excessive readmissions and preventable hospital-acquired conditions
4

Affordable Care Act Provisions Focus and Opportunities
Cathy Schoen, Senior Vice PresidentThe Commonwealth Fund
Progressive States Network ACA 101 WebinarJune 10, 2013

6
National Legislation – State/Local Reforms: Resources and Opportunities to Improve
• Insurance reforms: expand and improve coverage
– Enhance affordability and new market rules
• Payment reforms to support and stimulate innovation
– Primary care and Patient-Centered Care Teams
– Accountable Care Organizations
– Medicare, Medicaid and Private Initiatives
• Innovation Center: flexibility to partner/try new ideas
• Information systems and transparency
• New resources and tools to improve
– Access, quality/outcomes, and lower costs

7
Source: Modification of S. Guterman, et al. “Innovation in Medicare And Medicaid Will Be Central To Health Reform’s Success,” Health Affairs 29, no. 6 (June 2010).
ACA Timeline: Insurance, Payment and System Innovation Reforms
2010 2011 2012 2013 2014 2015
Initial insurance reforms
10% Medicare Primary Care
Increase
Innovation Center (CMMI)
Value-based Purchasing for
Hospitals
Primary Care and Health Homes
Reduce Payment for Preventable
Readmissions
Medicare Shared Savings (ACOs)
National Medicare Payment Bundling
Pilot
Major Insurance Expansions
Insurance Exchanges +
Credits
Medicaid
Insurance Market reforms
Value-based Purchasing for
Physicians
Medicaid Primary Care Payment up
to Medicare Levels
Reduce Payment for Hospital
Acquired Infections
Patient Centered Outcomes Research
Pioneer ACOs
Bundled Payment Improvement
Initiative
State InnovationGrants
October EnrollmentStarts for InsuranceExchanges for Jan 1, 2014
8
Insurance Expansion and Market Reforms
• New insurance marketplaces in all states for individuals and small business– Choice of qualified plans – web-based enrollment– Federal credits to lower premiums and cost sharing– State-based: federally run, partner, or state-run– Enrollment starts Oct 2013 for coverage in 2014
• Medicaid expansion to 138% of poverty ($ ) at state option– First 3 years 100 percent federal financed– Phase to 90 percent federal
• Insurance market reforms for all states– Premium oversight and benefit standards– Prohibition on higher premiums based on sex or health– Requirement to have insurance (low penalty starts 2014)

3% - 7%8% - 12% 13% - 18%19% - 24%25% - 31%
Adults Children
50 Million Uninsured 2010/11Percent of Adults (19-64) and Children (0-18) Uninsured
Data Source: Commonwealth Fund analysis U.S. Census Bureau, March 2011-12 Current Population Survey
9
9

Four levels of cost-sharing: 1st tier (Bronze) actuarial value: 60% 2nd tier (Silver) actuarial value: 70% 3rd tier (Gold) actuarial value: 80% 4th tier (Platinum) actuarial value: 90%
Premium Tax Credits and Cost-Sharing ProtectionsUnder the Affordable Care Act
Federal Poverty Level
IncomePremium
contribution as a share of income
Out of Pocket limits
Actuarial value: Silver plan
< 100%S: $11,490F: $23,550
MedicaidNo credits available Medicaid Medicaid
100 to 133% S: <$15,282F: <$31,322
2% if credit (or Medicaid)
S: $1,983F: $3,967
94%
133%- 149%S: $15,282 - <17,235F: $31,322 - <35,325
3.0%–4.0% 94%
150%–199%S: $17,235 - <22,980F: $35,325 - <47,100
4.0%–6.3% 87%
200%–249%S: $22,980 - <28,725F: $47,100 - <58,875
6.3%–8.05%S: $2,975F: $5,950
73%
250%–299%S: $28,725 - <34,470F: $58,875 - <70,650
8.05%–9.5% 70%
300%–399%S: $34,470 - <45,960F: $70,650 - <94,200
9.5%S: $3,967F: $7,933
70%
400%+S: $45,960+F: $94,200+
—S: $5,950F: $11,900
—
Note: Actuarial values: average percent of medical costs covered by plan. Premium and cost-sharing credits are for silver plan.Source: Federal poverty levels are for 2013; Commonwealth Fund Health Reform Resource Center: What’s in the Affordable Care Act? (PL 111-148 and 111-152), http://www.commonwealthfund.org/Health-Reform/Health-Reform-Resource.aspx.
10
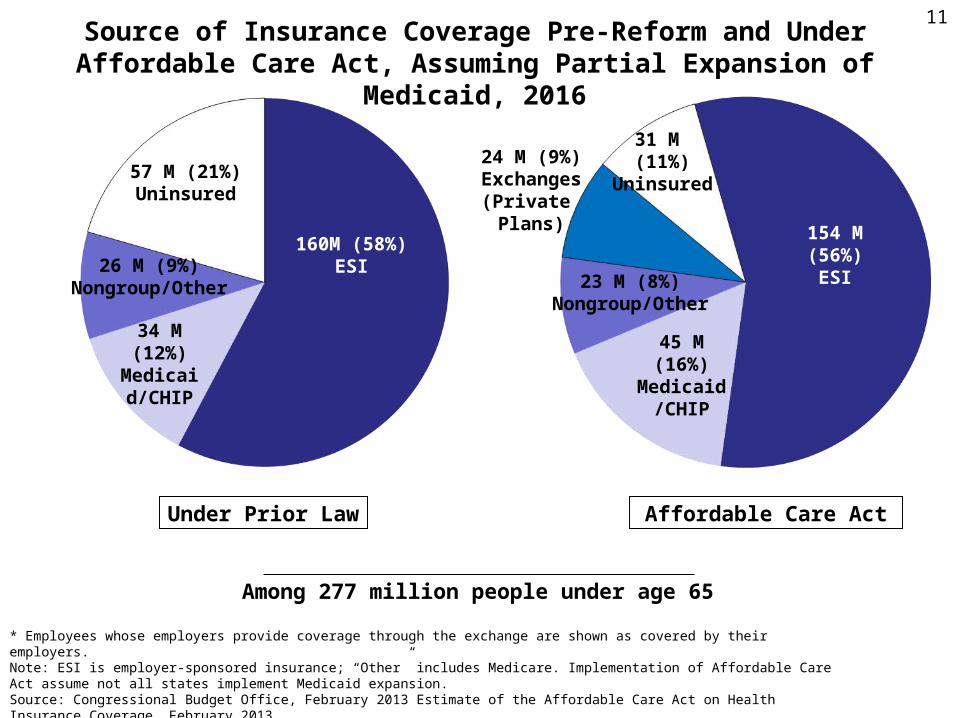
Source of Insurance Coverage Pre-Reform and Under Affordable Care Act, Assuming Partial Expansion of Medicaid, 2016
* Employees whose employers provide coverage through the exchange are shown as covered by their employers. Note: ESI is employer-sponsored insurance; “Other” includes Medicare. Implementation of Affordable Care Act assume not all states implement Medicaid expansion.Source: Congressional Budget Office, February 2013 Estimate of the Affordable Care Act on Health Insurance Coverage, February 2013. http://www.cbo.gov/sites/default/files/cbofiles/attachments/43900_ACAInsuranceCoverageEffects.pdf
Among 277 million people under age 65
Under Prior Law Affordable Care Act
45 M (16%)Medicaid/
CHIP
24 M (9%)Exchanges
(Private Plans)
23 M (8%)Nongroup/Other
31 M (11%)
Uninsured
154 M (56%)ESI
160M (58%)ESI
34 M (12%)
Medicaid/CHIP
57 M (21%)Uninsured
26 M (9%)Nongroup/Other
11

Source: National Conference of State Legislatures, Federal Health Reform: State Legislative Tracking Database. http://www.ncsl.org/default.aspx?TabId=22122; Avalere State Reform Insights; Center of Budget and Policy PrioritiesPolitico.com; Commonwealth Fund Analysis.
Medicaid Expansion
State Action on Establishing Health Insurance Marketplaces and Participation in Medicaid Expansion, As of May 2013
Health Insurance Marketplaces
Expanding (22 + DC)
Not expanding (16)
Unclear/undecided (9)
Expanding with variation (3)
Pursuing state-run exchange (17 + DC)
Pursuing state-federal partnership exchange (7)
Pursuing federally facilitated exchange (26)
12
Affordable Care Act: Key Insurance Reform State Implementation Issues, 2013-2014
• Readiness of insurance marketplaces for October 1, 2013 enrollment – Plans certified to be sold with network capacity and systems in place?– Plan premiums and cost-sharing. Are they viewed as “affordable”? – Outreach strategy, awareness of new choices and subsidies? – Experience of people choosing plans and access to tax credits?
• State Medicaid participation and alternate “private plan” approaches– Final decisions on State Medicaid expansion to 138% poverty– Coverage of people with incomes under poverty not eligible for tax credit – Coordination of Medicaid and new marketplaces – Offer a Basic Health Plan for those with incomes up to 200% poverty?
• Insurance market reforms– Oversight of premiums increases and insurance market– Prohibition on rating based on sex or health conditions– Essential benefit standards
13

Common ACA Myths1. The federal government will control the health care system
– A fundamentally state-based approach to system reform, within very broad federal parameters
2. Medicaid is costly and broken and needs an entire makeover – Medicaid is effective in improving health care access and
population health– Per capita Medicaid costs well below private insurance– States get $9.00 for every $1.00 invested. The 2014 adult
expansion = virtually no new net costs to states compared to current spending levels
3. Health Insurance Marketplaces are too complicated to work– Similar to any online shopping experience – Prior experience in Massachusetts and Utah– Outreach and assistance through Navigators & enrollment
assisters
14

Common ACA Myths
4. Reform will harm small employers– Smaller low-wage employers without health plans
are the biggest beneficiaries of the new Marketplaces and Medicaid expansions
5. Health insurance costs will skyrocket
Early reports: premium costs below projections without taking premium subsidies and cost-sharing assistance into account.
15

16Moving Forward: Improving Care System Performance and Confronting Cost
Uninsured Rates
Quality of Care Chasm
Costs of Care
Fragmentation &
Complexity

2003 2011
Affordability a Shared Concern: Premiums Rising Faster than Incomes Across the Country: 2003 and 2011
Sources: 2003 and 2011 Medical Expenditure Panel Survey–Insurance Component (for total average premiums for employer-based health insurance plans); 2003–04 and 2010–11 Current Population Surveys (for median household incomes for under-65 population).
Less than 14% 14%–16.9% 17%–19.9% 20% or more
ND
SD
DC
ID
DE
IA
IN
WI
CA
HI
KS
UT
AZ NM AR
LA
KYVA
VT NH
MA
CTRI
NJ
AK
ALMS
MI
ME
WV MDCO
NE
WY
OR
IL
TN NC
SCGA
FL
PA
NY
OH
MO
MN
OK
TX
MT
NV
WA
ND
SD
DC
ID
DE
IA
IN
WI
CA
HI
KS
UT
AZ NM AR
LA
KYVA
VT NH
MA
CTRI
NJ
AK
ALMS
MI
ME
WV MDCO
NE
WY
OR
IL
TN NC
SCGA
FL
PA
NY
OH
MO
MN
OK
TX
MT
NV
WA
80 percent of under-65 population live where premiums amount to 20 percent or more of median (middle) income
SOURCE: Schoen et al., State Trends in Premiums and Deductibles, 2003–2011: Eroding Protection and Rising Costs Underscore Need for Action, The Commonwealth Fund, December 2012.
17

ACA: Payment and Health System Reforms: Improving Outcomes and Lowering Cost
• Payment reforms to support and stimulate system innovation
– Primary care: enhance payment and “medical homes”
– Accountable care organizations: provider networks accountable for outcomes and total costs
– More “bundled” payments: total costs of care episode
– Pay for value: reduced payment for infections, readmissions
• Partnership with State Medicaid and Private Payers
• Federal Innovation Center: support private and state initiatives
• Investment in Information Systems & Data: guide and inform
18
19
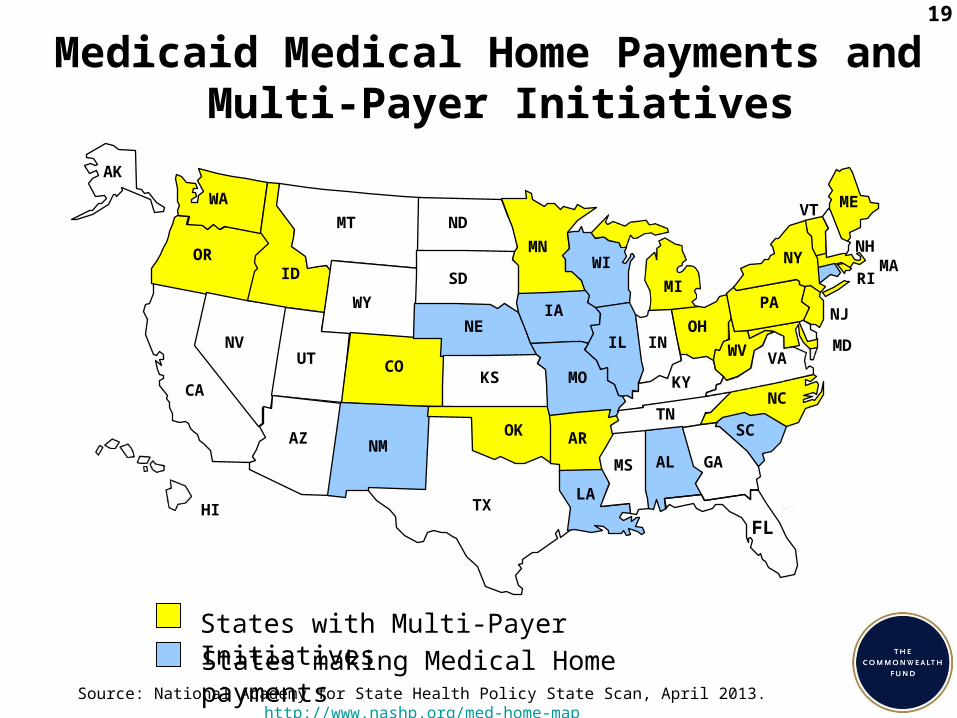
Medicaid Medical Home Payments and Multi-Payer Initiatives
Source: National Academy for State Health Policy State Scan, April 2013. http://www.nashp.org/med-home-map
WA
OR
TX
CO
NC
LA
PA
NY
IA
VA
NE
OK
RI
AL
MD
MT
ID
KS
MN NHMA
ME
AZ
VT
MOCA
WY
NM
IL
WI
MI
WV
SC
GA
FLHI
UTNV
ND
SD
AR
INOH
KY
TN
MS
AK
States with Multi-Payer InitiativesStates making Medical Home payments
NJ
Hawaii Puerto Rico
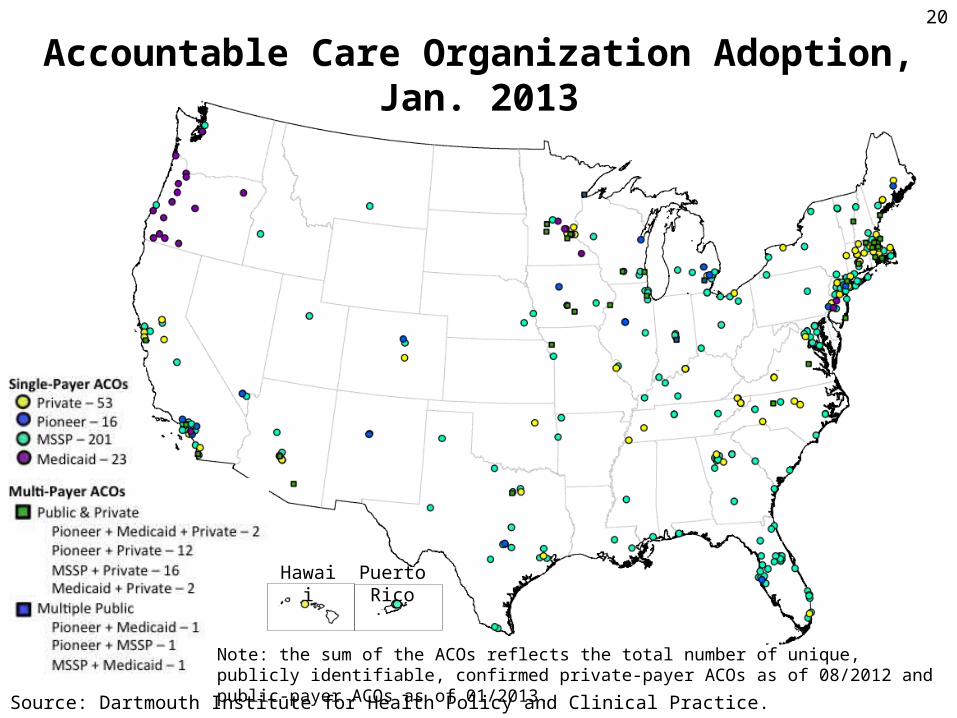
Accountable Care Organization Adoption, Jan. 2013
Note: the sum of the ACOs reflects the total number of unique, publicly identifiable, confirmed private-payer ACOs as of 08/2012 and public-payer ACOs as of 01/2013.
Source: Dartmouth Institute for Health Policy and Clinical Practice.
20

Reduced Payments for Avoidable Complications
Medicare Advantage Plan Bonuses
Bundled Payments
Physician Quality Reporting System
Meaningful Use
Value Based Purchasing
AccountableCare Organizations
Hospital Inpatient Quality Reporting
Medical Homes
The Affordable Care Act21
Prevention and PopulationHealth

ACA and Beyond: State Actions
• ACA reforms provide a foundation + new resources, tools– State policy and care system leaders’ action to move forward
• Key opportunities to build on momentum– Payer partnership with Medicare, Medicaid, private– Build innovation into state supported programs– Transparent all-payer data on quality and costs– Targets and benchmarks: populations and geographic areas
• Strategic action for public health as well as delivery systems
• Oversight to hold care systems and insurers accountable
– Licensure and regulatory authority
– Malpractice and other market reforms
• Future webinar: Delivery system and payment reforms
22