00754569
DESCRIPTION
1TRANSCRIPT

Proceedings - 19th International Conference - IEEE/EMBS Oct. 30 - Nov. 2, 1997 Chicago, IL. USA
CLASSIFICATION OF DIABETIC RETINOPATHY LESIONS FROM STEREOSCOPIC FUNDUS IMAGES
Hung Nguyen, Ani1 Roychoudhry, Anthony Shannon University of Technology, Sydney, PO Box 123, Broadway NSW 2007, Australia
Abstract Classification of the severity of diabetic retinopathy (DR) is vital .for determining appropriate therapies for this frequent complication of diabetes. The purpose of this study is develop an automated system to help with the classifcation of some diabetic retinopathy lesions stereoscopic fundus images. The system is used in particular to distinguish drusen from hard exudates (diabetic retinopathy lesions), and to evaluate the severity of lesions such as retinal oedema.
Introduction Diabetic retinopathy (DR) is the leading cause of visual loss in the westem world. Commonly, about 20% of patients with non-insulin dependent diabetes mellitus (NIDDM) have already developed evidence of retinopathy at clinical diagnosis. If it is detected in the early stages, an appropriate treatment can be devised to prevent the progression of diabetic retinopathy or blindness.
In a typical diabetic retinopathy grading scheme used by the ETDRS research group, non-simultaneous stereo photographs of seven standard fields of the retina are graded by trained non-ophthalmologists who are selected for normal depth perception [l].
The lesions of diabetic retinopathy are basically divided into “Background” and “Proliferative” lesions. Typical background lesions are microaneurysms, retinal haemorrhages (dot, blot and flame), hard exudates, cotton wool spots, intraretinal microvascular anomalies, retinal oedema etc. Proliferative lesions include new vessels, pre- retinal haemorrhage, fibrous tissue and retinal detachment.
Drusen are confounding lesions which are not associated with diabetic retinopathy. They appear as deep, yellowish/white dots, sometimes surrounded by a thin line of pigment. Large drusen can easily be recognised but small drusen can be confised with small hard exudates. A good stereoscopic effect is important for the classification of diabetic retinopathy as drusen are located very deep at the level of the retinal pigment epithelium, while hard exudates usually appear to be more superficial.
Drusen also have many other distinguishing characteristics like round shape, dull appearance and a faint border of pigment that have been exploited by research with impressive
results (The STARE project [2]). However an important component of stereoscope photographs, depth, has so far been neglected. Another type of DR lesions, retinal thickening (oedema), is usually graded by the size of the thickened area and the maximum thickness within that area.
The purpose of this study is to develop an automated classification system which uses depth as another parameter to further improve the classification accuracy for confounding lesions and to evaluate the severity of DR lesions such as retinal thickening and retinal detachment.
Methods A typical stereo photography camera geometry [3] is shown in Figure 1, where W is a world point that is imaged by a left and right camera. It can be shown- that depth is related to disparity by
AB Z=/z - - x2 - XI
where h is the focal length, B is the baseline, and Z is the true world coordinate for depth.
Image I /I
axis
Fig 1. Stereo Camera Geometry
The computation problem of obtaining depth from stereo images is a two part process: 0 features in the left and right images are matched to one
other (the correspondence process) 0 the disparity in location of corresponding features is
determined. From this disparity the location of the feature in three dimensional space is determined.
For corresponding points, the images have to be adjusted to satisfy the epipolar conditions [4]. This implies that a point on the right image lies on the same horizontal line with the
(0-7803-4262-3/97/$10.00 (C) 1997 IEEE) 426
Proceedings - 19th International Conference - IEEE/EMBS Oct. 30 - Nov. 2, 1997 Chicago, IL. USA
corresponding point on the left image. In order to achieve the correspondence process, one of the images of the stereo pair may have to be rotated. scaled and translated. A global registration technique based on Fourier Mellin Transform is used to determine the rotational and scaling factors [5]. The result of this process is that the required scale change and rotation are reduced to translations. Once the images have been rotated and scaled, a correlation scheme is used to determine the vertical translation required to satisfy the epipolar condition.
The green plane of the images is used as it exhibits highest contrast. The left and right images undergo a radiometric correction [6] which matches the radiometry of the images by making use of the mean, variance and dynamic range of intensities for each image. The correspondence search is implemented as a window based correlation search [3]
where
and Y is the cross-correlation coefficient at point (s,t) over the neighbourhood defined by w(x,y). For an N x N stereoscopic pair of images, x,y ,s ,r = 0 , 1 , 2 , . . . , N - l , and
f,,w,,, are the mean values in the regions of the two images.
A 15 x 15 window is used as it gives good results in terms of least false matches. Both natural images as well as the segmented images are used. The natural images yield a dense depth map but matching is prone to errors in some regions. The segmented images yield a sparse but accurate depth map. Finally, the disparity map obtained from this process is smoothed using a 5 point low pass box filter. Essentially, the images are segmented [2] for bright lesions and the segmented optic disc [7] disparity is used as a reference.
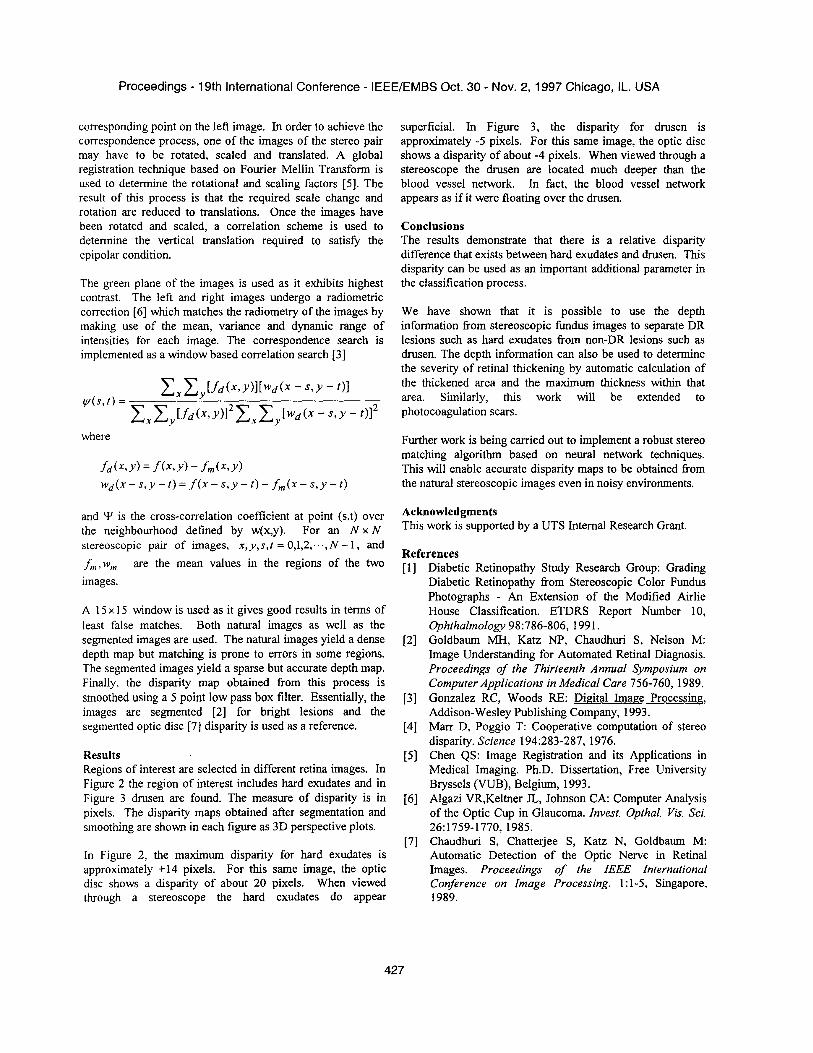
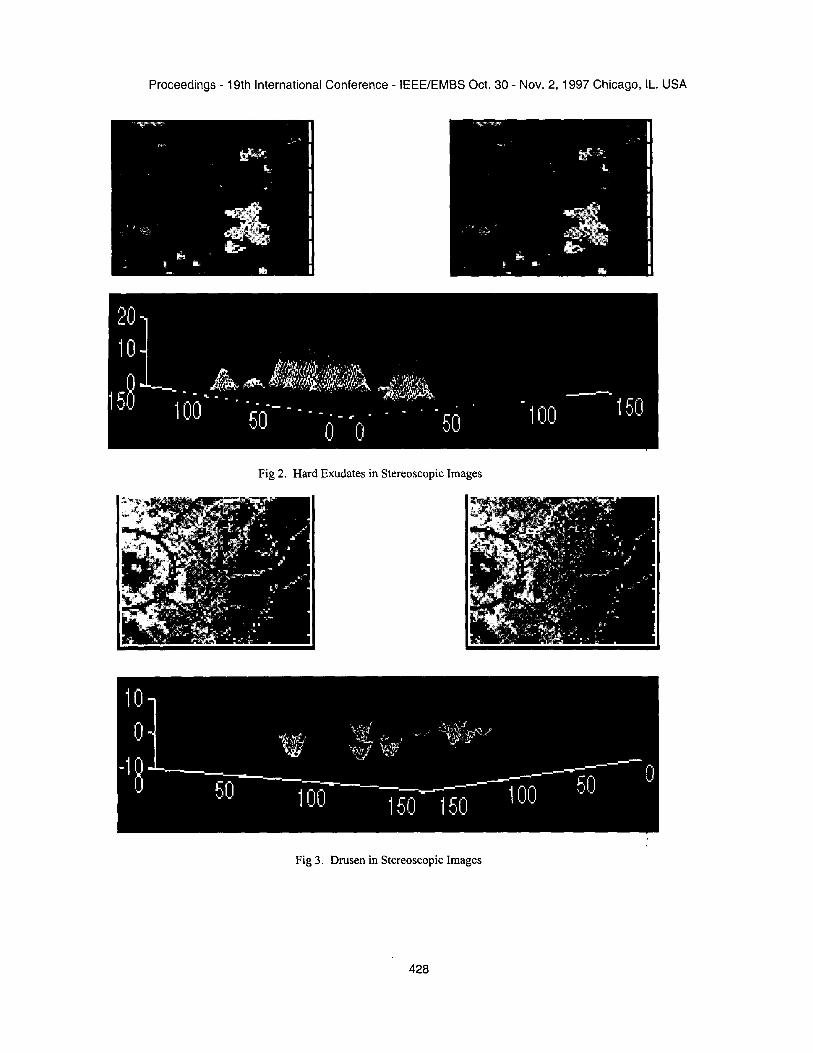
Results Regions of interest are selected in different retina images. In Figure 2 the region of interest includes hard exudates and in Figure 3 drusen are found. The measure of disparity is in pixels. The disparity maps obtained after segmentation and smoothing are shown in each figure as 3D perspective plots.
In Figure 2, the maximum disparity for hard exudates is approximately +14 pixels. For this same image, the optic disc shows a disparity of about 20 pixels. When viewed through a stereoscope the hard exudates do appear
superficial. In Figure 3, the disparity for drusen is approximately -5 pixels. For this same image, the optic disc shows a disparity of about -4 pixels. When viewed through a stereoscope the drusen are located much deeper than the blood vessel network. In fact, the blood vessel network appears as if it were floating over the drusen.
Conclusions The results demonstrate that there is a relative disparity difference that exists between hard exudates and drusen. This disparity can be used as an important additional parameter in the classification process.
We have shown that it is possible to use the depth information from stereoscopic fundus images to separate DR lesions such as hard exudates from non-DR lesions such as drusen. The depth information can also be used to determine the severity of retinal thickening by automatic calculation of the thickened area and the maximum thickness within that area. Similarly, this work will be extended to photocoagulation scars.
Further work is being carried out to implement a robust stereo matching algorithm based on neural network techniques. This will enable accurate disparity maps to be obtained fi-om the natural stereoscopic images even in noisy environments.
Acknowledgments This work is supported by a UTS Internal Research Grant.
References Diabetic Retinopathy Study Research Group: Grading Diabetic Retinopathy from Stereoscopic Color Fundus Photographs - An Extension of the Modified Airlie House Classification. ETDRS Report Number 10, Ophthalmology 98:786-806, 1991. Goldbaum MH, Katz NP, Chaudhuri S, Nelson M: Image Understanding for Automated Retinal Diagnosis. Proceedings of the Thirteenth Annual Symposium on Computer Applications in Medical Care 756-760, 1989. Gonzalez RC, Woods RE: Digital Image Processing, Addison-Wesley Publishing Company, 1993. M m D, Poggio T: Cooperative computation of stereo disparity. Science 194:283-287, 1976. Chen QS: Image Registration and its Applications in Medical Imaging. Ph.D. Dissertation, Free University Bryssels (VUB), Belgium, 1993. Algazi VR,Keltner JL, Johnson CA: Computer Analysis of the Optic Cup in Glaucoma. Invest. Opthal. Vis. Sci.
Chaudhuri S, Chatterjee S, Katz N, Goldbaum M: Automatic Detection of the Optic Nerve in Retinal Images. Proceedings of the IEEE International Conference on Image Processing. 1 : 1-5, Singapore, 1989.
26:1759-1770, 1985.
427
Proceedings - 19th International Conference - IEEE/EMBS Oct. 30 - Nov. 2, 1997 Chicago, IL. USA
~
Fig 2. Hard Exudates in Stereoscopic Images
Fig 3 . Drusen in Stereoscopic Images
428