1 pediatric sleep disorders craig t. nakamura, m.d. z z z z
TRANSCRIPT
1
PediatricSleep
Disorders
Craig T. Nakamura, M.D.
Z Z Z Z . . .
3
TODAY’S OBJECTIVES:-- background-- obstructive sleep apnea-- sonambulism (sleep walking)-- night terrors-- sleep hygiene-- prevent everyone from
falling asleep
4
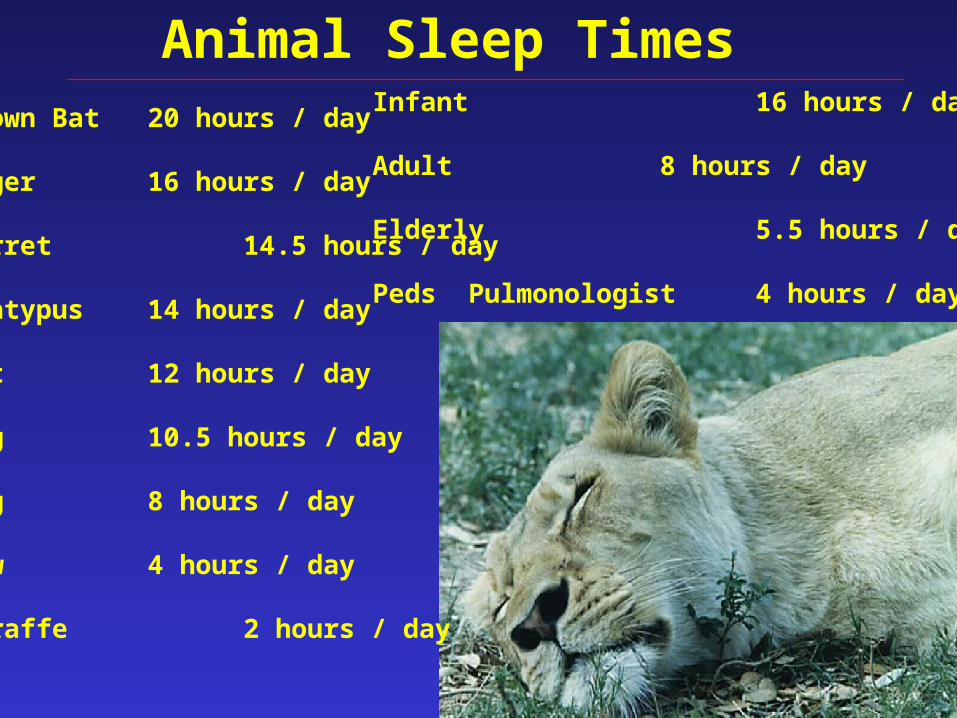
Animal Sleep TimesBrown Bat 20 hours / day
Tiger 16 hours / day
Ferret 14.5 hours / day
Platypus 14 hours / day
Cat 12 hours / day
Dog 10.5 hours / day
Pig 8 hours / day
Cow 4 hours / day
Giraffe 2 hours / day
Infant 16 hours / day
Adult 8 hours / day
Elderly 5.5 hours / day
Peds Pulmonologist 4 hours / day
5
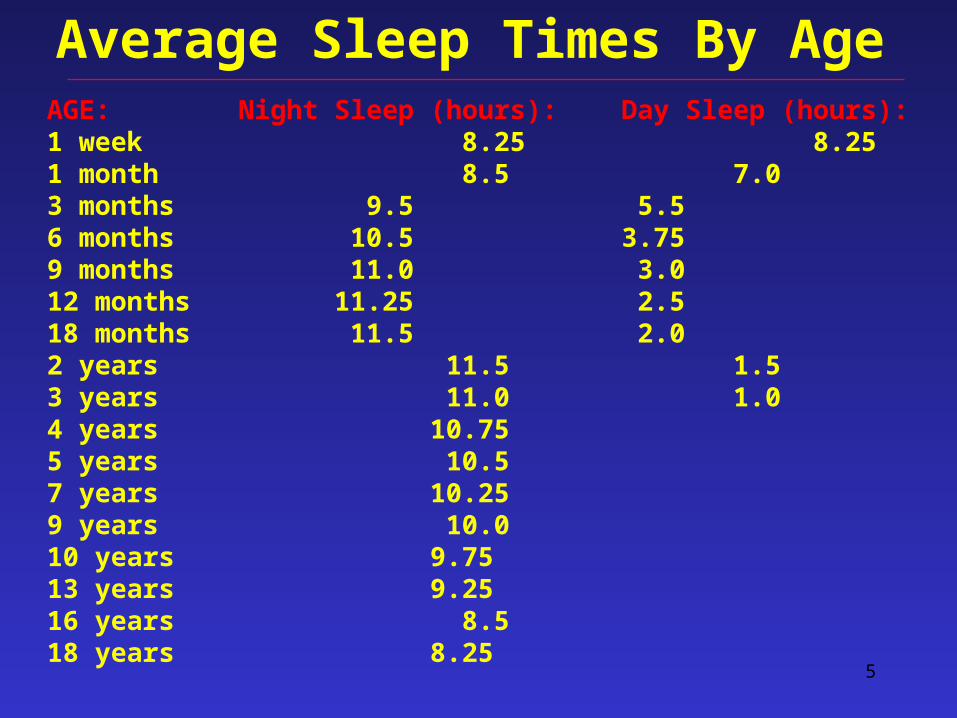
Average Sleep Times By AgeAGE: Night Sleep (hours): Day Sleep (hours):1 week 8.25 8.251 month 8.5 7.03 months 9.5 5.56 months 10.5 3.759 months 11.0 3.012 months 11.25 2.518 months 11.5 2.02 years 11.5 1.53 years 11.0 1.04 years 10.755 years 10.57 years 10.259 years 10.010 years 9.7513 years 9.2516 years 8.518 years 8.25
6
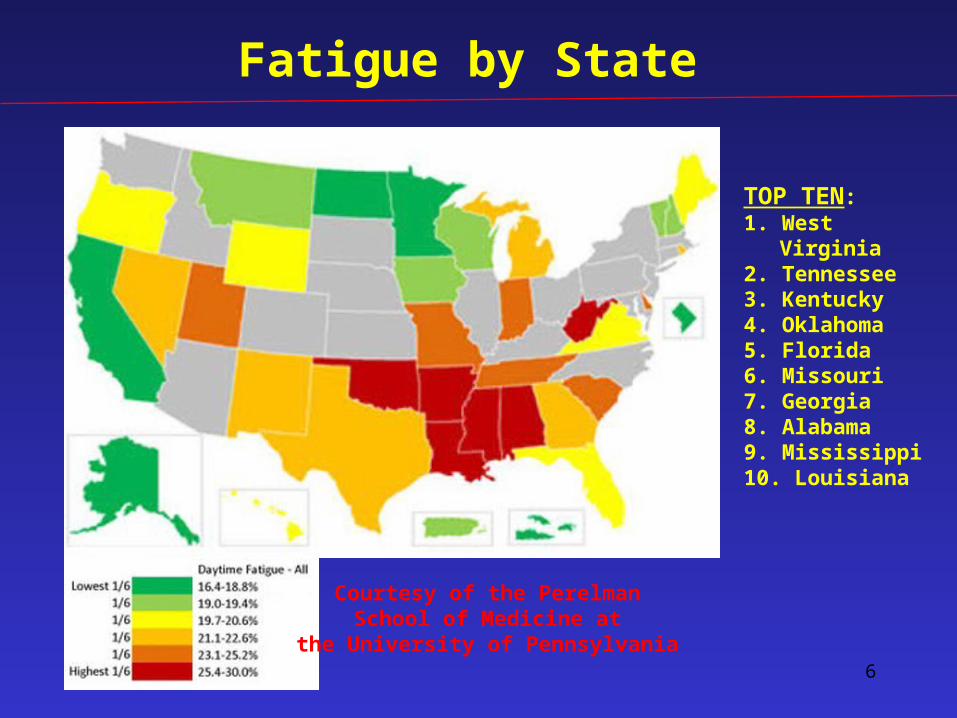
Courtesy of the PerelmanSchool of Medicine at
the University of Pennsylvania
Fatigue by State
TOP TEN:1. West Virginia2. Tennessee3. Kentucky4. Oklahoma5. Florida6. Missouri7. Georgia8. Alabama9. Mississippi10. Louisiana

7
Courtesy of the PerelmanSchool of Medicine at
the University of Pennsylvania
Sleep Disturbance by State
8
“Paying the Mortgage”
• Insufficient sleep sleep debt(eventually must be “repaid”)
• affects immunity• also nervous system• important for cycling of growth
hormone• In adults, ↑ rate of automobile
accidents by 3x
9
Sleep in Children
10
Sleep Induced Changes
Sleep impairs ventilation in all children (sick or healthy):
-- normal-- underlying respiratory illness-- CNS disease-- obstructive sleep apnea
11
Sleep Disorders in Children• If diagnosed and treated early,
morbidity can be avoided
• Therefore, important to recognize
signs of sleep-disordered breathing:
a) primary care providers
b) teachers
c) parents
d) local postman

12Sleep Stages
13
Sleep Stages
5 phases of sleep stages 1, 2, 3, 4, REM sleep
50% stage 220% REM sleep30% the other 3 stages
progresion from stages 1 to REM~ 90 to 110 min / total cyclethen cycle starts again
14
Stage 1 Sleep
light sleepdrift in and outeyes move very slowlymuscle activity slowswhen awaken, recall fragmented
visual imagessense of fallingmuscle contractions
15
Stage 2 Sleep
eye movements stopbrain waves become sloweroccasional bursts called
sleep spindles
16
Stages 3 & 4 (Deep) Sleep
no eye or muscle movementswhen awakened, groggy, disorientedbedwetting, night terrors, sleep walkingStage 3:
extremely slow (delta) brain waveswith smaller faster waves
Stage 4:delta waves
17
REM Sleeprapid, irregular breathingeyes jerk rapidlylimb muscles temporarily paralyzedheart rate & BP ↑bizarre / illogical dreamsfirst cycle 70 to 90 minutespenile erections HEH HEH. HE SAID, ERECTION.

18
Obstructive Sleep Apnea
19
Apnea: Greek word meaning
“want of breath”
20
Obstructive Sleep Apnea Syndrome (OSAS)
Disorder of breathing during
sleep characterized by
prolonged partial and / or
intermittent complete upper
airway obstruction that disrupts
normal ventilation and patterns
during sleep.
First described in 1965
21
Obstructive Sleep Apnea
• adults:cessation for > 10 seconds
• children:cessation for 2 ½ missed breaths
• with apneas, oxygen levels ↓, carbon dioxide levels ↑• also causes arousals and
fragmented sleep
22
Obstructive Sleep Apnea
• prevalence ~ 2%• affects millions• M = F• more common with family history of OSAS• ↑ in African Americans • ↑ in children with chronic respiratory tract infections
23
Obstructive Sleep Apnea
• ↑ in children 2 - 6 years of age
• same age of adenoidal & tonsillar hypertrophy
• continues through adolescence(especially with craniofacial
anomalies, neurologic disorders, obesity)

24
Obstructive Sleep Apnea• due to upper airway collapse
• can be due to:– anatomic factors– abnormal neuromuscular tone– both
• worse in REM sleep
25
OSAS: etiologic factors
• obesity• craniofacial disorders
esp. mid-face hypoplasia• micrognathia
ie. Pierre-Robin• other
-- Crouzon synd -- Aperts synd -- Down synd -- Achondroplasia -- Duchenne’s MD -- cerebral palsy
-- Arnold Chiari malf -- Prader-Willi synd-- hypothyroidism -- choanal stenosis-- sickle cell anemia-- mucopolysaccharidosis
26
Obstructive Sleep Apnea: History
• predominant symptoms-- snoring-- labored breathing-- daytime somnolence-- difficulty in school
• important to ask about snoring, snorting, noisy breathing (gasping, grunting)
• note: parents frequently don’t volunteer this information

27
Other Historical Findings:
• labored breathing, retractions, paradoxical chest wall motion• observed apneas• restless sleep• diaphoresis• enuresis• cyanosis• unusual positions seated or neck hyper-extension• daytime neurobehavioral abnormalities
ADHD or sleepiness• morning headaches from hypercapnia
28
OSA Findings• hypertension
-- systemic
-- pulmonary• failure to thrive• adenoidal facies• nasal obstruction• mouth breathing• hyponasal speech• tongue size• tonsils size• soft palate size and
shape
29
Obstructive Sleep Apnea
• gold standard nocturnal full, observedpolysomnogram (sleep study)• rarely, multiple sleep latency test (MSLT)• other studies much less helpful -- audiotapes
-- nocturnal videotaping-- overnight pulse oximetry-- nap sleep study (1 hr)
• re-testing after T&A essential (~ 6 week post-op)
30
Obstructive Sleep Apnea
• questionaires to 7th and 8th graders• 1,588 questionaires• top 25% [HP] and bottom 25% [LP]• frequent / loud snoring: 5 % HP / 13% LP• Prior tonsillectomy / adenoidectomy:
7 HP / 24 LP (3.4 odds ratio)• Conclusion: children with lower academic
performance ↑ snoring and more likely to require T&A. “A learning debt that may hamper future performance”
Gozal D et al. Pediatrics. 2001; 107(6):1394-1399.
31
Obstructive Sleep Apnea
• 297 first graders in lowest 10th percentile
• sleep studies to assess for sleep-associated gas exchange abnormalities [SAGEA] • SAGEA identified in 54 (18.1%)• encouraged to Rx• 24 underwent T&A [T&A] • in T&A group, improvement by 0.5• no change in non-T&A group & those in top
90th percentile
Gozal D et al. Pediatrics. 1998; 102(3 pt 1):616-620.
32
Obstructive Sleep Apnea
Conclusion:
SAGEA is frequently present in poorly performing 1st grade students in whom it adversely affects learning performance.
The data suggest that a subset. . . could have SAGEA and may benefit from prospective medical evaluation and treatment.
Gozal D et al. Pediatrics. 1998; 102(3 pt 1):616-620.
33
Obstructive Sleep Apnea
• surgical treatment
– adenotonsillectomy
adenoids can reappear– uvulopalatopharyngoplasty (UP3)– rarely tracheostomy– occasional recurrence
• other therapies– CPAP– BiPAP– lifestyle changes (ie. weight loss)

34
Z Z Z Z Z !
Primary Snoring in Children
35
Primary Snoring
• snore – a noise produced when breathing in (vibrates soft
palate and uvula)
• snoring without sleep apneas
• 20% of normal children snore
occasionally
• 7 - 10% snore every night
• OSAS only ~ 2% of snorers
36
Primary Snoring
• differs from primary snoring
• OSAS associated w/ complications• primary snoring – 10% of children– not associated with OSA, arousals, or gas
exchange abnormalities
37
Primary Snoring
• study on 1,144 3rd grade schoolchildren
• snoring shown to be associated with poor academic
performance in math and spelling in 3rd grade school children
Urschitz MS et al. Am J Respir Crit Care Med. 2003.
38
Central apneas
Sudden infant death syndrome (SIDS)

39
Sleepwalking(somnambulism)
40
Somnambulism
• typically pre-pubertal children• highest 11-12 years old (17%)• can last into adulthood• genotyping
• walking or moving during sleep• potential for harm
41
Somnambulism
• difficulty arousing
• can be triggered by sleep disorder
• amnesia following
• first 3rd of sleep episode
• slow wave sleep (stages 3 or 4)
42
Somnambulism
• get plenty of sleep• develop calming bedtime ritual• remove hazardous materials• ground floor if possible• reduce open windows• occasionally hypnosis• benzodiazepines• Topamax?

43
NightTerrors
44
Night Terrors
• sudden arousal from slow wave sleep (stage 3 or 4); 1st third of p.m.• intense terror
cry followed by autonomic changes
• tachycardia• partial or total amnesia• can occur nightly

45
SleepHygiene
46
Sleep Hygiene – habits / behaviors
• stimulantscaffeine: coffee, tea, colas, cocoa, chocolate,
medications
nicotine
• exercise
-- generally helpful-- avoid within 6 hours of bedtime
47
Sleep Hygiene – habits / behaviors
• alcoholslows brain waves initially, but disrupts
sleep later (↓ REM sleep)avoid within 4 – 6 hours of bedtime

48
Sleep Hygiene• environment
comfortable bed, dark & quiet room
mask / earplugs if necessary
minimize changes
• dietheavy meals before disrupts
light snack can help, especially milk and
other dairy products (tryptophan)
49
Sleep Hygiene
• regular schedule
• reduce stress
• avoid long daytime naps
• reduce stimuli
• avoid clock-watching
• designate worry time
50
Sleep Hygiene
• sleep only when drowsy• if unable to sleep, leave
& return when sleepy• maintain regular waking time• limit bedroom activities • avoid / reduce naps – limit to less than 1 hour– no later than 3 p.m.
helpful tips:
51
Signs of problems
• too much time needed to help child fall asleep
• child wakes repeatedly• behavior & mood are affected • parents also lose sleep• parent-child relationship starts to suffer
52
Three common problems
• sleep-onset association disorderie. child requires rocking
• night-time eating / drinking disorderie. frequently awakens for feeds
• limit-setting problemsie. refusing to go to bed or stalling
children can get pretty creative
53
Sleep Hygiene in Children
• bedtime preparation can reduceanxiety
• 10 to 30 minutes of “special time” before bed
• should not be stimulating– ie. no wrestling or scary stories
• don’t extend length of “special time”
54
YAWN FACTS:
-- lasts six seconds-- heart rate ↑ 30%-- 55% yawn within 5 min of seeing someone else-- the blind yawn after hearing someone else-- reading about yawning stimulates yawning-- fetuses yawn-- olympic athletes often yawn before competing
- unknown cause- possible boredom color test bar pattern
5.8 yawns / min “MTV-like” video
3.4 yawns / min

55
THEEND