1 diabetic macula edema. microaneurysms cws hard exudates beading of vessels irma nvd/nve ...
TRANSCRIPT

1
Diabetic macula edema

?
Microaneurysms
CWS
Hard exudates
Beading of vessels
IRMA
NVD/NVE
DME- Types
2

Definition of DME
Swelling of the retina due to leaking of fluid from blood vessels within the macula in patients with diabetes
Thickening of the basement membrane and a reduction in the number of pericytes are believed to lead to increased permeability and leakage of plasma constituents in the surrounding retina, resulting in retinal edema
3
http://www.medterms.com/script/main/art.asp?articlekey=16569. Accessed February 2009
4
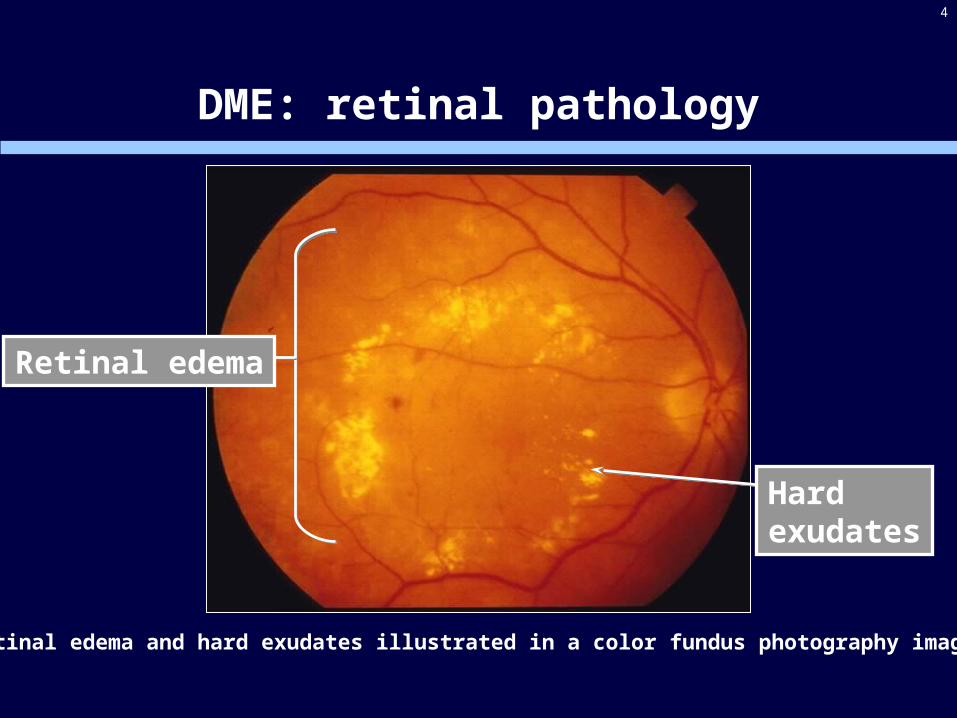
DME: retinal pathology
Retinal edema
Hard exudates
Retinal edema and hard exudates illustrated in a color fundus photography image

5
Factors affecting DME
Incidence of DME increases with
elevated levels of HbA1C
severity of DR
duration of DM
elevated diastolic blood pressure
gender (more frequent in females)
serum lipid levels
Klein et al. Ophthalmology 1998; 105: 1801-1815
6
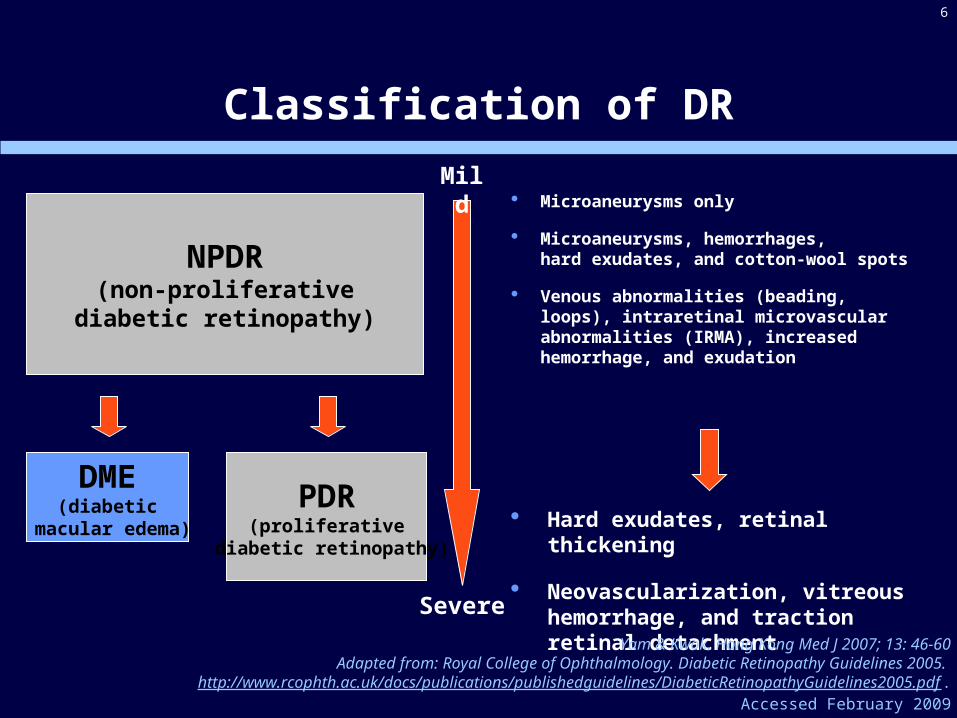
Classification of DR
Microaneurysms only
Microaneurysms, hemorrhages, hard exudates, and cotton-wool spots
Venous abnormalities (beading, loops), intraretinal microvascular abnormalities (IRMA), increased hemorrhage, and exudation
NPDR(non-proliferative
diabetic retinopathy)
PDR(proliferative
diabetic retinopathy)
DME(diabetic
macular edema) Hard exudates, retinal thickening
Neovascularization, vitreous hemorrhage, and traction retinal detachment
Mild
Severe
Yam & Kwok. Hong Kong Med J 2007; 13: 46-60Adapted from: Royal College of Ophthalmology. Diabetic Retinopathy Guidelines 2005.
http://www.rcophth.ac.uk/docs/publications/publishedguidelines/DiabeticRetinopathyGuidelines2005.pdf .Accessed February 2009

7
Most common complications are microvascular changes1
Diabetic macula edema (DME) is a common cause of blindness in people of working age2,3 and can develop in both Type 1 and 2 DM4
About 8% of diabetic patients develop DME with visual impairment5
1King et al. Diabetes Care 1998; 21: 1414-1431; 2Royal College of Ophthalmology. Diabetic Retinopathy Guidelines 2005. http://www.rcophth.ac.uk/docs/publications/publishedguidelines/DiabeticRetinopathyGuidelines2005.pdf . Accessed February
2009; 3Watkins. BMJ 2003; 326: 924-926; 4Klein et al. Ophthalmology 1998; 105: 1801-1815; 5Calculated from: Ling et al. Eye 2002; 16: 140-145; Broadbent et al. Eye 1999; 13: 160-165; Knudsen et al. Br J Ophthalmol 2006; 90: 1404-1409; Hove et al.
Acta Ophthalmol Scand 2004; 82: 443-448; Romero-Aroca et al. Arch Soc Esp Oftalmol 2007; 82: 209-218; Zietz et al. Dtsch Med Wochenschr 2000; 125: 783-788; Kristinsson. Acta Ophthalmol Scand Suppl 1997; 223: 1-76
Diabetes and vision loss

8
Role of VEGF in DR
Vascular endothelial growth factor (VEGF) plays a major role in patients with DR
mediates active intraocular neovascularization and breakdown of the blood-retinal barrier1
associated with VEGF gene polymorphism2
1Aiello et al. N Engl J Med 1994; 331: 1480-14872Nakamura. Graefes Arch Clin Exp Ophthalmol 2009; 247: 21-26

9
VEGF165 in DR
Retinal VEGF165 levels are elevated in experimental diabetes
Increased VEGF165 levels are found in the vitreous of eyes with proliferative DR
Patients with DR have higher VEGF165 levels in the aqueous
Qaum et al. IOVS 2001; 42: 2408-2413; Aiello et al. N Engl J Med 1994; 331: 1480-1487

Diagnosis of DR / DME
Diagnosis of DR / DME often occurs during routine eye examinations of patients with DM
Type 1 diabetes (no DR / DME) first examination 3–5 years after
diagnosis of diabetes, recommended yearly follow-up
Type 2 diabetes (no DR / DME) first examination at time of diagnosis
of diabetes, recommended yearly follow-up
Follow-up frequency increases with diagnosis of DR / DME
10
AAO Guidelines. Diabetic Retinopathy. http://www.aao.org/ppp. Accessed February 2009Royal College of Ophthalmology. Diabetic Retinopathy Guidelines 2005.
http://www.rcophth.ac.uk/docs/publications/publishedguidelines/DiabeticRetinopathyGuidelines2005.pdf. Accessed February 2009. Images: National Eye Institute, National Institutes of Health
Normal vision
DR

11
DME: current treatment
Systemic treatment
glucose control
blood-pressure control
blood-lipid control
multifactorial metabolic interventions
Ocular treatment
laser photocoagulation (standard treatment for DR / DME)
vitrectomy
pharmacologic therapyAAO Guidelines. Diabetic Retinopathy. http://www.aao.org/ppp. Accessed February 2009
Royal College of Ophthalmology. Diabetic Retinopathy Guidelines 2005. http://www.rcophth.ac.uk/docs/publications/publishedguidelines/DiabeticRetinopathyGuidelines2005.pdf . Accessed February 2009

12
Reduction in vessel hyperpermeabilityand leakage in macular edema
DME: aims of therapy
Treatment of neovascularizationin PDR

13
Laser photocoagulation for DME
Standard treatment – helps to slow fluid leakage and reduce the amount of fluid in the retina (macula edema)
Aim of treatment is to stabilize / prevent further vision loss
Limitations of treatment include
does not eliminate possibility of further vision loss
improvement in visual acuity is uncommon
complications including permanent damage to the retinal pigment epithelium and secondary choroidal neovascularization
National Eye Institute, National Institutes of Health. Diabetic Retinopathy. http://www.nei.nih.gov/health/diabetic/retinopathy.asp#4a Accessed February 2009
AAO Guidelines. Diabetic Retinopathy. http://www.aao.org/ppp. Accessed February 2009Royal College of Ophthalmology. Diabetic Retinopathy Guidelines 2005.
http://www.rcophth.ac.uk/docs/publications/publishedguidelines/DiabeticRetinopathyGuidelines2005.pdf . Accessed February 2009

14
DR and DME: the unmet treatment needs
Despite the use of standard interventions for DR, vision loss as a result of the disease still occurs in many patients1
Good metabolic and blood-pressure control are often difficult to achieve in clinical practice, and sight-threatening DR still develops2
Laser treatment is destructive and cannot restore vision loss that has already occurred; it therefore cannot be regarded as an ideal treatment, and there is a need for better-tolerated and less-destructive therapies3
1Comer & Ciulla. Curr Opin Ophthalmol 2004; 15: 508-5182The DIRECT Programme Study Group. J Renin Angiotensin Aldosterone Syst 2002; 3: 255-261
3Fong. Surv Ophthalmol 2002; 47: S238-S245

RESTORE study in DME patients: 12-month results
Core slide resource

Primary objective
To demonstrate superiority of ranibizumab (0.5 mg) as monotherapy and/or adjunctive to laser treatment vs. laser therapy based on the mean average change from baseline in BCVA over a 12-month treatment period

Key secondary objectives
To evaluate whether ranibizumab (0.5 mg) as monotherapy or adjunctive to laser is superior to laser treatment in the proportion of patients with improvement in BCVA
To evaluate ranibizumab (0.5 mg) monotherapy and adjunctive to laser relative to laser treatment with respect to:
the time course of BCVA change
the effects on central retinal thickness (CRT) and other anatomical changes
the effect on patient-reported outcomes
safety

Primary endpoint
The mean average change in BCVA from baseline to Month 1 through Month 12
Mean average change is the mean difference between baseline BCVA and the average BCVA over time (Month 1 to Month 12)

RESTORE study design
Visual impairmentdue to DME(n=345)
Randomised 1:1:1
Ranibizumab 0.5 mg
+ active laser
Ranibizumab 0.5 mg
+ sham laser
Sham Injection+ active laser
Active/sham laser treatment was administered before sham/intravitreal injection on the same day (minimum interval between the two treatments was 30 minutes)

RESTORE treatment schedule
Primary endpoint
sham injection
Laser
(n=111)
0 1 2 3 4 5 6 7 8 9 10 11 12Month 0 1 2 3 4 5 6 7 8 9Month
ranibizumab
Laser
(n=118)
ranibizumab
sham laser
(n=116)
Treatment Initiation phase Continuous/resumed treatment phase
ranibizumab 0.5 mg
ranibizumab 0.5 mg PRN*
laser
laser PRN ≠
* According to pre-defined treatment criteria
≠ According to the judgment of the investigator and in accordance with ETDRS guidelines
2 years extension phase with
open-label ranibizumab 0.5 m
gA
rm 1
Arm
2A
rm 3
Randomized, double-masked, multicenter, laser-controlled Phase III (N=345)
RESTORE

Re-treatment criteria
Ranibizumab:
• monthly ranibizumab/sham injections suspended when:
• No further BCVA improvement due to treatment at 2 last consecutive visits OR
• BCVA >84 letters at 2 last consecutive visits
• monthly ranibizumab/sham injections reinitiated when:
• decrease in BCVA due to DME progression in the opinion of the
investigator
Laser photocoagulation (active or sham):
• in accordance with the ETDRS guidelines at intervals of ≥3 months from the last treatment AND
• if deemed necessary by the evaluating investigator
RESTORE

Key inclusion criteria
Male/female patients >18 years of age
Type 1 or type 2 diabetes mellitus
HbA1C ≤10.0%
Eligibility criteria for study eye:
BCVA score: 78-39 letters
Decrease in vision is due to DME and not due to other causes (based on investigator opinion)
Medication for the management of diabetes stable within 3 months prior to randomization and expected to remain stable during the course of the study
RESTORE

Key exclusion criteria
Ocular disorders of the study eye that may confound interpretation of study results
Systemic conditions such as:
history of stroke
renal failure requiring dialysis or renal transplant or renal insufficiency with creatinine levels > 2.0 mg/dl
untreated diabetes mellitus
blood pressure systolic >160 mmHg or diastolic >100 mmHg, untreated hypertension or change in antihypertensive treatment within 3 months preceding baseline
Treatment with anti-angiogenic drugs (study eye) within 3 months prior to randomization, ocular conditions requiring corticosteroid treatment or laser photocoagulation (study eye) within 6 months prior or during study
RESTORE

Demographic Variable (Randomized set)
Ranibizumab N = 116
Ranibizumab + LaserN=118
LaserN=111
Age (years)
Mean (SD) 62.9 (9.29) 64.0 (8.15) 63.5 (8.81)
Age group (years), n(%)
<55 24 (20.7) 14 (11.9) 13 (11.7)
55 - <65 41 (35.3) 42 (35.6) 53 (47.7)
65 - <75 40 (34.5) 53 (44.9) 31 (27.9)
≥75 11 (9.5) 9 (7.6) 14 (12.6)
Gender, n (%)
Male 73 (62.9) 70 (59.3) 58 (52.3)
Female 43 (37.1) 48 (40.7) 53 (47.7)
Predominant race, n(%)
Caucasian 109 (94.0) 111 (94.1) 106 (95.5)
Others* 7 (6.1) 7 (5.9) 5 (4.5)
Patient demographics
*Others include: Black, Asian, Pacific islander and missing

Characteristics (Randomized set)
Ranibizumab N=116
Ranibizumab + LaserN=118
LaserN=111
Diabetes type, n (%)
Type I 13 (11.2) 15 (12.7) 13 (11.7)
Type II 103 (88.8) 102 (86.4) 97 (87.4)
Not stated 0 1 (0.8) 1 (0.9)
HbA1c (%)
Mean (SD) 7.23 (1.085) 7.50 (1.099) 7.28 (1.105)
HbA1c group, n (%)
<8 84 (72.4) 85 (72.0) 80 (72.1)
8 - 10 30 (25.9) 31 (26.3) 28 (25.2)
>10 0 1 (0.8) 0
Missing 2 (1.7) 1 (0.8) 3 (2.7)
Time since first diagnosis of diabetes (years)
Mean (SD) 15.23 (9.909) 14.62 (9.835) 12.93 (9.024)
Diabetes characteristics at baseline

Mean average change in BCVA from Month 1 through Month 12 compared to baseline (primary endpoint)
Treatment
ranibizumab ranibizumab + laser laser
Me
an
ave
rag
e c
ha
ng
e (
SE
) o
f BC
VA
fr
om
ba
selin
e to
M1
-12
0
2
4
6
8
ranibizumab (n=115)ranibizumab + laser (n=118)laser (n=110)
6.15.9
0.8
p<0.0001*
p<0.0001*
* Differences in LS means and the two-sided 95% CIs are estimated from pair wise ANOVA (stratified) model
Full analysis set/LOCF

Mean change in BCVA from baseline over time
10
Month
0 2 4 6 8 10 12
Me
an
ch
an
ge
(±S
E)
in B
CV
A (
lett
ers
)
-2
0
2
4
6
8
ranibizumab (n=115)
ranibizumab + laser (n=118)
laser (n=110)
1 3 5 7 9 11
Ranibizumab injection
0.9
6.4
6.8
RESTORE
Full analysis set/LOCF

Mean change in CRST from baseline over time
*CRST: central retinal subfield thickness
Month
1 3 5 7 9 11
Ranibizumab injection
0 2 4 6 8 10 12
Mea
n ch
ange
(±S
E)
in C
RS
T (
µm
)
-160
-140
-120
-100
-80
-60
-40
-20
0
20
ranibizumab (n=115) ranibizumab + laser (n=118) laser (n=110)
-61.3
-128.3
-118.7
RESTOREFull analysis set/LOCF

Mean average change in BCVA from baseline over time according to type of DME
Numbers in boxes are mean average change of BCVA from baseline to Months 1-12 (primary endpoint)
Numbers in boxes are mean average change of BCVA from baseline to Months 1-12 (primary endpoint)
FOCAL* DIFFUSE**
0.4
6.8
7.0
5.6
0.6
7.0
Month
0 1 2 3 4 5 6 7 8 9 10 11 12
Me
an
(±S
E)
VA
ch
ang
e
from
bas
elin
e,
lett
ers
-2
0
2
4
6
8
10
ranibizumab (n=63)ranibizumab+laser (n=68)laser (n=52)
Month
0 1 2 3 4 5 6 7 8 9 10 11 12
Me
an
(±S
E)
VA
ch
ang
e
from
ba
selin
e,
lett
ers
-4
-2
0
2
4
6
8
10
ranibizumab (n=45)ranibizumab+laser (n=46)laser (n=52)
RESTORE
* focal (central reading center definition): >67% of leakage originated from leaking microaneurysms in the whole edema area. If around 30-67% leakage comes from microaneurysms, the edema is focal if in the central subfield >67% of the leakage originates from microaneurysms
**diffuse (central reading center definition): <33% of leakage comes from leaking microaneurysms and the rest comes from diffuse leaking capillaries in the whole edema area. If around 30-67% leakage comes from microaneurysms, the edema is diffuse if in the central subfield <33% of the leakage originates from microaneurysms

Mean average change in BCVA from baseline over time according to type of diabetes
TYPE I DIABETES
TYPE II DIABETES
Month
0 2 4 6 8 10 12
Me
an (
±SE
) V
A c
hang
e
from
bas
elin
e, le
tter
s
-1
0
1
2
3
4
5
6
7
8
9
10
11
12
ranibizumab (n=13)ranibizumab+laser (n=15)laser (n=12)
Month
0 1 2 3 4 5 6 7 8 9 10 11 12M
ean
(±S
E)
VA
ch
ange
fr
om
bas
elin
e,
lett
ers
-4
-2
0
2
4
6
8
10
12
ranibizumab (n=102)ranibizumab+laser (n=102)laser (n=96)
2.8
7.7
6.7
0.7
6.2
6.8
Numbers in boxes are mean average change of BCVA from baseline to Months 1-12 (primary endpoint)
Numbers in boxes are mean average change of BCVA from baseline to Months 1-12 (primary endpoint)
RESTORE

Mean average change in BCVA from baseline over time according to prior laser treatment status
WITH PRIOR LASER TREATMENT WITHOUT PRIOR LASER TREATMENT
Month
0 1 2 3 4 5 6 7 8 9 10 11 12
Mea
n (±
SE
) V
A c
hang
e
from
ba
selin
e, le
tter
s
-4
-2
0
2
4
6
8
10
ranibizumab (n=60)ranibizumab+laser (n=55)laser (n=47)
Month
0 1 2 3 4 5 6 7 8 9 10 11 12M
ean
(±S
E)
VA
ch
ange
fr
om b
asel
ine,
lett
ers
-4
-2
0
2
4
6
8
10
ranibizumab (n=55)ranibizumab+laser (n=63)laser (n=63)
1.2
4.5
7.6
0.6
8.0
5.9
Numbers in boxes are mean average change of BCVA from baseline to Months 1-12 (primary endpoint)
Numbers in boxes are mean average change of BCVA from baseline to Months 1-12 (primary endpoint)
RESTORE

Visual functioning questionnaire (VFQ-25): Mean change from baseline at Month 12
Full analysis set/LOCFQoL, quality of life; VFQ-25, Vision Function Questionnaire 25
QoL, quality of life; VFQ-25, Vision Function Questionnaire 25*p <0.05; **p <0.001 versus Laser
*p <0.05; **p <0.001 versus Laser
*
**
*
* *
* *
0
5
10
15
Composite General vision Near activities Distanceactivities
Ranibizumab 0.5 mgRanibizumab 0.5 mg + laserLaser
Mea
n ch
ange
in V
FQ
-25
sco
re f
rom
ba
selin
e to
mon
th 1
2 (±
SE
)
*
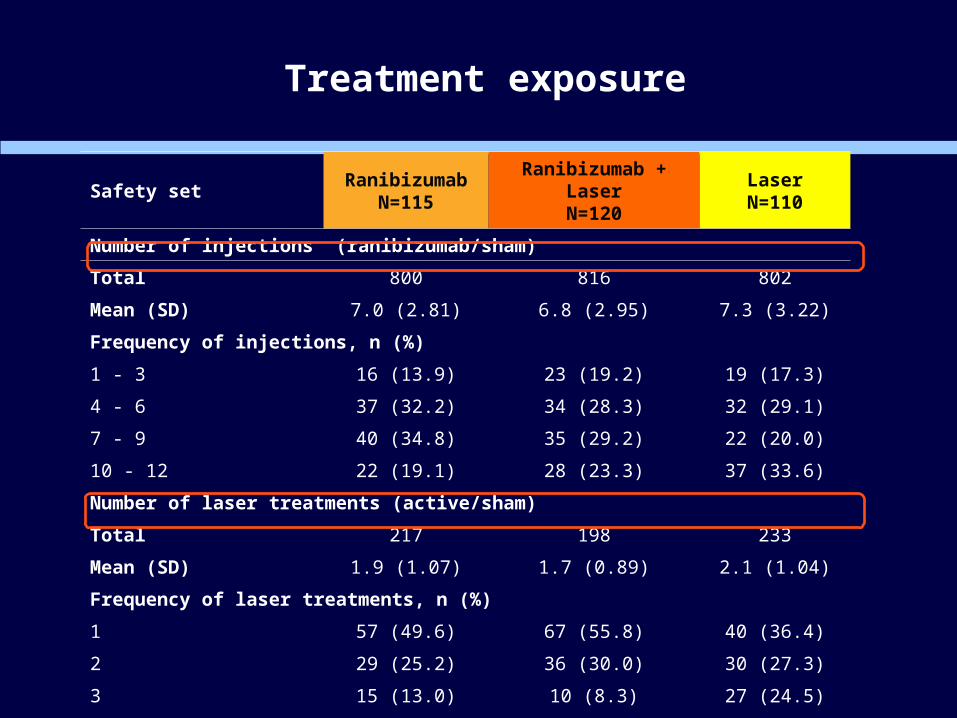
Treatment exposure
Safety setRanibizumab
N=115Ranibizumab + Laser
N=120LaserN=110
Number of injections (ranibizumab/sham)
Total 800 816 802
Mean (SD) 7.0 (2.81) 6.8 (2.95) 7.3 (3.22)
Frequency of injections, n (%)
1 - 3 16 (13.9) 23 (19.2) 19 (17.3)
4 - 6 37 (32.2) 34 (28.3) 32 (29.1)
7 - 9 40 (34.8) 35 (29.2) 22 (20.0)
10 - 12 22 (19.1) 28 (23.3) 37 (33.6)
Number of laser treatments (active/sham)
Total 217 198 233
Mean (SD) 1.9 (1.07) 1.7 (0.89) 2.1 (1.04)
Frequency of laser treatments, n (%)
1 57 (49.6) 67 (55.8) 40 (36.4)
2 29 (25.2) 36 (30.0) 30 (27.3)
3 15 (13.0) 10 (8.3) 27 (24.5)
≥ 4 14 (12.2) 7 (5.8) 13 (11.8)

Proportion of patients receiving injections over time
Month
Day 1 1 2 3 4 5 6 7 8 9 10 11
Pe
rce
nta
ge
of p
atie
nts
re
ce
ivin
g tre
atm
en
t (%
)
0
20
40
60
80
100
ranibizumab (n=115)ranibizumab+laser (n=120)laser (n=110)
Safety set

Summary of ocular adverse events (AEs)
Main AEs
eye pain (8.3-11.3%)
conjunctival hyperemia (5.0-7.8%)
conjunctival hemorrhage (0-8.3%)
Low level of intra-ocular pressure (IOP) increased (<1%)
Suspected to be related to study drug and/or ocular injection:
eye pain (8.3-10.4%)
conjunctival hyperemia (3.3-7.0%)
conjunctival hemorrhage (0-7.5%)
RESTORE

Summary of ocular serious adverse events (SAEs)
No ocular SAEs were reported in the ranibizumab monotherapy arm
Ocular SAEs reported in two patients each in the ranibizumab + laser and laser arms (one patient in the laser arm reported both cataract and maculopathy)
No cases of endophthalmitis were reported in any of the treatment arms
None of the ocular SAEs were suspected to be related to study drug and/or ocular injection
RESTORE
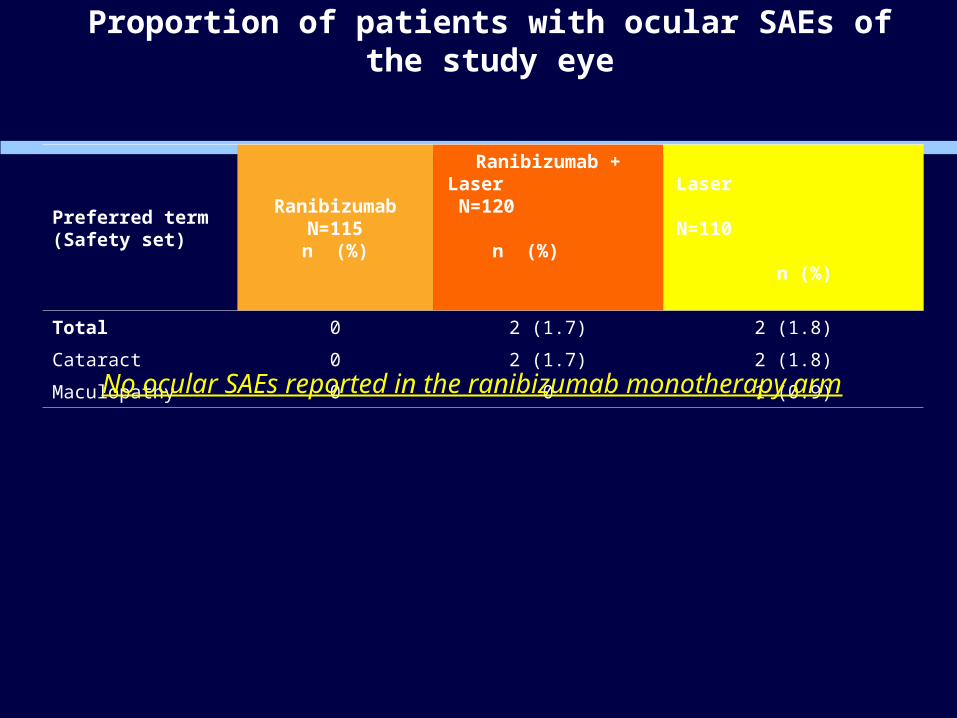
Proportion of patients with ocular SAEs of the study eye
Preferred term (Safety set)
RanibizumabN=115n (%)
Ranibizumab + Laser N=120 n (%)
Laser N=110
n (%)
Total 0 2 (1.7) 2 (1.8)
Cataract 0 2 (1.7) 2 (1.8)
Maculopathy 0 0 1 (0.9)
No ocular SAEs reported in the ranibizumab monotherapy arm

Summary of non-ocular SAEs (per system organ class)
Non-ocular SAEs with incidence rates >1% were low
cardiac disorders (3.3-7.0%)
infections and infestations (2.5-5.2%)
metabolism and nutrition disorders (1.7-3.5%)
Suspected to be related to study drug and/or ocular injection:
3 patients in ranibizumab arm (intestinal obstruction, hypoglycemia, pulmonary embolism, dyspnea, arterial thrombosis limb) and
1 patient in ranibizumab+laser arm (coronary artery occlusion)
Two deaths reported in each treatment arm, none suspected to be related to the study drug and/or injection procedure
RESTORE

Proportion of patients with AEs potentially related to systemic VEGF inhibition
Preferred term (Safety set)
RanibizumabN=115n (%)
Ranibizumab + LaserN=120n (%)
LaserN=110n (%)
Arterial thromboembolic events* 4 (3.5) 4 (3.3) 3 (2.7) Arterial thrombosis limb 1 0 0 Carotid artery stenosis 1 1 1 Cerebral artery embolism 1 0 0 Cerebrovascular accident 1 0 0 Cerebrovascular disorder 0 1 0 Coronary artery occlusion 0 1 1 Myocardial infarction 1 1 0 Peripheral arterial occlusive disease 1 0 1 Vertebrobasilar insufficiency 0 1 0
Venous thromboembolic events* 2 (1.7) 0 2 (1.8) Axillary vein thrombosis 0 0 1 Deep vein thrombosis 0 0 1 Pulmonary embolism 2 0 1
Hypertension 9 (7.8) 6 (5.0) 9 (8.2)
Non-ocular haemorrhage 1 (0.9) 0 1 (0.9)
Epistaxis 1 (0.9) 0 1 (0.9)
Proteinuria 1 (0.9) 1 (0.8) 0* ATEs by defined RMP version 6 “identified risks”
RESTORE

Summary
The primary objective of the study was met with statistically significant superiority of ranibizumab 0.5 mg monotherapy and ranibizumab 0.5 mg adjunctive to laser compared to laser alone with BCVA improvement from baseline to Month 1 through Month 12 of 5.4 and 4.9 letters, respectively
In contrast to laser monotherapy, ranibizumab alone or in combination with laser leads to a rapid and continuous VA improvement within the initial 3 months followed by VA stabilization under PRN treatment
Patients received on average 6.8-7.3 ranibizumab/sham injections and 1.7-2.1 laser (active or sham) treatments in all treatment arms
No new ocular or non-ocular safety risks were identified

Conclusions - Efficacy
Ranibizumab monotherapy or as adjunctive therapy to laser photocoagulation provided superior benefits in BCVA improvement as compared to laser monotherapy at Month 12 (primary endpoint met)
The study shows that 37-43% of ranibizumab-treated patients improved vision by 10 letters or more as compared to 16% with standard laser therapy
Ranibizumab given alone or as adjunctive to laser showed rapid mean average BCVA gain which was sustained over 12 months of treatment at around 6 letters above baseline compared to 0.8 letter with laser therapy alone
Ranibizumab was well tolerated as monotherapy or as adjunctive to laser therapy in patients with visual impairment due to DME
no cases of endophthalmitis
ranibizumab showed low incidence (<1%) of IOP increased
systemic safety: low incidence of hypertension (5.0-8.2%) and ATEs (2.7-3.5%) in all treatment groups
Conclusions - Safety

TURKEYProf. Dr. Bora EldemAssoc.Prof.Dr Ziya KapranProf. Dr. Cezmi AkkinProf. Dr. Mehmet ErginDr Berati Hasanreisoglu
BELGIUMDr Joachim Van CalsterDr. Marlene Devriendt
FRANCEDr Pascale MASSIN
Dr. Jean- Paul RomanetPr. Michel Weber
Pr Catherine Creuzot-Garche
GERMANYProf. Dr. Antonia JoussenProf. Dr. med. Karl-Heinz EmmerichProf. Dr. med.Katrin EngelmannProf. Dr. med. Lutz HansenProf. Dr. med. Helmut HoehProf. Dr. med. Frank HolzProf. Dr. med. Anselm KampikProf. Dr. med. Ulrich KellnerProf. Dr. med. Bernd KirchhofProf. Dr. med. Gabriele LangProf. Dr. med. Andreas MohrDr. med. Georg SpitalProf. Dr. med. Peter WiedemannProf. Dr. med. Salvatore GrisantiProf. Dr. med. Norbert Schrage
GREECEProf. Miltiadis TsilibarisAssoc. Prof. Periklis BrazitikosAss. Prof. Vergados IoaanisProf Stavros DimitrakosDr Stamatina Kabanarou
ITALYProf. F. BandelloProf. Ugo MenchiniProf. Carlo SborgiaProf. Alfredo ReibaldiProf. Emilio BalestrazziDr.ssa Anna TarantiniProf. Nicola Delle Noci
NETHERLANDSProf. Dr. R.O. SchlingemannDr. J.P. Martinez CirianoDr. B.J. Kleverling
SPAINDr. Josep Garcia ArumiDr. Francisco Gomez UllaDr. Ramon Torres ImazDr. Enrique CerveraDr. Alfredo Adan CiveraDr. Jose Ruiz Moreno
SWITZERLANDDr. med. Malaika Kurz-LevinProf. Dr. med Ulrike SchneiderProf. Dr. med. Justus GarwegDr. med. Christoph TappeinerProf. Dr. med Heinrich GerdingDr. med. Patrik Kloos
UKDr Nicholas BeareDr. Geeta MenonDr Clare Bailey
HUNGARYDr. Andras PappDr. Andras SeresDr Andras BertaDr. Árpád BereckiDr Ágnes Kerény
List of PIs in RESTORE study Slide 1/2

AUSTRALIAProf. Paul MitchellA/Prof Mark GilliesA/Prof Tien WongDr Brendan VoteDr. Dianne Sharp
CANADADr John GonderDr Peter KertesDr David MaberleyDr Shelley BoydDr Sébastien OlivierDr Vladimir KozousekDr. John Chen
List of PIs in RESTORE study
RESTORE
Slide 2/2

Primary and secondary BCVA endpoints: subset of RESTORE (Baseline VA ≤73 letters, CRT ≥300 μm) vs RESOLVE
Primary endpoint: Mean average change in BCVA from baseline to Month 1 through Month 12
Ranibizumab
(n=80)
Ranibizumab+laser
(n=81)
Laser
(n=75)
RESOLVE
(n=102)
7.4 7.2 1.4 7.6
Secondary endpoint: Mean change in BCVA from baseline at Month 12
Ranibizumab Ranibizumab+laser Laser RESOLVE
8.4 8.0 1.7 10.3
RESTORE

Treatment regimen concepts / hypotheses
Treatment is individualized
No relevant increase in efficacy upon further treatment in patients who had become stable for at least three consecutive months under ranibizumab treatment
Treatment
Starts and continues until stability of disease
Interruption when disease stabilises
Monitor for disease activity on monthly basis
Restart when disease activity is observed
Continue until disease stability is observed

The Diabetic Retinopathy Clinical Research Network
Randomized Trial Evaluating Ranibizumab Plus Prompt or Deferred Laser or Triamcinolone Plus Prompt Laser for
Diabetic Macular Edema
Supported through a cooperative agreement from the National Eye Institute and the National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Department of Health and Human Services EY14231,
EY14229, EY018817
47

48
Study DesignStudy Design
Primary outcome: Change in visual acuity from baseline to 1 year (intent to treat analysis)
Randomized, multi-center clinical trial
At least one eye meeting all of the following criteria:• Electronic-ETDRS© best corrected visual acuity
letter score of 78 to 24 (~20/32 to 20/320)• Definite retinal thickening due to diabetic macular
edema involving the center of the macula on clinical examination
• Central subfield (Stratus OCT™) ≥250 µm

Follow-up Schedule
49
Baseline to 1 Year
1 Year to 3 Years
• Every subject has a follow-up visit at 1 year• Follow-up every 4 weeks• All groups except ranibizumab plus deferred
laser group: Additional follow-up visit occurs 3 to 10 days after injection if focal/grid laser also is to be given
• Every subject has a follow-up visit at 2 years• Follow-up every 4 to 16 weeks depending on
treatment group, disease progression, and treatment administered
• Triamcinolone plus prompt laser group only: Additional safety visit every 4 weeks after triamcinolone injection
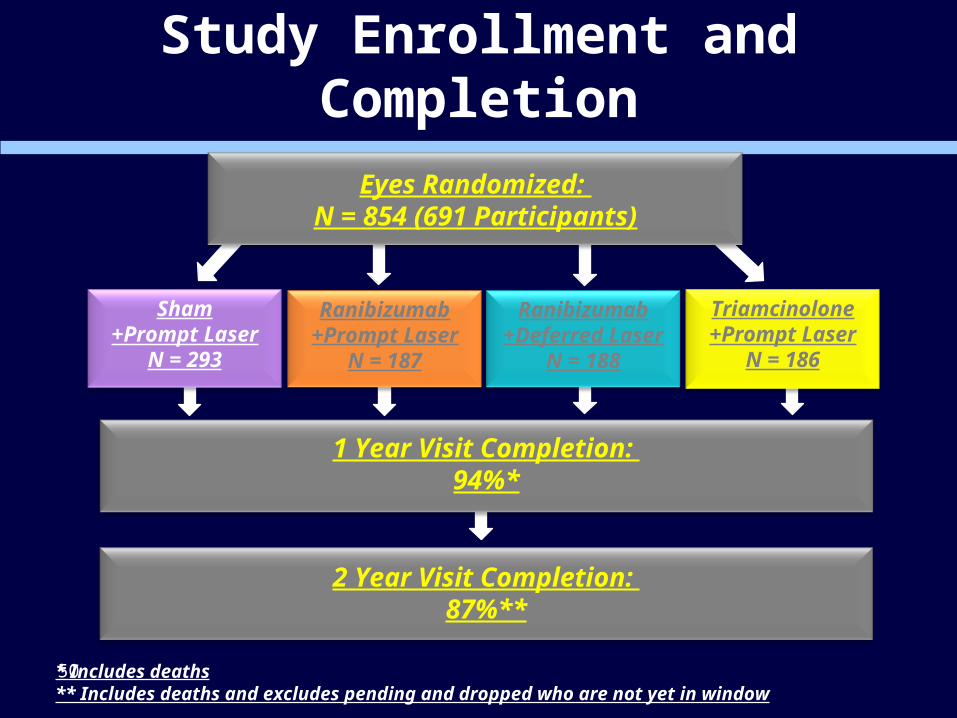
Study Enrollment and Completion
50
Ranibizumab+Prompt Laser
N = 187
Ranibizumab+Deferred Laser
N = 188
Sham+Prompt Laser
N = 293
Triamcinolone+Prompt Laser
N = 186
Eyes Randomized: N = 854 (691 Participants)
1 Year Visit Completion: 94%*
2 Year Visit Completion: 87%**
* Includes deaths** Includes deaths and excludes pending and dropped who are not yet in window

51
Baseline CharacteristicsBaseline CharacteristicsSham
+Prompt
Laser
Ranibizumab
+Prompt
Laser
Ranibizumab
+Deferred
Laser
Triamcinolone
+Prompt
Laser
Median age 63 62 64 62
Diabetes type
Type I 9% 6% 8% 8%
Type II 89% 92% 90% 89%
Uncertain 3% 2% 2% 3%
Median E-ETDRS©
visual acuity letter score (Snellen equivalent)
65 (20/50) 66 (20/50) 66 (20/50) 66 (20/50)
Median OCT CSF thickness (µm) 407 371 382 374

52
Injections/Sham Prior to 1 YearInjections/Sham Prior to 1 YearSham
+Prompt
Laser
N = 274
Ranibizumab
+Prompt
Laser
N = 171
Ranibizumab
+Deferred
Laser
N = 178
Triamcinolone
+Prompt
Laser
N =176
Maximal possible # of sham/injections 13 sham* 13 drug 13 drug 9 sham/4 drug
Median number of sham/study drug injections to 1 year
11* 8 9 5 sham/3 drug
AE Precluding Study Drug Injection† NA 2% 2% 15%
Compliance with sham/drug injection when required by protocol
96% 95% 97% 97%
Masked participant with 1 study eye identified correct assignment at 1 year
10% 88% 90% 44%
*Excludes 56 eyes among 163 participants with 2 study eyes unmasked at baseline when assigned ranibizumab + deferred laser. † % of visits reported; 12% of eyes in the triamcinolone group compared with 3% and 4% in the ranibizumab groups

53
Laser Treatments Prior to 1 YearLaser Treatments Prior to 1 Year
Sham
+Prompt
Laser
Ranibizumab
+Prompt
Laser
Ranibizumab
+Deferred
Laser*
(permitted starting at 24-
week visit)
Triamcinolone
+Prompt
Laser
Median number of laser treatments including baseline
3 2 0 2
Proportion of eyes receiving laser at 48-week visit
26% 16% 8% 21%
No, only 1, only 2 or 3 more lasers after baseline
13%, 27%, 31%, 32%, 70%, 20%, 26%, 30%,
40%, 20% 27%, 11% 10%, 1% 28%, 15%
* 3 eyes deviated from the protocol and received laser prior to 24 weeks (2 were given laser at the 1 week safety visit and 1 at the 20 week visit).

54
Sham
+Prompt
Laser
N = 293
Ranibizumab
+Prompt
Laser
N = 187
Ranibizumab
+Deferred Laser
N = 188
Triamcinolone
+Prompt
Laser
N = 186
Eyes with alternative treatments(number of treatments)
14 (25) 1 (1) 0 1 (1)
Per protocol (failure‡ criteria met) 5 1 0 1
Deviations from protocol - clinical care
9 0 0 0
Alternative* Treatments Prior to 1 YearAlternative* Treatments Prior to 1 Year
*Alternative treatments include: intravitreal bevacizumab, intreavitreal triamcinolone acetonide, vitrectomy, and intravitreal bevacizumab + intravitreal triamcinolone.‡Failure is defined as: ≥10 letter loss from baseline, OCT CSF ≥250 µm, DME present on clinical exam that is cause of visual loss, “complete laser” given AND ≥13 weeks since last laser treatment with no improvement since the last laser treatment

Visual Acuity
55

Mean Change in Visual Acuity* at Follow-up Visits
56* Values that were ±30 letters were assigned a value of 30P-values for difference in mean change in visual acuity from sham+prompt laser at the 52-week visit: ranibizumab+prompt laser <0.001; ranibizumab+deferred laser <0.001; and triamcinolone+prompt laser=0.31.

Change in Visual Acuity (LOCF) at 1 Year*
57
Change in Visual Acuity (letters)
Sham
+Prompt
Laser
N = 293
Ranibizumab
+Prompt
Laser
N = 187
Ranibizumab
+Deferred
Laser
N = 188
Triamcinolone
+Prompt
Laser
N = 186
Mean +3 +9 +9 +4
Difference in mean change from Sham +Prompt Laser
[P Value]**
+5.8[P<0.001]
+6.0 [P<0.001]
+1.1[P = 0.31]
*Visits occurring between 308 and 420 days from randomization were included as 1-year visits. When more than 1 visit occurred in this window, data from the visit closest to the 1-year target date were used. For other eyes with out any 1-year data (19 eyes in the sham+prompt laser group, 16 eyes in the ranibizumab+prompt laser group, 10 eyes in the ranibizumab+deferred laser group, and 10 eyes in the triamcinolone+prompt laser group) the last observation carried forward (LOCF) method was used to impute data for the primary analysis.**Analysis of covariance adjusted for correlation between 2 study eyes and baseline visual acuity

Change in Visual Acuity at 2 Years*
58
Change in Visual Acuity (letters)
Sham
+Prompt
Laser
N = 163
Ranibizumab
+Prompt
Laser
N = 106
Ranibizumab
+Deferred
Laser
N = 112
Triamcinolone
+Prompt
Laser
N = 103
Mean +2 +7 +10 0
Difference in mean change from Sham +Prompt Laser
[P Value]**+5.0
[P = 0.01]+7.2
[P<0.001]-1.6
[P = 0.43]
*Visits occurring between 616 and 840 days from randomization were included as 2-year visits**Analysis of covariance adjusted for correlation between 2 study eyes and baseline visual acuity

Visual AcuitySubgroup Analyses
59

Change in Visual Acuity at 1 Year Stratified by Baseline Visual Acuity
60
N=146

Change in Visual Acuity at 1 Year Stratified by Baseline CSF
61

Change in Visual Acuity at 1 Year Stratified by Prior DME Treatment
62

Change in Visual Acuity at 1 Year Stratified by Number of Study Eyes
63
N=130

Change in Visual Acuity (LOCF) at 1 Year Stratified by Eyes with Diffuse vs. Focal Edema at Baseline as
Graded by Study Ophthalmologist
64

Change in Visual Acuity at 1 Year Stratified by Pseudophakic at Baseline
65

Mean Change in Visual Acuity at Follow-up Visits among Eyes that were
Pseudophakic at Baseline*
66
Visit Week
* Values that were ±30 letters were assigned a value of 30

Retinal Thickening
67

Mean Change in Central Subfield Thickening at Follow-up Visits
68
Visit Week
P values are for the difference in mean change in OCT CSF retinal thickness from sham+prompt laser at the 52-week visit: ranibizumab+prompt laser <0.001, ranibizumab+deferred laser <0.001, and triamcinolone+prompt laser <0.001.

Change in Retinal Thickening at 1 Year*
69
Change in OCT Central Subfield Thickeninga
Sham
+Prompt Laser
N = 271
Ranibizumab
+Prompt Laser
N = 171
Ranibizumab
+Deferred Laser
N = 175
Triamcinolone
+Prompt Laser
N = 173
Mean change from baseline (µm) -102 -131 -137 -127
Difference in mean change from Sham Prompt+Laser
[P Value]**
-55[P<0.001]
-49[P<0.001]
-52[P<0.001]
Thickness <250 µm with at least a 25 µm decrease from baseline
27% 53% 42% 47%
*Visits occurring between 308 and 420 days from randomization were included as 1 year visits. When more than 1 visit occurred in this window, data from the visit closest to the 1 year target date were used. **Analysis of covariance adjusted for baseline OCT retinal thickness and visual acuity and correlation between 2 study eyes
a Missing data for 22 eyes in the sham+prompt laser group, 16 eyes in the ranibizumab+prompt laser group, 13 in the ranibizumab+deferred Laser, and 13 eyes in the triamcinolone+prompt laser group (includes missing and ungradeable data [3 in sham+prompt laser, 2 in ranibizumab+deferred laser and 2 in triamcinolone+prompt laser]

Change in Retinal Thickening at 2 Years*
70
Change in OCT Central Subfield Thickeninga
Sham
+Prompt Laser
N = 152
Ranibizumab
+Prompt Laser
N = 99
Ranibizumab
+Deferred Laser
N = 100
Triamcinolone
+Prompt
Laser
N = 93
Mean change from baseline (µm) -133 -144 -170 -95
Difference in mean change from Sham + Laser [P Value]**
-31[P = 0.01]
-36[P = 0.004]
-3[P = 0.81]
Thickness <250 µm with at least a 25 µm decrease from baseline
38% 54% 55% 44%
*Visits occurring between 616 and 840 days from randomization were included as 2-year visits. When more than 1 visit occurred in this window, data from the visit closest to the 2-year target date were used. ** Analysis of covariance adjusted for baseline OCT retinal thickness and visual acuity and correlation between 2 study eyesª Excluding pending- Missing data for 2 eyes in the sham+prompt laser group, 2 eyes in the ranibizumab+prompt laser group, 2 in the ranibizumab +deferred laser, and 6 eyes in the triamcinolone+prompt laser group; Ungradeable data for 1 in the ranibizumab+prompt laser, 1 in ranibizumab+deferred laser and 2 in triamcinolone+prompt laser

Retinopathy
71

Retinopathy Progression During 1 Year of Follow-up
72
Sham
N = 293
Ranibizumab
N = 375
Triamcinolone
N = 186
Reported vitreous hemorrhage OR received PRP
8% 3% 3%
P Value for comparison with sham -- 0.002 0.02

Safety
73

74
Major Ocular Adverse Events During 2-Years of Follow-up
74
Sham
+Prompt Laser
N = 293
Ranibizumab
+Prompt Laser
N = 187
Ranibizumab
+Deferred Laser
N = 188
Triamcinolone
+Prompt Laser
N = 186
Number of injections 1833 2140 685
Endophthalmitis* 1 (<1%) 2 (1%) 2 (1%) 0
Pseudoendophthalmitis† 1(<1%) 0 0 1 (1%)
Ocular vascular event‡ 1 (<1%) 1 (1%) 1 (1%) 3 (2%)
Retinal detachment§ 0 0 1 (1%) 0
Vitrectomy 15 (5%) 4 (2%) 7 (4%) 2 (1%)
Vitreous Hemorrhage 27 (9%) 6 (3%) 8 (4%) 7 (4%)*One case unrelated to study drug injection (following cataract extraction) in the sham+prompt laser group; 1 case related to study drug injection and 1 case unrelated to injection (following cataract surgery) in the ranibizumab+prompt laser group; 2 cases related to study drug injection in the ranibizumab+deferred laser group. The 3 cases related to study drug injection in the ranibizumab groups are 0.08% of ranibizumab study drug injections given. † One case unrelated to the study drug injection (vitreous opacity with hypopyon) and one case related to study drug injection in the triamcinolone group. ‡ Includes 2 central retinal vein occlusions and 4 branch retinal vein occlusions. §Includes 1 traction retinal detachment with proliferative diabetic retinopathy and prior panretinal photocoagulation at baseline.

75
Elevated Intraocular Pressure/Glaucoma During 2-Years of Follow-up
75
Elevated Intraocular Pressure/Glaucoma
Sham
+Prompt
Laser
N = 293
Ranibizumab +Prompt Laser
N = 187
Ranibizumab
+Deferred Laser
N = 188
Triamcinolone +Prompt Laser
N = 186
Increase ≥10 mmHg from baseline 8% 9% 6% 42%
IOP ≥30 mmHg 3% 2% 3% 27%
Initiation of IOP-lowering meds at any visit*
5% 5% 3% 28%
Number of eyes meeting ≥1 of the above
11% 11% 7% 50%
Glaucoma surgery** <1% 1% 0 1%
*Excludes eyes with IOP lowering medications at baseline**Includes 2 filter and 2 cilliary body destruction

76
Cataract Surgery During 2-Years of Follow-up
76
Sham
+Prompt
Laser
Ranibizumab
+Prompt
Laser
Ranibizumab
+Deferred Laser
Triamcinolone
+Prompt Laser
Phakic at baseline
N = 192 N = 131 N = 134 N = 124
Eyes that had cataract surgery
12% 12% 13% 55%

Number of Deaths
77
Sham
N = 130
Ranibizumab
N = 375
Triamcinolone
N = 186
Deaths* 7 (5%) 15 (4%) 6 (3%)
*Study participants with 2 study eyes are counted in their injection group.

78
Cardiovascular or Cerebrovascular Events According to Antiplatelet Trialists’ Collaboration
through 2-Years
78
Sham‡
N* = 130
Ranibizumab
N* = 375
Triamcinolone
N* = 186
Non-fatal myocardial infarction 3% 1% 3%
Non-fatal cerebrovascular accident-ischemic or hemorrhagic (or unknown)
6% 2% 2%
Vascular death (from any potential vascular or unknown cause†)
5% 2% 2%
Any APTC event 12% 5% 6%
* N=Number of Study Participants. Study participants with 2 study eyes are assigned to the non-sham group. Multiple events within a study participant are only counted once per event.‡One participant had a non-fatal myocardial infarction and a non-fatal stroke (only counted once in the any cardiovascular event row)†Four of the vascular deaths in the sham group, 1 of the vascular deaths in the ranibizumab group, and 1 of the vascular deaths in the triamcinolone group were from an unknown cause

Discussion
79

80
Intravitreal Ranibizumab Summary
Intravitreal ranibizumab with prompt or deferred (≥24 weeks) focal/grid laser had superior VA and OCT outcomes compared with focal/grid laser treatment alone.
• ~50% of eyes had substantial improvement (≥10 letters) while ~30% gained ≥15 letters
• Results were similar whether focal/grid laser was given starting with the first injection or it was deferred >24 weeks
80

81
Intravitreal Ranibizumab Summary
If ranibizumab is to be given as it was in this study, the data indicate a need to follow eyes continuously undergoing this treatment
• Additional ranibizumab and/or laser were needed in most eyes through ≥2 years, even if ‘success’ criteria were met early in the course of treatment.
81

82
Intravitreal Triamcinolone Summary
Intravitreal triamcinolone combined with focal/grid laser did not result in superior VA outcomes compared with laser alone.
Intravitreal triamcinolone did result in a greater reduction in retinal thickening at 1 year but not 2 years compared with laser alone.
In an analysis limited to pseudophakic eyes, the triamcinolone group’s outcome for VA appeared to be of similar magnitude to that of the 2 ranibizumab groups.
82

83
Intravitreal Triamcinolone Conclusion
In pseudophakic eyes, intravitreal triamcinolone with prompt focal/grid laser may be equally effective as ranibizumab at improving visual acuity and reducing retinal thickening, but is associated with an increased risk of intraocular pressure elevation.
83

Thank You on Behalf of Diabetic Retinopathy Clinical Research Network (DRCR.net)
84
52 clinical study sites

RESOLVE: Study Purpose and Population
Phase II study to evaluate the safety and explore the effect of ranibizumab in patients with diabetic macular edema (DME) with center involvement
Study parts and population
Group A: Pilot 42 patients analyzed in the 6-month interim analysis
Group B: Confirmatory* 109 patients not analyzed at interim
Group A+B (all patients): primarily safety and overall efficacy
*Clinical Trial Protocol Amendment 3 released May 29, 2008

RESOLVE: Study Objectives and Endpoints
Primary endpoints
Group A: demonstrate superiority of ranibizumab to non-treatment in reducing macular edema from baseline to Month 6 in DME
Group B: confirm the efficacy of ranibizumab on visual acuity (VA) as mean average change from baseline to Month 1 through Month 12 in best-corrected VA (BCVA)
Secondary endpoints
explore the treatment effect on VA, retinal structure, and need for laser photocoagulation
explore the superiority of ranibizumab effect on macular edema compared with sham

RESOLVE: Trial DesignRESOLVE: Trial Design
FA, fluorescein angiography OCT, optical coherence tomography
Randomized 1:1:1
Sham
Baseline fundus photograph, FA and OCT(reading center)
Investigator identifies potential DME patients
Photocoagulation after 3 injections if needed
Assessment if “increase” is needed
Increase to 0.6 mg if needed
Ranibizumab 0.3 mg
Ranibizumab0.5 mg
Increase to 1.0 mg if needed
N = 151

Key Inclusion Criteria
Male / female patients >18 years of age
Patients with type 1 or type 2 diabetes mellitus
HbA1C ≤ 12.0%
Patients with DME with center involvement in at least one eye (focal or diffuse)
Eligibility criteria for the study eye at Visit 1:
► Central macular thickness must be ≥300 µm in the center subfield, as assessed by optical coherence tomography (OCT) and confirmed by the central reading center
► BCVA letter score between 73 and 39

RESOLVE Treatment Dosing Schedule
Month*
Ranibizumab10 mg/ml
Sham
0
Ranibizumab6 mg/ml
12
Primary endpoint
21
Dose may be doubled from 0.5 mg to 1.0 mg after 1 mo if indicated
Dose may be doubled from 0.3 mg to 0.6 mg after 1 mo if indicated
3 4 5 6 7 8 9 10 11
*Months 3-12 treatment on demand based on success, futility, and safety criteria

Treatment Adjustments: Dose Doubling* Criteria
Retinal thickness in the study eye remains >300 µm at the Month 1 visit following baseline injection
or
Retinal thickness in the study eye is >225 µm and a reduction in retinal edema from the previous assessment is <50 µm, at any monthly visit after Month 1 following the baseline injection
*By doubling the injection volume from 50 to 100 μl ywo formulations of 6 mg/ml and 10 mg/ml have been used
1. Kvanta et al., Invest Ophthalmol Vis Sci 1996; 37: 1929-1934.2. Jonas JB, Neumaier M. Ophthalmic Res 2007, 39: 139-142.

Treatment Adjustments:
Success and Re-initiation Criteria
Discontinuation because of success if:
Retinal thickness in the study eye is ≤225 µm
and
BCVA is ≥79 letters (≥20/25)
at any visit following the third injection
Re-initiation of treatment if:
Retinal thickness increases by ≥50 μm
or
Visual acuity decreases by ≥5 letters and is <74 letters

Treatment Adjustments: Futility Criteria - No Borderline Improvement
Borderline improvement defined as:
Decrease in retinal thickness of ≥50 µm and representsat least a 20% reduction
or
Increase in BCVA of ≥5 letters
At the investigator’s discretion: discontinue treatmentafter 3 consecutive injections if no borderline improvement
000
62.8
2427
44
43
2525
1
(32-84)
(47.1)(52.9)
(86.3)
(7.8)(5.9)
(49.0)(49.0)
(2.0)
0
00
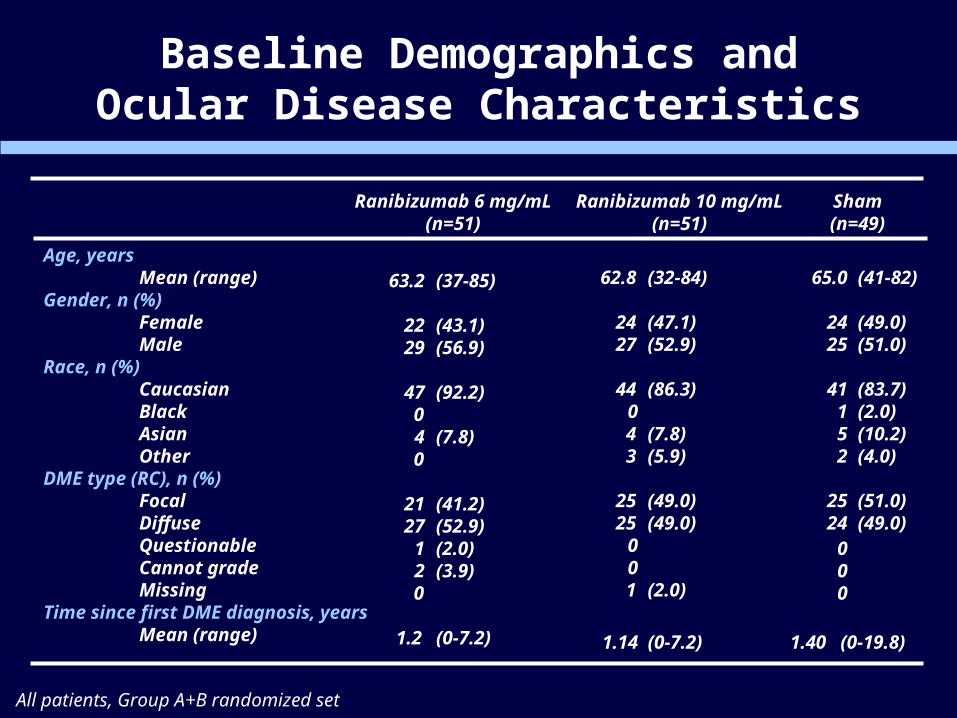
Baseline Demographics andOcular Disease Characteristics
All patients, Group A+B randomized set
Age, yearsMean (range)
Gender, n (%)FemaleMale
Race, n (%)CaucasianBlackAsianOther
DME type (RC), n (%)FocalDiffuseQuestionableCannot gradeMissing
Time since first DME diagnosis, yearsMean (range)
63.2
2229
47
4
2127
12
(37-85)
(43.1)(56.9)
(92.2)
(7.8)
(41.2)(52.9)(2.0)(3.9)
0
0
0
1.2 (0-7.2)
65.0
2425
41152
2524
(41-82)
(49.0)(51.0)
(83.7)(2.0)(10.2)(4.0)
(51.0)(49.0)
Ranibizumab 6 mg/mL(n=51)
Ranibizumab 10 mg/mL(n=51)
Sham(n=49)
1.14 (0-7.2) 1.40 (0-19.8)

RESOLVE Results: Mean BCVA Change* From Baseline
Time (months)
Mean VA change from BL ± SE (letters)
Pooled ranibizumab (N = 102)Sham (N = 49)
0
*All patients, Group A+BFull analysis set; first VA value post-baseline was assessed at Day 8BCVA, best-corrected visual acuity; BL, baseline; *LOCF, last observation carried forward SE, standard error of the mean

RESOLVE: mean CRT change*from baseline
Pooled ranibizumab (N = 102)Sham (N = 49)
Mean CRT change from BL ± SE (µm)
Time (months)
0
*All patients, Group A+BFull analysis set; first VA value post-baseline was assessed at Day 8BL, baseline; *LOCF, last observation carried forward SE, standard error of the mean

Ocular Adverse Events
All patients, Group A+B randomized set
Patients experiencingat least one ocular AE
Most common ocular AEs
Conjunctival hemorrhage
Eye pain
Ranibizumab6 mg/mL
(n=51)
Ranibizumab10 mg/mL
(n=51)
Sham
(n=49)
38 (74.5)
10 (19.6)
9 (17.6)
42 (82.4)
13 (25.5)
9 (17.6)
28 (57.1)
7 (14.3)
10 (20.4)
Adverse event (AE), n (%)

Serious Ocular Adverse Events
Ranibizumab6 mg/ml(n=51)
Ranibizumab10 mg/ml
(n=51)Sham(n=49)
Vitreous hemorrhage 1 0 0
Peripheral retinal ischemia 0 1 0
Retinal artery occlusion* 0 1 0
Endophthalmitis 1 1 0
Retinal detachment 0 0 1
Total patients 1 3 1
* transient post-injection of other non-serious ocular adverse events that occurred, no new or unexpected events were observed for this patient population and treatment

Adverse Events Potentially Related to Systemic VEGF Inhibition
Ranibizumab6 mg/ml(n=51)
Ranibizumab10 mg/ml
(n=51)Sham(n=49)
Arterial thromboembolic events 0 (0.0%) 2 *(4.0%) 2 (4.1%)
Hypertension 4 (7.8%) 5 (9.8%) 5 (10.2%)
Total 4 (7.8%) 7 (13.8%) 6 (12.2%)
* 1 Myocardial infarction, 1 Transient ischemic attack
All patients, Group A+B. Safety set.

RESOLVE: Conclusions
The Phase II RESOLVE study results indicate DME response to treatment with intravitreal ranibizumab
Efficacy in the ranibizumab-treated arms showed clinical and statistical superiority compared with sham treatment in terms of mean average change in BCVA and CRT
The safety profile of ranibizumab in patients with DME was similar to that in patients with AMD
These results provide a sound basis for continuing development of ranibizumab in Phase III trials