1 bringing quality to the bedside the evolution of the nurse quality champion sue nuss, phd, rn...
TRANSCRIPT

1
Bringing Quality to the Bedside
The Evolution of the Nurse Quality Champion
Sue Nuss, PhD, RNNikki Clark, BSN, RNKelli Jacobs, BSN, RN

• Illustrate process to get approval for unit-based nurse Quality Champions
• Describe role of Quality Champion
• Share experiences of 2 Quality Champions
Objectives
Our Goal
Exemplify and enhance a patient-centered, innovative culture of quality and safety throughout the health care journey that is based on evidence and research
Supporting Tactics
To have a standardized nurse driven Q/PI structure throughout the organization• Have a Q/PI team on every nursing unit /department • Have a “Quality Champion” in each nursing unit / department • Quality Champion to work with Manager/ANM to assure quality care is foundation of
culture• Quality and Patient Safety Curriculum
Monthly or Quarterly Nursing Grand Rounds to disseminate Quality initiatives/issues throughout the organization (Align with Practice Pillar to accomplish objective)
Strategic Plan
“Vision” for Quality Champion
Expectations: • 16 or 24 hours per month for these duties
Tenure:• 2 year term with option for 2 consecutive
terms
Qualifications:
• RN (BSN prepared) • 3 years experience (at least 1 year at NMC)
• Prefer some Q/PI experience
Duties:• Work with Manager/ANM to review opportunities for
improvement per unit “quality” scorecard
• “Go to” person for staff re: quality issues
• Disseminate quality information (from unit to NQC and NQC to unit)
• Work with Q/PI team to:– Facilitate no more than 3 team projects per year– Assist with development of action plans– Initiate, monitor, and recommend based on action plan
• Member of unit Q/PI team, but not in chair position
• Given resources to empower QC to make changes related to quality issues
• Complete Foundations in Continuous Improvement training within 6 months of acceptance

16 hours / month
• 0.9 FTE to 1.0 FTE
• 8 hrs/pay period
• Average RN salary = $25.97
• 16 hrs/month = 192 hrs/yr
• Annual cost = $4,986.24
24 hours / month
• Remain 0.9 FTE
• 12 hr shift/pay period
• Average RN salary = $25.97
• 24 hrs/month = 288 hrs/yr
• Annual cost = $7,479.36
Cost of Quality Champion
25,000 4,000 8,583 5,344 11,0000
5,000
10,000
15,000
20,000
25,000
1
Co
st
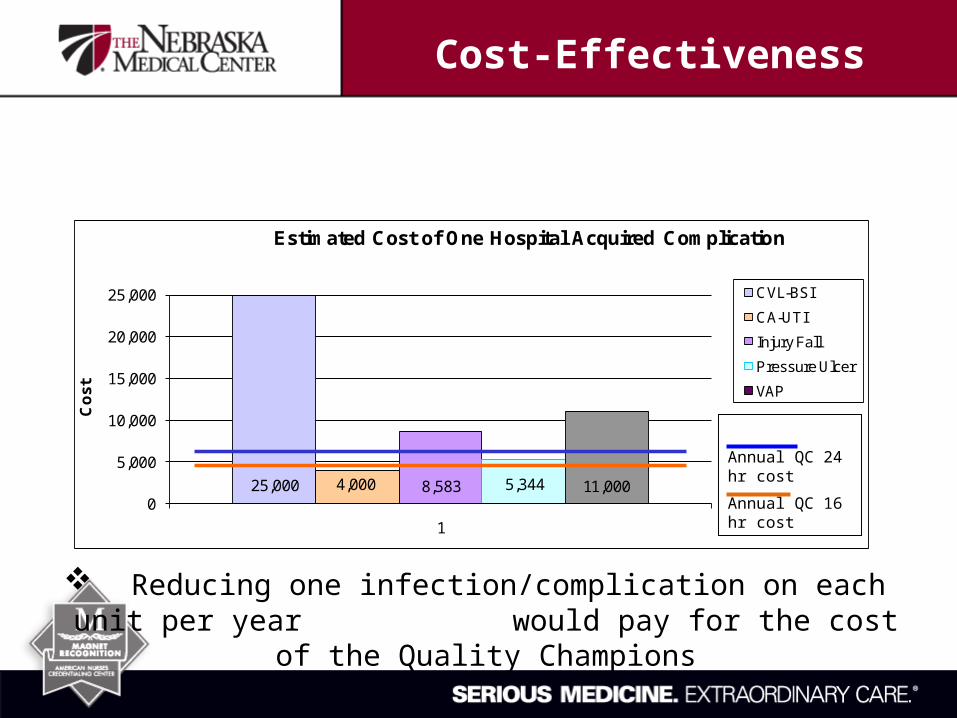
Estimated Cost of One Hospital Acquired Complication
CVL-BSI
CA-UTI
Injury Fall
Pressure Ulcer
VAP
Reducing one infection/complication on each unit per year would pay for the cost of the Quality Champions
Annual QC 24 hr cost
Annual QC 16 hr cost
Cost-Effectiveness
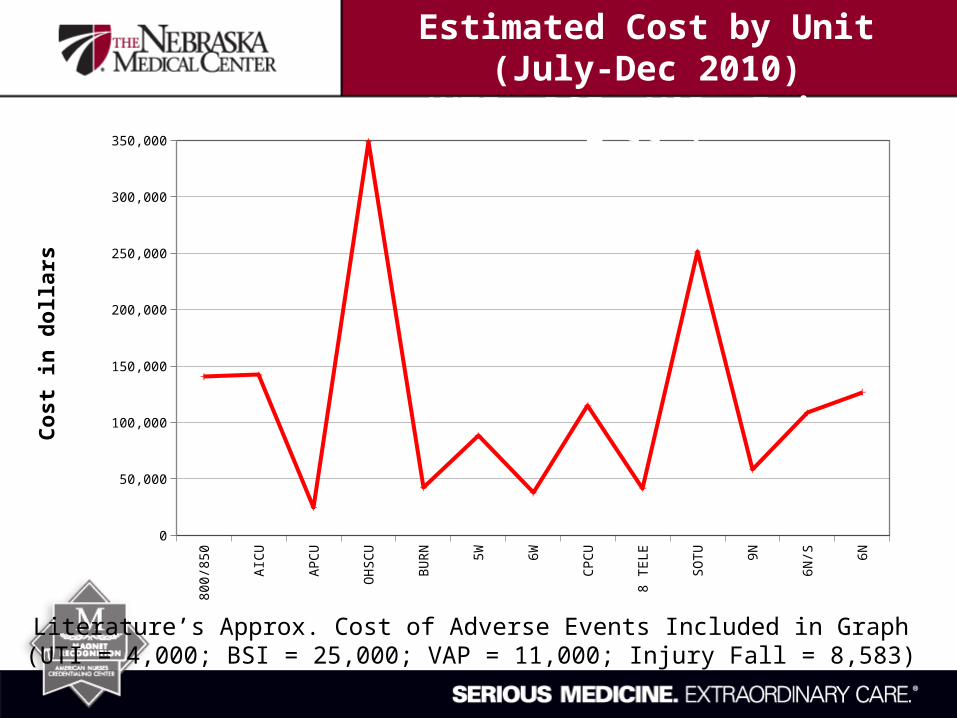
Literature’s Approx. Cost of Adverse Events Included in Graph(UTI = 4,000; BSI = 25,000; VAP = 11,000; Injury Fall = 8,583)
800/850
AICU APCU OHSCU
BURN 5W 6W CPCU 8 TELE
SOTU 9N 6N/S 6N
Total Cost
140583
142166
24583 349162
42166 88332 37749 114830
41749 251247
58166 108583
126830
25,000
75,000
125,000
175,000
225,000
275,000
325,000
Co
st
in d
oll
ars
Estimated Cost by Unit (July-Dec 2010)(UTI, BSI, VAP, Injury Falls)

• Presented proposed QC role to Nursing Directors
• Challenged with “how does QC differ from ANM”?
• Further analysis– Queried ANMs– Analysis using 12 hours per month
Steps Taken

• Only 50% response rate (7 of 14)
• Only 2 stated they had enough time to work on “quality indicators”
• HOWEVER, most of these indicators are day to day indicatorso Quadramed reliabilityo Incident reportso Financial reportso Unclassified patient datao Staffing varianceso Patient roundso Personnel issueso Mentoringo Press Ganey
ANM Responses

• “Time spent on this is hard to quantify”
• “ No data collection is being done; only reviewing reports due to lack of time”
• “Lack of managerial support to work on QI tasks”
• “Some weeks are filled with meetings and makes it hard to focus on this kind of work”
• “Other tasks associated with the ANM-personnel issues and mentoring, patient rounds, meetings, budget, supplies, staff evaluations, availability to staff, etc.
• “ I would say that overall there is enough time to work on those above tasks. There may be days when you cannot spend the necessary time due to other situations of the floor, but overall it is manageable”
ANM Responses

“I strongly feel that the QC person should be a staff nurse that is well respected by the nurses at the bedside. They need to be the voice that is heard, with the management team in the supporting role. Change is better received when it comes from those who are impacted by the change . . . the bedside nurse”
ANM Responses

1. Quality Champion needs to be a staff nurse not an ANM
a. More “approachable” for staffb. “Voice” of staff – not managementc. More staff representation on Nursing Quality Council
2. Compromise from original proposal regarding hours
a. 12 hours per monthi. Meetings – UBC, PI, NQCii. Quality work
b. Cost would be $3740 per yearc. Manager / ANM could assign “opportunity” type projects to QC
Suggestions

3. Suggestions for PI teams:
a. Ideally each unit would have some version of a team dedicated to Quality initiatives
i. Unit based PI teamii. PI work done within UBCiii. For areas with Service / Product Line PI teams, QC would
represent specific unit
Suggestions
1. Decrease in hospital acquired adverse events (HAI, NPSG, PSI)A. Organization levelB. Unit level
2. Improved and sustained Core Measure / SCIP compliance
3. Improved Patient Satisfaction scores
4. Improved staff knowledge of “quality”
5. Professional growth of QCA. Poster presentationsB. PublicationsC. NDNQI Quality Award
Measures of Success

Starting in July 2011 . . .
• 23 QCs identified All inpatient areasSeveral ambulatory / procedural based
areas
• Given 12 hours per month to work on “quality” work
What was the end result?
Expectations of Quality Champions

50%
20%
25%
5%
Time Allotment
Project work (6 hrs)Investigation (2.4 hrs)Meetings (3 hrs)RRT / Codes outside ICU (0.6 hrs)
What will QC time look like?

• Investigation (20%)
– Scoping of project– Defining problem
• Project work (50%)
– Preparing– Doing– Leading “the work”
• Meetings (25%)
– UBC / Unit PI– NQC– UBMD / Mgr / QC
• RRT/Codes outside ICU (5%)
– Look at unit trends– Discuss with staff– Develop action plans
Time Allotment
Medical Director
Quality Champion
Manager / ANM
Goal of triad is to drive unit specific quality initiatives – from a
medical, administrative, and direct care provider
perspective
Unit Quality Triad

• Use time efficiently do investigating or project work on a day when already coming in for a meeting
• Work with unit-based Quality Triad to improve outcomes
• Reach out to other QC work on similar projects collectively
• Come prepared to discuss QC work at NQC
• Track time dedicated to “quality” work
Expectations

• Routine documentation audits
• Program certification or regulatory work
• Work that does not align with HQC goals or unit goals
What the QCs is not expected to do?

• Infection Related– CA-UTI (early foley removal)– CL-BSIs
• Care of the central line (creating a standardized process)
– Decrease UTI rate in thoracic patients
• Patient Satisfaction– Pain control and monitoring– Patient Satisfaction
• Nurse Communication
– HCAHPS • RN Communication Domain
– Press Ganey Patient Satisfaction– Response time to call lights
• Patient Safety– Falls – Medication errors related to change in
concentration and mislabeled bags that protect light sensitive medications
– Common E's and Trends on Incident Reports
• Miscellaneous– Saline flush confirmation and
documentation – Unit Throughput – Discharge planning– Patient education and conversion to
outpatient learning – Accurate documentation for immediate
use sterilization
What are QCs working on?
• Testimonials from 2 QCs
– Kelli Jacobs, BSN, RN
– Nikki Clark, BSN, RN
Real life experiences

24
• My background– RN for 5 years– Work on Solid Organ Transplant Unit
• Why I wanted to be a QC– Opportunity to learn more about QI process and work directly with QI projects
• Current project is NS Flush Documentation
– SOTU nurses to barcode scan all NS flushes that they administer to their patients • To provide accurate documentation of the quantity used • Barcode scanning also supports our institution's expectation of real-time charting
• Why this project? – The majority of saline flushes used by the nurses were not being documented or recorded in the pt's
I&O– Opportunity existed to improve
• Reimbursement for flushes• Quality of patient care by providing a reliable way for nurses to document all of the flush syringes that are used
QC Perspective – Kelli Jacobs, BSN, RN
25
• Success of the QC role– Provides a great opportunity to work hands-on with unit-based and hospital-wide quality projects– Gives staff nurses the power and ability to directly affect quality of patient care and nursing processes
• Success of Quality Triad Model– Helps build relationships between the staff nurses, manager, and the unit-based medical director – By working together, valuable input and ideas are acquired that would probably otherwise be overlooked – It improves communication and builds trust between team members and allows the team as a group to look at a
quality issue from different perspectives – This aids in being able to address quality improvement issues more thoroughly and completely
• Opportunities– Still have an opportunity to strengthen our triad meetings by creating a standing agenda and trying to schedule a
set date and time for meetings – Medical director tries to attend not just the triad meeting, but all of our quality meetings if he is able – Overall, this has created opportunities, not just for the triad members (QC, manager, UMD), but also for other staff
nurses, as anyone is welcome to join the unit Quality team and partake in quality improvement projects
• Next Project– Hand Hygiene compliance
QC Perspective – Kelli Jacobs, BSN, RN

26
• My background– Healthcare for 13 years – Cancer research for 3 1/2 years – RN for 3 years– Work on Oncology-Hematology Special Care Unit
• Why I wanted to be a QC– My background in research – Wanted to make a difference by influencing and demonstrating best practice to our patients and staff– Wanted new staff to have the opportunity to ask questions and bring concerns to someone that worked on the floor – Helps me brush up on skills, policies, and procedures – Helps to demonstrate to others so that they too are following policies and procedures
• Current project is NS Flush Documentation – Reducing central line blood stream infections through looking at all aspects that the RN takes part in:
• 5 second scrub the hub/line accessing • Dressing changes• Port needle changes• Bathing
• Why this project? – According to our HCAHP scores, this was an area that we needed to work on – It is important means to infection especially in immunocompromised patients.
QC Perspective – Nikki Clark, BSN, RN

27
• Success of the QC role– Serves a liaison person for staff to express concerns about practices on the floor– QC can help drive the focus to look into the issue and take action if necessary – QC can take concerns to management for support and updates– It is also something that I enjoy doing
• Success of Quality Triad Model– The triad model is great if you have parties on board – When the MD is involved, they tend to have more clout when pulling strings to get things accomplished in certain situations– Having active management involvement created rapport and demonstrates that they do care about what is happening on the floor – QC serves as a liaison between management/MDs to staff on the floor
• Opportunities– There are always opportunities.– I wish I could have more involvement from my medical director– Opportunities to initiate change in a nonthreatening way so that staff is more receptive to changes in practice in order to
complete best practice according to evidence based practice– Have found that staff sometimes think they are doing something correctly, only to find out that according to policy they are
missing a few steps
• Next Project– TBD– Always looking at falls– Brushing up with RNs on required education that needs to be given to pt before/after chemo and/or transplant.
QC Perspective – Nikki Clark, BSN, RN
