1 introduction to psychiatric disease and the drugs of experience j. michael mcintosh, m.d....
Post on 21-Dec-2015
213 views
TRANSCRIPT

1
Introduction to Psychiatric Disease
and the Drugs of Experience
J. Michael McIntosh, M.D.
University of Utah

2
Impact
• Mental Illness extracts a enormous toll on the individual.
• Mental Illness places huge burdens on society.
• The study of neuroscience and how behavior influence CNS function will lead to the best treatments and cures.

3
Impact• The World Health Organization indicates that of the top
10 conditions that cause disability worldwide, 5 are mental disorders:
• major depression; schizophrenia; bipolar disorder; alcohol abuse and obsessive compulsive disorder.
• Depression is the leading cause of disability in the world as measured by Years Lived with Disability and the prevalence is increasing.

4
Epidemiology
• Lifetime prevalence of schizophrenia is approximately 1% worldwide.
• Schizophrenia is equally prevalent in men and women.
• The onset is earlier in men, with peak onset at 15-25 years. For women peak onset is 25-35 years. Outcome for female schizophrenics is generally better.

5
Suicide risk
• Suicide risk. About 50% of all patients with schizophrenia attempt suicide at least once. 10-15% of schizophrenic patients died by suicide in a 20 year follow-up period.
• Major risk factors for suicide include the presence of
depressive symptoms, young age and high levels of premorbid functioning (especially a college education).

6
Epidemiology
• A disproportionate number of schizophrenic patients are in the low socio-economic groups.
• Downward drift hypothesis suggests that schizophrenics move into or fail to rise out of a low socio-economic group. Social causation hypothesis proposes that stresses in low socio-economic groups contribute to the development of the disease.
• It is estimated that 50% of homeless people are schizophrenic.

7
Economic Burden
• Financial cost to society. About 1% of the national income goes toward the treatment of mental illness (excluding substance-related disorders).
• Schizophrenia accounts for 2.5% of all health care expenditures. 75% of people with severe schizophrenia are unable to work.

8
Diagnostic criteria for schizophrenia
• Different systems are used. DSM-IV (Diagnostic and Statistical Manual) most commonly used in the United States.
• It is a clinical diagnosis. There are no diagnostic laboratory tests.

9
American Description (DSMIV) Diagnostic Criteria
• Characteristic symptoms: Two (or more) of the following, each present for a significant portion of time during a 1-month period (or less if successfully treated): – delusions – hallucinations – disorganized speech (e.g., frequent derailment or
incoherence) – grossly disorganized or catatonic behavior – negative symptoms, i.e., affective flattening, alogia, or
avolition

10
Three Classes of clinical features.
• Positive symptoms include delusions (false beliefs) hallucinations (false perceptions), and thought disorganization.
• Negative symptoms refer to social withdrawal, diminished affect, poverty of speech, lack of energy, and the inability to experience pleasure.
• Disturbances in basic cognitive functions, such as attention, verbal fluency, executive functions and memory (particularly working memory). In addition, many patients have co-existing mood symptoms including depression and anxiety.

11
Mood Disorders
• Long recognized disorders.
• Depression. Hippocrates (460-357 BC) -“black bile” a state of “aversion to food, despondency, sleeplessness, irritability and restlessness.”

12
Mania
• Aretaeus of Cappadocia (ca. 150 AD) described “mania” “There are infinite forms of mania but the disease is one. If mania is associated with joy, the patient may laugh, play, dance night and day, and go to the market crowned as if victor in some contest of skill. The ideas the patients have are infinite. They believe they are experts in astronomy, philosophy, or poetry.”

13
Manic psychosis
• “The patient may become excitable, suspicious, and irritable; hearing may become sharp…get noises and buzzing the ears; or may have visual hallucinations; bad dreams and his sexual desires may get uncontrollable; aroused to anger, he may become wholly mad and run unrestrainedly, roar aloud; kill his keepers and lay violent hands upon himself.”

14
• DSM-IV (Diagnostic and Statistical Manual) most commonly used in the United States.
• Clinical diagnosis. There are no diagnostic laboratory tests.
• Psychotic features may accompany major depression or bipolar disorder.

15
DSM IV Major Depression
• A) Five (or more) of the following symptoms have been present during the same 2-week period and represent a change from previous functioning; at least one of the symptoms is either (1) depressed mood or (2) loss of interest or pleasure

16
Depression• 1) depressed mood most of the day, nearly every day, as indicated by either
subjective report (e.g., feels sad or empty) or observation made by others (e.g., appears tearful). Note: In children and adolescents, can be irritable mood.2) markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day (as indicated by either subjective account or observation made by others)3) significant weight loss when not dieting or weight gain (e.g., a change of more than 5% of body weight in a month), or decrease or increase in appetite nearly every day. Note: In children, consider failure to make expected weight gains.4) insomnia or hypersomnia nearly every day5) psychomotor agitation or retardation nearly every day (observable by others, not merely subjective feelings of restlessness or being slowed down)6) fatigue or loss of energy nearly every day7) feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) nearly every day (not merely self-reproach or guilt about being sick)8) diminished ability to think or concentrate, or indecisiveness, nearly every day (either by subjective account or as observed by others)9) recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide

17
Mania
• A distinct period of abnormally and persistently elevated, expansive, or irritable mood, lasting at least 1 week (or any duration if hospitalization is necessary).
• During the period of mood disturbance, three (or more) of the following symptoms have persisted (four if the mood is only irritable) and have been present to a significant degree:
– inflated self-esteem or grandiosity – decreased need for sleep (e.g., feels rested after only 3 hours of sleep) – more talkative than usual or pressure to keep talking – flight of ideas or subjective experience that thoughts are racing – distractibility (i.e., attention too easily drawn to unimportant or irrelevant
external stimuli) – increase in goal-directed activity (either socially, at work or school, or sexually)
or psychomotor agitation – excessive involvement in pleasurable activities that have a high potential for
painful consequences (e.g., engaging in unrestrained buying sprees, sexual indiscretions, or foolish business investments)

18
• Sex. Lifetime prevalence of major depression is higher for women than men (10-22% vs. 6-12%).
• Race. Prevalence of mood disorders does not vary significantly by race or ethnicity.
• Trends. Depression has a higher prevalence in younger age groups than in older ones. Hypothesized that birth cohorts born after WWII are at appreciably greater risk for major depressive disorder than older birth cohorts in advanced Western society. The trend has been observed not only in the United States but also in Sweden, Germany, Canada, and New Zealand.

19
Suicide• Each year 30,000 people in U.S. die by suicide. Number of
attempted suicides are 8-10 times that high.
• Depressive disorders account for 80 percent of this figure, schizophrenia accounts for 10 percent.
• Men commit suicide more than three times as often as do women. Women, however, are 4 times more likely to attempt suicide than are men.
• The trends in suicide data among patients with mood disorders parallel the trends in mood disorders (i.e. suicide rates are much higher in younger persons today than they were in younger persons 30 years ago).

20
Etiology
• The etiologies of schizophrenia and mood disorders are unknown.
• They likely represent heterogeneous group of disorders with overlapping clinical symptoms.

21
• Austrian neurologist; founder of psychoanalysis.• Freud was one of the first to infer that mental
disorders could be a result of individual history, and not just physical impairment.
•Sigmund Freud•1856-1939

22
Much of mental life is unconscious.
People like to think they are in control of their lives, but factors outside of conscious awareness
often influence behavior.

23
Sexual Impulses (or more generally, life affirming impulses) Libido (or libidinal energy) is the energy source for this impulse. Basic Life impulses are referred to as needs.
Aggressive Impulse (or more generally, death encouraging impulses) Aggressive energy is the energy source of this impulse.
As an Impulse grows, it becomes more likely that the person will choose an action which will reduce this need.
Freud postulated two basic Impulses:

24
Neurosis: a range of disorders resulting from efforts by a patient to defend himself against becoming aware of threatening (and therefore repressed) feelings, fantasies, and memories.
Psychosis: a range of conditions in which neurotic defenses break down, and the person is “overwhelmed” by the fantasies and needs of his or her unconscious.

25
Many of Freud’s Ideas Now Lampooned

26
Freud’s concept that mental disorders could be a result of individual history, and not just physical impairment remains an important cornerstone of modern psychiatry with increasing molecular evidence.
However,

27
Physical Findings
1. Genetics
2. Neurobiology
3. Role of Experience?

28

29

30
• Monozygotic twins of a patient with a mood disorder have a concordance rate of approximately 60-90%
• Dizygotic twins. 16-35% concordance.

31
Neuropathology of schizophrenia
• Increased size of cerebral ventricles (lateral and 3rd) and decreased brain volume is the most widely replicated finding. Ventricular enlargement is found in affected twins of monozygotic pairs discordant for schizophrenia. This enlargement appears to be stable when patients are followed up prospectively.
• Decreased cortical gray matter especially evident in superior temporal gyrus, dorsal prefrontal cortex and limbic areas such as the hippocampal formation and anterior cingulate cortex. These abnormalities may be present in first-episode, never-medicated patients.

32

33
• Decreased numbers of neurons have been found in the hippocampus and the dorsolateral prefrontal cortex. In studies of monozygotic twins discordant for schizophrenia diminished activation of the dorsolateral prefrontal cortex as measured by SPECT and PET studies is seen.

34
Abnormal dendridic spines in prefrontal cortex- layer 3

35
Specific neuronal circuits involving the thalamus, caudate-putamen, anterior cingulate, limbic and primary auditory cortex, hippocampus and parahippocampal gyrus are activated in schizophrenics during auditory hallucinations.
Hallucinations are real

36
Dopamine antagonists used for treatment of psychosis.

37

38
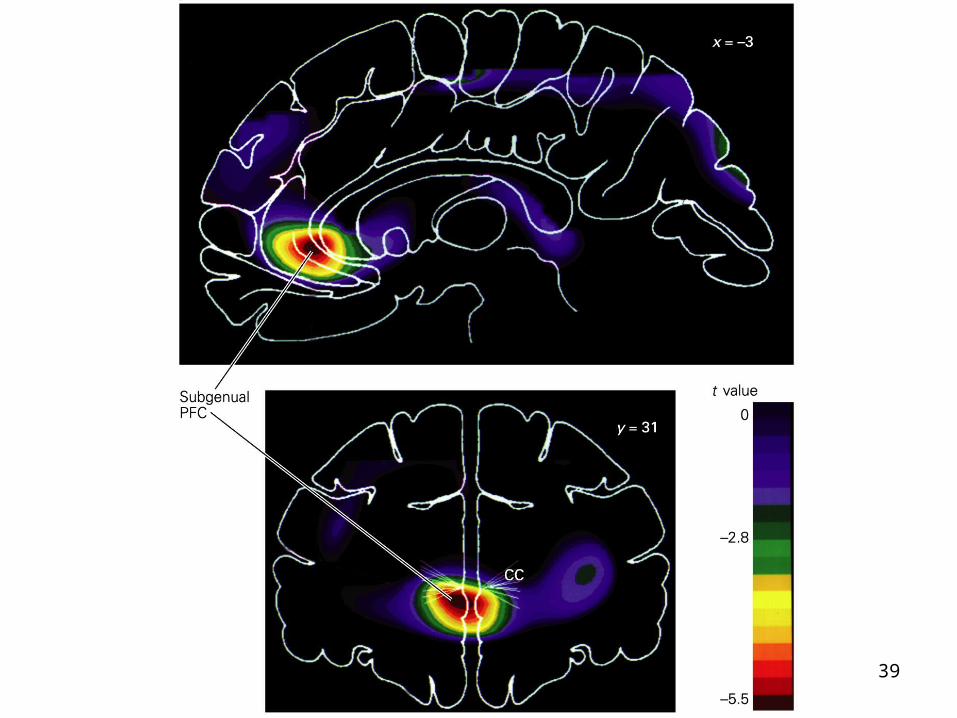
Mood & PET Studies
• The most widely reported finding in depression is decreased anterior brain metabolism, (agranular region of cingulate cortex L>R)
• This abnormality appears to be state dependent and has been observed in both depressive and bipolar disorders.
• There is a reversal in shifts from depression into hypomania.
39

40
• For severe cases of obsessive compulsive disorder (OCD) that are resistant to pharmacotherapy, psychosurgery may be considered as an alternative treatment. In OCD there is an increase in activity in a neuronal circuit running from the frontal cortex to the cingulate gyrus, striatum, globus pallidus, thalamus and back to the frontal cortex. Surgical interruption of this loop by cingulotomy (destruction of 2–3 cm of white matter) at the anterior cingulate cortex disrupts transmission from the frontal cortex and reduces the symptoms of OCD

41
Endogenous Drugs of Experience
• What we experience effects who we are both short term and long term.

42
Placebo Example
Placebo from the Latin “I shall please.”
“It’s all in your head.”

43
Placebo effect varies according to information given the patient.
Can have opposite effects on heart rate, or blood pressure, depending on whether they are given as tranquillizers or as stimulants.
44
• Pain, depression, and Parkinson’s Disease are illnesses where placebo effect can be prominent.

45
Parkinson’s Disease
• Symptoms caused by insufficient dopamine release.

46
• PET studies using 11C raclopride – a dopamine receptor binding molecule.
• Monitor striatum using PET scan.
• Increased release of dopamine levels leads to decreased raclopride binding.
47
Placebo effect
• Amount of change seen with placebo (17-19%) equal to therapeutic doses drugs to treat Parkinson’s.

48
• ½ of patients perceived a benefit.
• All showed binding changes.
• Those who reported effect had greater change (22% vs. 12%).

49
"We are studying the effect of a medication that may or may not relieve pain. This medication is thought to have analgesic effects through the activation of brain systems that suppress pain."
Pain and Placebo

50
Copyright ©2005 Society for Neuroscience
Zubieta, J.-K. et al. J. Neurosci. 2005;25:7754-7762
Effects of pain and placebo on the activation of mu-opioid receptor-mediated neurotransmission

51
Copyright ©2005 Society for Neuroscience
Zubieta, J.-K. et al. J. Neurosci. 2005;25:7754-7762
Figure 3. Relationship between placebo-induced regional {micro}-opioid system activation and expectation of analgesia

52
Implications for psychotherapy
Treatment with Prozac or Behavior Therapy results in similar brain changes.
L.R. Baxter Arch Gen Psychiatry 1992;49:681-689
53
Trust and trustworthiness were operationalized using a paradigm from experimental economics using monetary transfers (a money game).
Subjects were informed that their own decisions and those of the others will determine how much money they leave with.
They are unacquainted with, the other decision makers.
Oxytocin, A Trust Hormone?

54
Ovulating women are also statistically less trustworthy (one-tailed t-test, P >.036), presumably because of the inhibition of OT binding to its receptor by progesterone.
Decision makers who received an intentional trust signal have nearly twice the OT levels as decision makers in the Random Draw condition (F-test, one-tailed, n = 38, P <.004.
PAUL J. ZAK, Ann. N.Y. Acad. Sci. 1032: 224:227 (2004)

55
As a group, the investors who received oxytocin exhibited more trust in the anonymous trustee than did the investors who received the placebo.
Researchers got students to play a serious game. The game involved real monetary exchanges between two people playing the anonymous roles of 'investor' and 'trustee.'
Intranasal administrationof oxytoxin increases human trust.

56
Subjects given oxytocin seem better able to overcome trust obstacles such as betrayal aversion.
The effect of oxytocin on trust is not due to a general increase in the readiness to bear risks.
Oxytocin specifically affects an individual's willingness to accept social risks arising through interpersonal interactions.
Kosfeld M, et al., Nature, 2005 Jun 2;435(7042):673-6

57
(A and B) Affiliative behavior among subordinates can reduce the effects of stress. (A) Chimpanzees engage in social grooming. (B) A female tamarin monkey cares for another's young while the mother feeds. (C and D) Stressful dominance behavior may take physical or psychosocial forms. (C) Male savanna baboons may fight over a kill. (D) A dominant male baboon intimidates a subordinate. R.M. Sapolsky Science 29 April 2005

58
A physical stressor is an external challenge to homeostasis.
A psychosocial stressor is the anticipation, justified or not, that a challenge to homeostasis looms.
Psychosocial stressors typically engender feelings of lack of control and predictability and a sense of lacking outlets for the frustration caused by the stressor.
Both types of stressor activate an array of endocrine and neural adaptations.

59
Physiological correlates of the more stressful social rank.
60
When mobilized in response to an acute physical challenge to homeostasis (such as fleeing a predator), the stress response is adaptive, mobilizing energy to exercising muscle, increasing cardiovascular tone to facilitate the delivery of such energy, and inhibiting unessential anabolism, such as growth, repair, digestion, and reproduction.
Chronic activation of the stress response by chronic psychosocial stressors (such as constant close proximity to an anxiety-provoking member of one's own species) can increase the risk of numerous diseases including psychiatric.
61
1. In some species, rank is lifelong and inherited (for example, in female rhesus monkeys.
2. In contrast, in other species, high-ranking individuals
maintain dominance through psychological intimidation rather than aggression (where, for example, mere eye contact with the alpha individual might elicit subordination gestures).
Subordination as in #2 is associated with the greatest physiological indices, plausibly reflecting the frequent psychological stressors for subordinates and the paucity of physical stressors for dominant individuals.

62
This reflects the high rates of physical and psychological harassment of subordinates, their relative lack of social control and predictability, their need to work harder to obtain food, and their lack of social outlets such as grooming or displacing aggression onto someone more subordinate.
During major hierarchical reorganization, however, dominant individuals at the center of the social tensions
typically experience the greatest amounts of physical and psychological stress. As a result, during such reorganization among wild baboons or soon after group formation among species of captive primates, dominant individuals have the greatest physiological indices of stress.

63
We know that a particular rank gives rise to a particular physiological profile, rather than visa versa, because studies of individual captive animals before they are placed in social groups indicate that physiological profiles of singly-housed subjects do not predict their subsequent ranks in a social group.

64
Several stress-related physiological endpoints have been found to be sensitive to rank.
The most frequently studied endpoint is the blood level of glucocorticoids (GCs), adrenal steroid hormones that are secreted during stress, such as cortisol or hydrocortisone in primates and corticosterone in many rodent species.
GCs typify the double-edged nature of the stress response, as they help mediate adaptation to short-term physical stressors yet are pathogenic when secreted chronically.

65
Animals who are socially stressed by the dominance hierarchy for prolonged periods undergo neurobiological changes.
This can involve inhibition of neurogenesis, dendritic atrophy, and impairment of synaptic plasticity in the hippocampus and altered patterns of apoptotic cell death (increases in the cortex and decreases in the hippocampus) and enhanced benzodiazepine tone.

66
Subjective socioeconomic status (SES) can be at least as
predictive of health as is objective SES.
Feeling poor may be at the core of why being poor predicts poor health.
Schizophrenia is increased with lower SES.
Poverty associated with long -term stress in humans

67
There is evidence from MRI volumetric studies that hippocampal volume is reduced in posttraumatic stress disorder (PTSD or combat-related stress)
The hippocampus may also be affected in chronic depression.

68
Coming up Short
• Some people are more vulnerable to stress.
• 5-HTT- two common forms, long (l) and short (s).
• Mice and Monkeys that are l/l cope better with stress than those that are s/l or s/s.
• Monkeys with s allele that are raised in stressful conditions have impaired serotonin transmission.

69
Humans?
• 847 individuals were assessed with various tests for the past 23 years.
• Assessments were from ages 3 to 26 and included counting major stresses from 21-26.
• At age 26 assessed for whether they had been depressed in the past year.
• 17% reported major depression.

70
• Those with no major stressor had the same risk regardless of allele status (~10%)
• With 4+ life events this rose to 26% for l/l and 43% for s/s.
• Abuse as a child predicted depression after age 18 only in people carrying at least one s allele.

71
50% of Caucasian population carries one copy of s
Caspi et al., 2003, Science, 301:386

72
Child Maltreatment Effects
Caspi et al., 2003, Science, 301:386

73Copyright restrictions may apply.
Kendler, K. S. et al. Arch Gen Psychiatry 2005;62:529-535.
The hazard ratio of onset of major depression within a 2-month period as a result of (1) sex (men vs women), (2) genotype at the 5-HTT polymorphism (SS vs LS and LL), (3) the occurrence, in the
first month, of a stressful life event (SLE) based on 549 twins.

74Copyright restrictions may apply.
Kendler, K. S. et al. Arch Gen Psychiatry 2005;62:529-535.
The hazard ratio of onset of major depression within a 2-month
period as a result of (1) sex (men vs women), (2) genotype at the M polymorphism (SS vs LS and LL),
(3) the level of long-term contextual threat experienced in
the first month.

75
Believe in yourself.
Be a good monkey.
Help our genes