030.furcation involvement and its therapy
TRANSCRIPT
By By
Dr. Syed Jaffar RazaDr. Syed Jaffar RazaPG Trainee (Perio)PG Trainee (Perio)
FGSH, IslamabadFGSH, Islamabad
1
FURCATION InvolvementFURCATION Involvement & its THERAPY & its THERAPY

Definition
“Furcation defect : Term used to describe bone loss, usually a result of periodontal disease, affecting the base of the root trunk of a tooth where two or more roots meet.”
OR
“Invasion of bifurcation and trifurcation
of multi-rooted teeth by periodontal
Disease”
2
Terminology
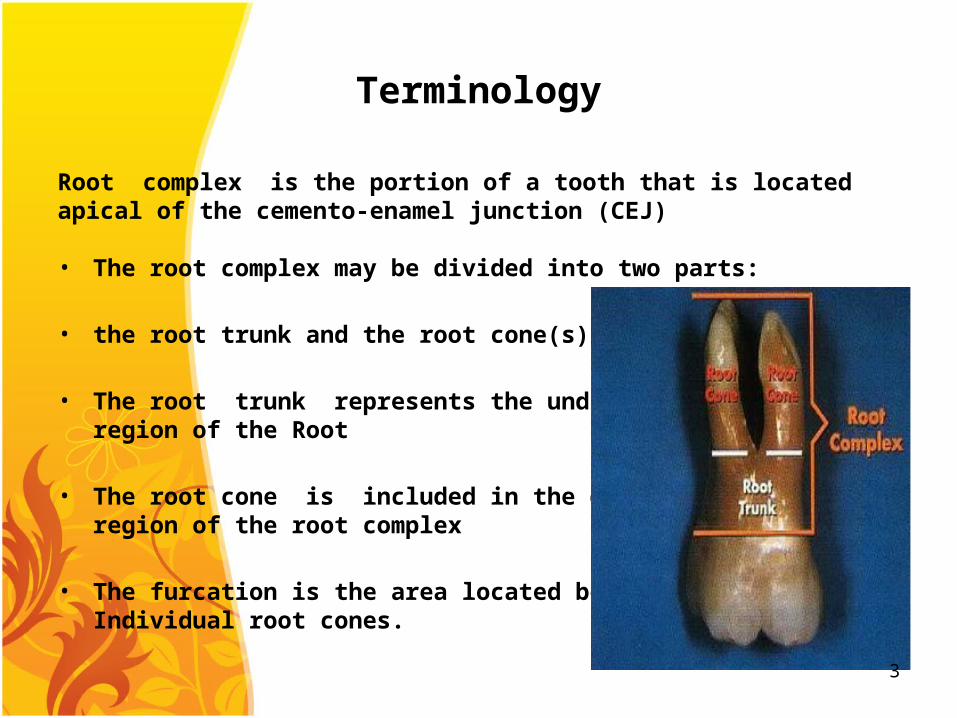
Root complex is the portion of a tooth that is locatedapical of the cemento-enamel junction (CEJ)
• The root complex may be divided into two parts:
• the root trunk and the root cone(s)
• The root trunk represents the undividedregion of the Root
• The root cone is included in the dividedregion of the root complex
• The furcation is the area located betweenIndividual root cones.
3

• Furcation entrance: the transitional area between the undivided and the divided part of the root
• Furcation fornix: the roof of the furcation
• Degree of separation: the angle ofseparation Between two roots (cones)
• Divergence: distance between two roots
4
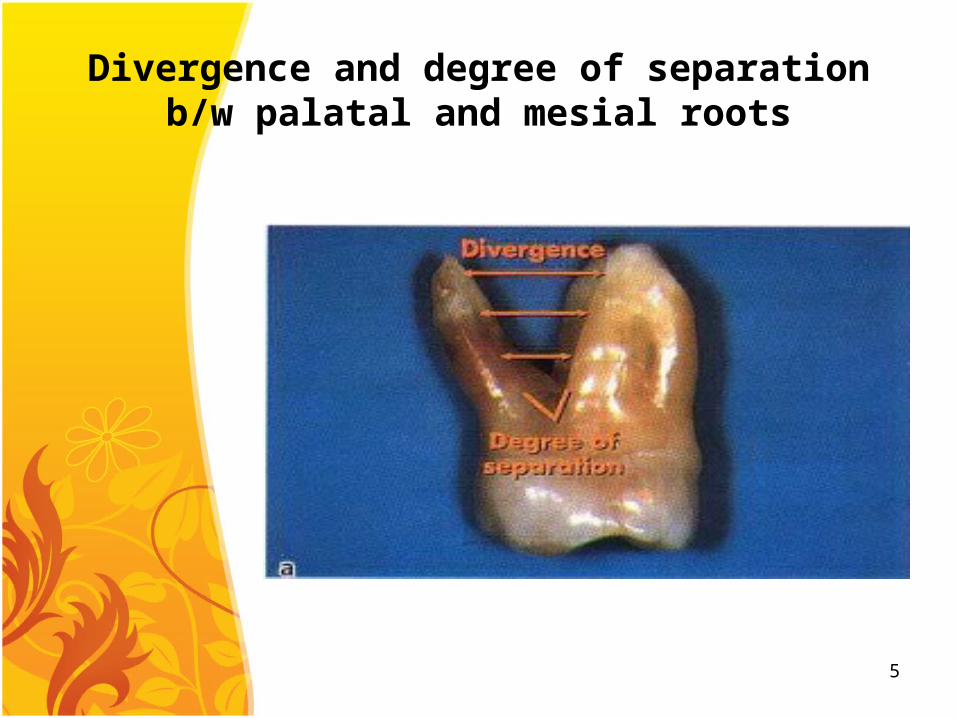
Divergence and degree of separation b/w palatal and mesial roots
5

Apical-occlusal view of a maxillary molar where the three root cones make up the furcated region and
the three furcation entrances
6

Buccal view of furcation entrance and its roof
7
Etiology
• bacterial plaque and the inflammatory consequences that result from its long-term presence
• local factors : affects plaque deposition
• Age : increases with age
• Dental caries
• Pulpal death
• Bacterial invasion
• Trauma from occlusion
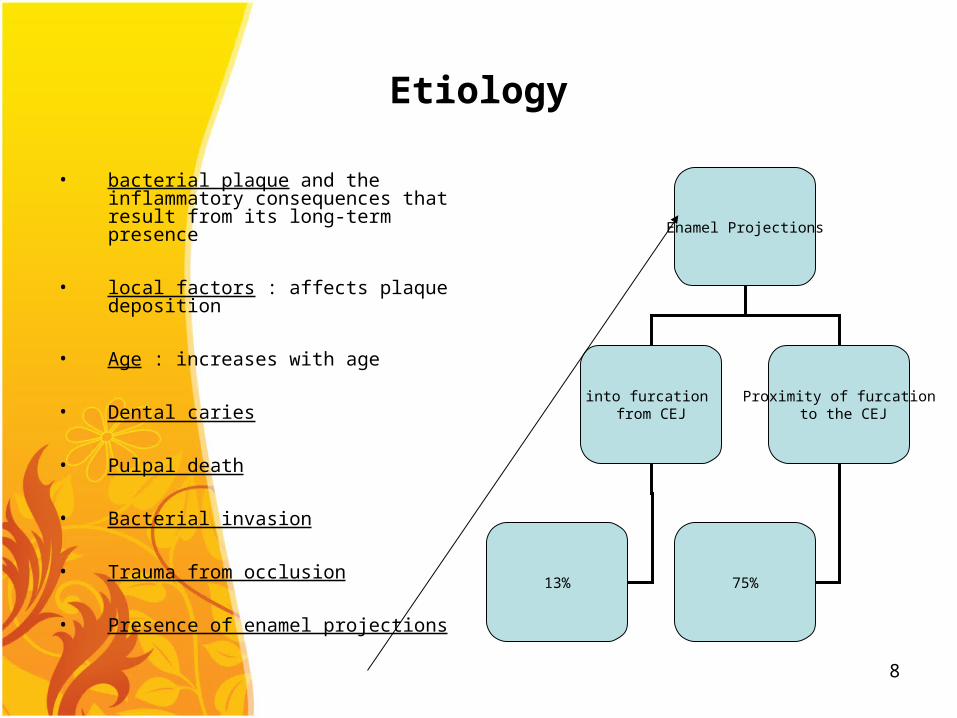
• Presence of enamel projections
Enamel Projections
into furcation from CEJ
Proximity of furcation to the CEJ
13% 75%
8

Classification
Horizantal Component involvement
Vertical component involvement
9

Hamp et al. (1975) classification
• Degree I: Horizontal loss of periodontal support notexceeding 1/3 of the width of the tooth
• Degree II: Horizontal loss of periodontal supportexceeding 1/3 of the width of the tooth, but notencompassing the total width of the furcation area
• Degree III: Horizontal "through and through" de-struction of the periodontal tissues in the furcationarea
10
Glickman`s Classification
Grade I:
early stage of furcation involvement supra bony pocket increase probing depth due to early bone
loss radiographic changes not found
Grade II:
cul-de-sac with definitely horizantal component
portion of bone remain in the furcation region vertical bone loss may or may not be
present.11
Glickman`s Classification
Grade III:
bone is not attached to dome of furcation Complete loss of interadicular bone appearance of radiolucent area with pocket
formation
Grade IV:
loss of attachment and gingival recession furcation is clinically visible Probe passes easily through and through.
12
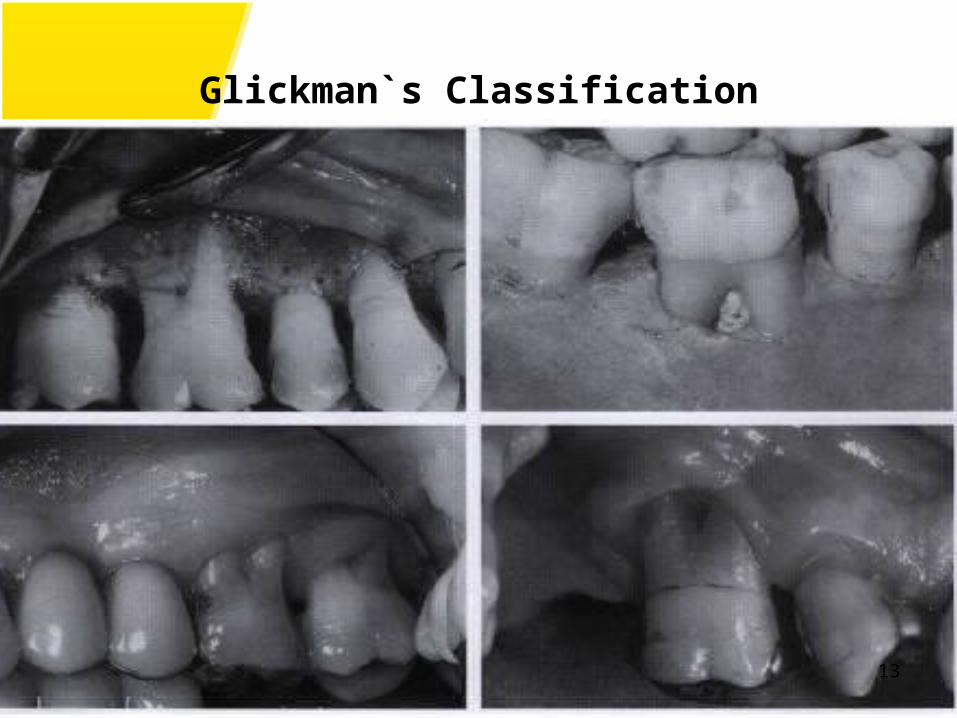
Glickman`s Classification
13

Diagnosis
• The following parameters should be recorded to evaluate the amount of tissue loss in periodontal disease and also to identify the apical extension of the inflammatory lesion
pocket depth (probing depth)
attachment level (probing attachment level)
furcation involvement (measured with nabers probe)
Radiographs
Radiographs
periapical
bitewing
14

Pocket Depth
15

Nabers probe for furcation areas
16

Technique of Nabers Probe
17
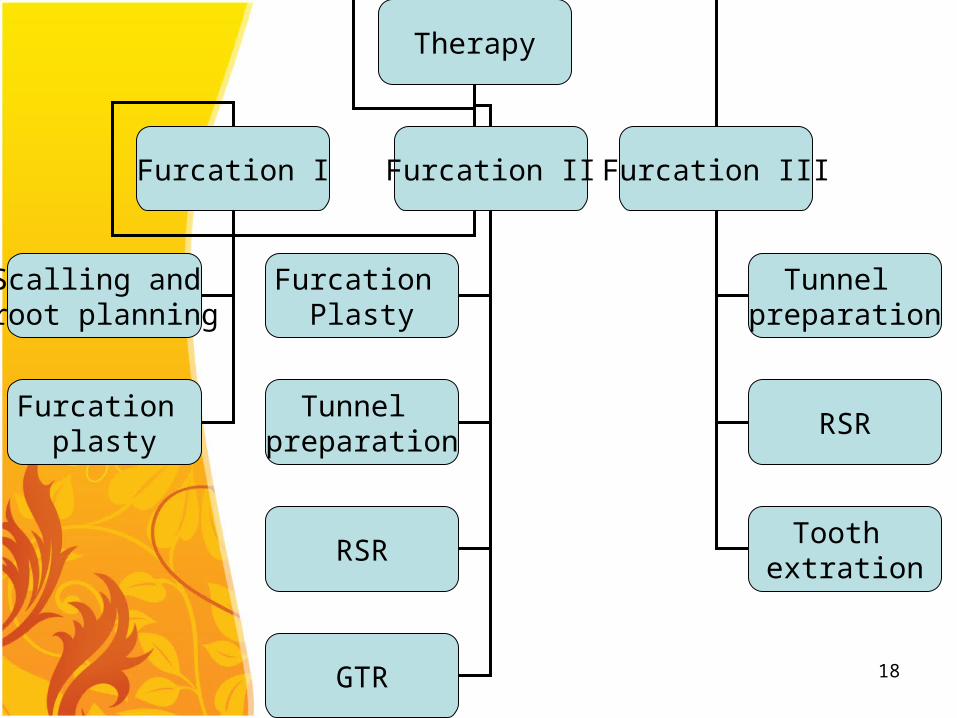
Therapy
Furcation I Furcation II Furcation III
Scalling and root planning
Furcation plasty
Furcation Plasty
Tunnel preparation
RSR
GTR
Tunnel preparation
RSR
Tooth extration
18

Therapy Objectives
Removal of theBacterial Plaque
Restoration ofHealthy anatomyOf periodontium
19
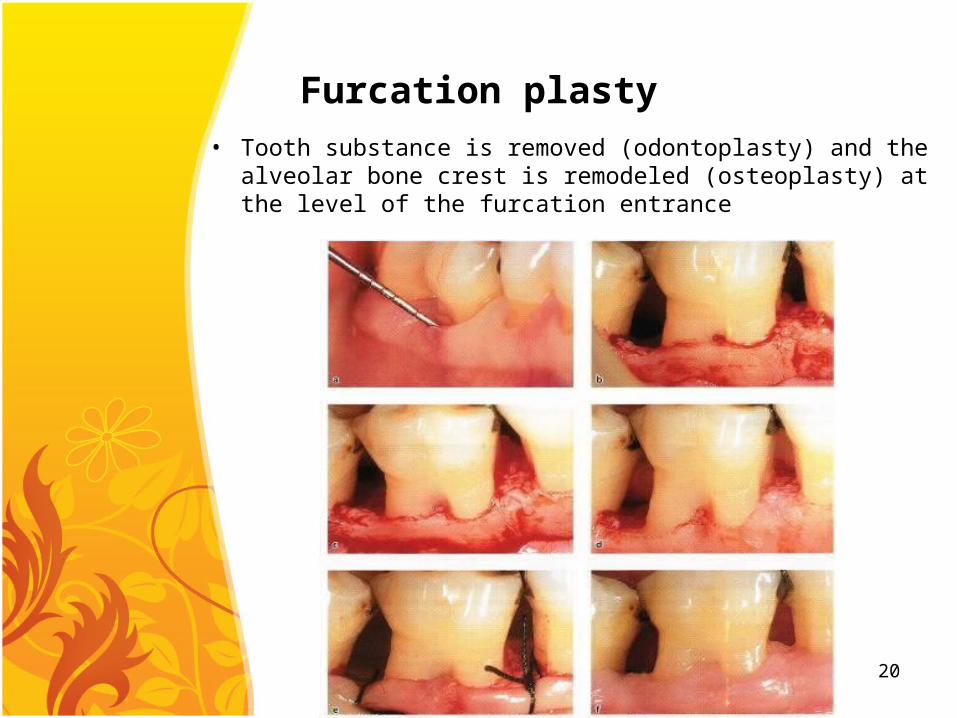
Furcation plasty
• Tooth substance is removed (odontoplasty) and the alveolar bone crest is remodeled (osteoplasty) at the level of the furcation entrance
20

Furcation plasty procedure
Reflection of soft tissue flap.
Removal of the inflammatory soft tissue
scaling and root planning of the exposed root surfaces.
The removal of crown and root substance in thefurcation area (odontoplasty)
The recontouring of the alveolar bone crest (osteoplasty)
positioning and the suturing of the mucosalflaps at the level of the alveolar crest in order tocover the furcation entrance with soft tissue.
21
Tunnel preparation
Technique used to treat deep degree II and degree III furcation defects in mandibular molars
Following hard and soft tissue resection enough space has been established in the furcation region to allow access for cleaning devices to be used during self performed plaque control
The flaps are apically positioned
The exposed root surfaces should be treated by topical application of chlorhexidine digluconate and fluoride varnish. Because of pronounced risk for root sensitivity and for carious lesions developing on the denuded root surfaces within artificially prepared tunnels
22

Tunnel preparation
23

Root separation and resection (RSR)
Root separation involves the sectioning of the root complex and the maintenance of all roots.
Root resection involves the sectioning and the removal of one or two roots of a multirooted tooth.
RSR is frequently used in cases of deep degree IIand degree III furcation involved molars.
24
Criteria for RSR
• The length of the root trunkA tooth with a short root trunk is a good candidate for RSR;
• The divergence between the root conesRoots with a short divergence are technically more difficult to separate than roots which are wide apart
• The length and the shape of the root conesShort and small root cones following separation tend to exhibit an increased mobility
• Amount of remaining support around individual rootsThis should be determined by probing the entire circumference of the separated roots
• Stability of individual roots
• Access for oral hygiene devices25

Regeneration of furcation defects
• "guided tissue regeneration" (GTR) therapy is provided
• GTR is more successful in degree II furcation involvements then in degree III involvements
26

GTR limits
• The morphology of the periodontal defect Horizantal bone loss
• The anatomy of the Furcation with complex morphology more in maxillary than mandibular tooth
• The varying and changing location of the soft tissue margins during the early phase of healing with a possible recession of the flap margin and early exposure of both the membrane material and the fornix of the Furcation
27

GTR feasibility improves if
• Adequate debridement area of exposed root surface
• The membrane material is properly placed
• A plaque control program is put in place.
This should include daily rinsing with a chlorhexidine solution and professional toothcleaning once a week for the first month, and once every 2-3 weeks for at least another 6 months of healing following the surgical procedure
28
Extraction option
• Through and through Furcation defects (degree III and IV)
• Advance attachment loss
• Un-adequate plaque control
• High caries activity
• Non compliance of the patient
29

The ENDThe END
30