“ understanding chronic kidney disease in general practice” dr emma dunn consultant nephrologist...
TRANSCRIPT

“ Understanding Chronic Kidney Disease in General
Practice”
Dr Emma DunnConsultant Nephrologist
Leeds Teaching Hospitals NHS Trust

• Background to CKD initiative – NSF and NICE
• eGFR
• Management of CKD in primary care
• Who to refer
• Renal anaemia/ bone disease

CKD initiative

Renal registry data 2007
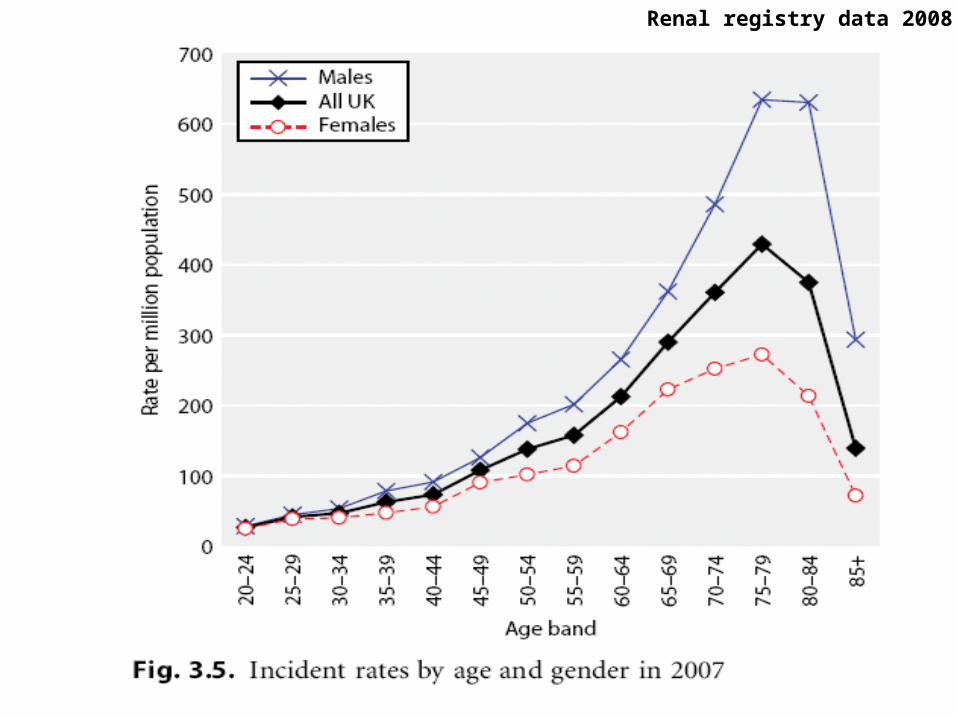
Renal registry data 2008

‘Crash Landers’

The National Service Framework for renal services
‘ to raise profile of renal disease as a chronic disease’
‘ to raise quality of care provided for people with kidney disease’
‘to increase their choice’
‘to minimise the impact of their disease on their lives’

Set 5 standards for care and identified 30 markers of good practice to be delivered by 2014:
‘ to help NHS and its partners to manage demand’
‘to increase fairness of access and improve choice and quality in dialysis and kidney transplant services’


Set 4 quality requirements and identified 23 markers of good practice that aimed to support NHS organisations in:
‘ prevention of chronic kidney disease in people at risk’
‘slowing down progression of the disease’
‘minimising consequences of acute renal failure’
‘extending palliative care to patients on dialysis, or with ESRD who are near the end of their lives’
National Service Framework for Renal Services (part 2) –
February 2005
1. People at risk of developing or having undiagnosed CKD, especially people with diabetes or hypertension, must be identified, assessed and their condition managed to preserve their kidney function.
2. People with a diagnosis of CKD must receive timely, appropriate and effective investigation, treatment and follow up to reduce the risk of progression and complications

Patients to be screened for CKD
• Diabetes
• Hypertension
• Cardiovascular disease (IHD, CHF, PVD, cerebrovascular disease)
• Structural renal tract disease, renal calculi or prostatic hypertrophy
• Multisystem diseases with potential renal involvement (e.g. SLE)
• Family Hx of stage 5 CKD or hereditary kidney disease
• Opportunistic detection of haematuria or proteinuria

All laboratories must measure kidney function using a formula-based estimation of glomerular filtration rate (eGFR).
CKD should be described using classification developed for the Kidney Disease Outcomes Quality Initiative (K/DOQI)
which divides CKD into five stages depending on eGFR.
To achieve quality requirements 1 and 2:
1. Prevention and early detection of CKD
2. Minimising consequences and progression of CKD
Renal NSF part 2 - CKD

Classification of Renal Impairment (K/DOQI)
• Stage 1 - Kidney damage with eGFR ≥90• Stage 2 - Kidney damage with eGFR 60-89• Stage 3 - Kidney damage with eGFR 30-59• Stage 4 - Kidney damage with eGFR 15-29• Stage 5 - Kidney failure eGFR<15 or on
dialysis
Classification of Renal Impairment (NICE)
• Stage 1 - Kidney damage with GFR≥90• Stage 2 - Kidney damage with GFR 60-89• Stage 3a - Kidney damage with GFR 45-59• Stage 3b - Kidney damage with GFR 30-44• Stage 4 - Kidney damage with GFR 15-29• Stage 5 - Kidney failure, eGFR <15 or on
dialysis
• ‘p’ for proteinuria (ACR ≥30mg/mmol or PCR ≥50mg/mmol)


Why do we need a CKD initiative?

Because………1. CKD is bad for you

Outcomes of CKD
• Loss of Kidney Function (kidney failure)
• Complications associated with CKD- hypertension- anaemia- bone disease- malnutrition - neuropathy- decreased quality of life
• Increased Morbidity and Mortality - Cardiovascular disease

ESRD

Survival of patients on dialysis in the UK 10 years after commencing renal replacement
(Renal Registry Report 2008)

Impact of ESRD on patient’s life expectancy
Levey et al AJKD 1998;32:853

Renal Registry Report 2008

Renal Registry Report 2008

Relative risk of death in all prevalent RRT compared with UK general population in 2007
Renal Registry Report 2008

Cardiovascular disease and CKD
• Life expectancy of patients with ESRD is poor
49 yr old male Life expectancy (years)
General population 29.8Prostate cancer 12.8Colon cancer 8.6ESRD 7.1
• Majority of premature death due to CVD (CVA, IHD, Heart Failure)

Causes of death in UK dialysis patients
Renal Registry 2008

CKD patients (pre-ESRD)

40
35
30
25
20
15
10
5
0
2.11 3.65
11.29
36.60
≥60(1&2) 45–59 (3A) 30–44 (3B) 15–29 (4) <15 (5)
Estimated GFR (ml/min/1.73 m2)
No. of events 73,108 34,690 18,580 8809 3824
21.80
Age-standardised rate of cardiovascular events(per 100 person-y)
CKD and cardiovascular risk
NEJM 2004; 351: 1296

Age-standardised rate of deathfrom any cause (per 100 person-y)16
14
12
10
8
6
4
2
0
0.76 1.08
4.79
11.36
14.14
≥60(1&2) 45–59(3A) 30–44 (3B) 15–29 (4) <15 (5)
Estimated GFR (ml/min/1.73 m2)
No. of events 25,803 11,569 7802 4408 1842
CKD and cardiovascular risk
NEJM 2004; 351: 1296

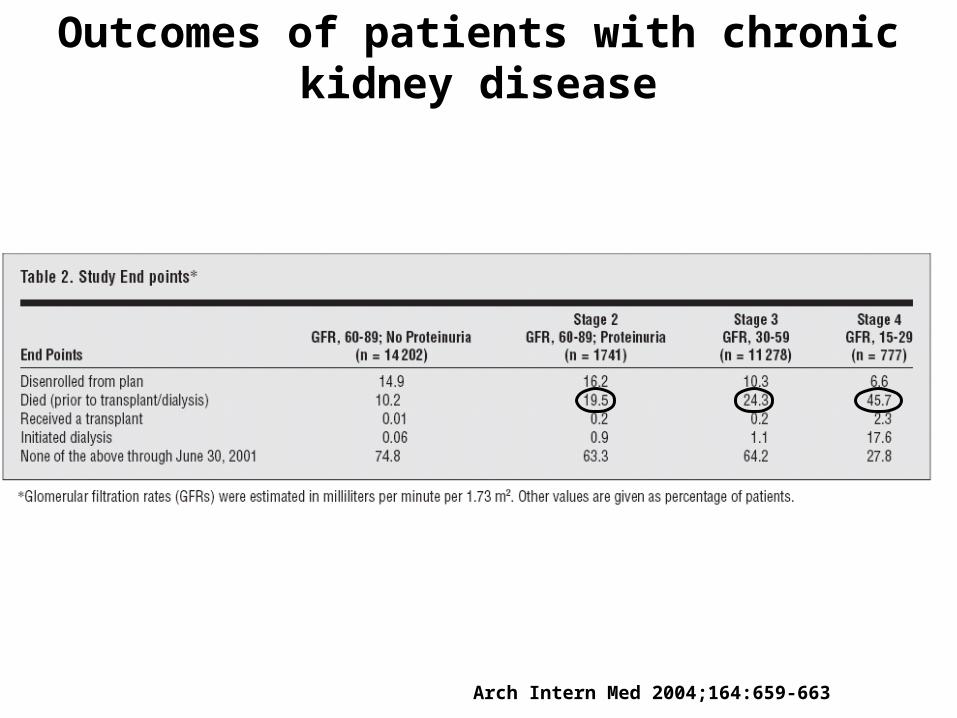
Outcomes of patients with chronic kidney disease
Arch Intern Med 2004;164:659-663
}1.1% }1.3% }19.9%
Kaiser Permanente health plan, Oregon USA
~28000 patients identified as having CKD (recorded eGFR <90ml/min on 2 separate occasions at least 90 days apart)
5 year follow-up (1996-2001) - from time of initial eGFR estimation until required RRT, died, or disenrolled from health plan
Outcomes of patients with chronic kidney disease
Arch Intern Med 2004;164:659-663

New Opportunities for Early Intervention by Computerised Assessment
(NEORICA)
Kidney International 2007;72:92-99

Because………1. CKD is bad for you2. CKD is common

UK Prevalence of CKD
NEOERICA project – primary care Manchester, Kent and Surrey
N=162,113
Age standardised prevalence of stage 3-5 CKD 8.5%
KI 2007,72:92-99
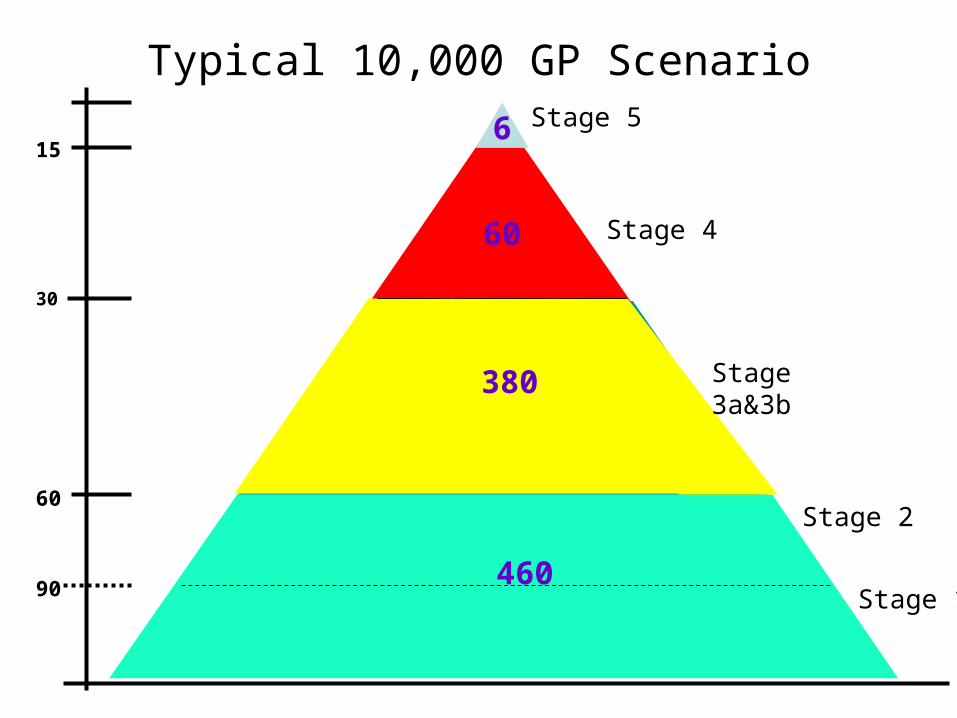
CKD: A Typical GP Practice of 10000
Stage 1
Stage 5
Stage 4
Stage 3a&3b
Stage 2
460
60
6
380
90
60
15
30
eGFR Typical 10,000 GP Scenario

Because………1. CKD is bad for you2. CKD is common3. Often asymptomatic in early stages,
but evidence shows that early intervention reduces risk of progression of early CKD to ESRF and reduces CV risk

Diagnosing kidney disease

Easy Assessment
• Serum Creatinine
Screening for renal disease
Easy Assessment
• Serum Creatinine
but has LIMITATIONS
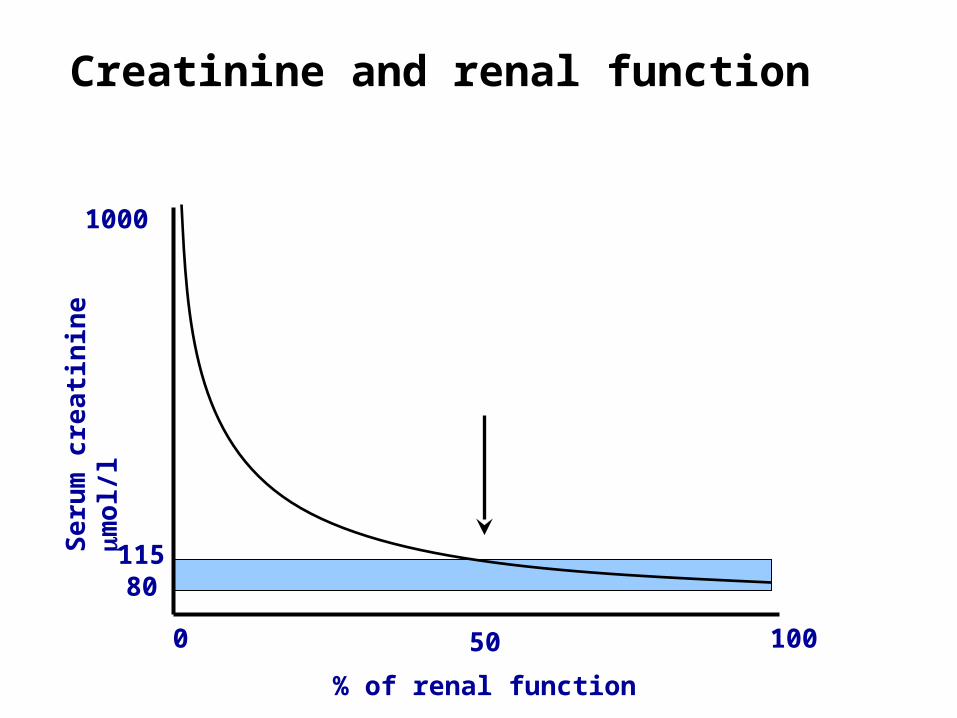
Creatinine and renal function
1000
Se
rum
cre
ati
ni n
e
mo
l/ l
11580
0 100
% of renal function
50

OutputKidney
PlasmaPoolContent
CreatinineInput
NormalMuscleMass
NormalKidneys
DiseasedKidneys
NormalMuscleMass
DiseasedKidneys
NormalKidneys
IncreasedMuscleMass
ReducedMuscleMass
Effect of Muscle Mass on Serum Creatinine

Creatinine 120 Weight 45kg
Age 75 yrs GFR 30mls/min
Creatinine 120 Weight 105kg
Age 35 yrs GFR 113mls/min

Complex assessment
• Isotopic measurement of GFR• Gold standard, but unsuitable for screening• Important if split function required
• Graph = Isotopic Glomerular Filtration Rate

eGFR

eGFR
Cockcroft-Gault Equation
Crcl (ml/min) = (140-age [years] x weight [kg])x1.23(x0.85 if female)
Serum Creatinine (micromol/l)
Abbreviated (four variable) MDRD Equation
GFR (ml/min/1.73m2) = 186 x (SCr)-1.154 x (age)-0.203 x (0.742 if female) x (1.210 if African American)

Modification of Diet in Renal Disease (MDRD) equation
• Derived from 1628 patients with clinically diagnosed CKD ( stage 3-4 CKD)
• eGFR ~ age, creatinine, gender,race
• Results standardised to BSA of average adult (1.73m2)
• Consistently performs well against gold standard
• Superior to Cockcroft-Gault or 24 hour urine collections
• Good internal consistency – Useful to track changes over time


Limitations of eGFR
• Accuracy - it is estimated90% of eGFRs are within 30% of true value– So 15 could be anywhere between 12-20– So 60 could be anywhere between 42-78
• More accurate for estimating low GFR– US, Australia & Scotland only report >60– UK report up to 89
Limitations of eGFR
Largely related to problems with creatinine
• Product of muscle metabolism – can not be used to assess renal function in:
• Malnourished / anorectics• Body builders • Children• Pregnant women• Amputees
• Tubular secretion and gi excretion increase at low GFR- so underestimates severe renal failure
• Trimethoprim and cimetidine block tubular secretion

Limitations of eGFR – variation in serum creatinine
– Laboratory assay– Biological variation (intra-individual variation in serum
creatinine concentration can be up to 5%)
– Fluid status– Diurnal variation (serum creatinine level peaks at 19:00
hrs)
– Delays in centrifugation of blood (>10 hours
associated with increase in serum creatinine)– Cooked Meat

Limitations of eGFR – variation in serum creatinine
• Ingestion of cooked meat meal increases serum creatinine level
• Absorption of serum creatinine from gut (converted from muscle creatine by cooking process)
• Can cause significant increase in serum creatinine (36-65% increase 2- 4 hours postprandially)
• Advise patients not to eat any cooked meat in the 12 hours before having blood test for eGFR
Influence of age on renal function
What is physiological?
What is ‘disease’?

Influence of age on renal function
• West Lincolnshire PCT
• Adult population 185 434
• 40 GP practices – 109 GPs
• All routine serum creatinine samples measured on population over 18month period (2005-6)

Age (years)
Number tested (% population)
CKD3 (%
population)
CKD4 (%populatio
n)
CKD5 (%populatio
n)
<20 688 (4.6%)
0 0.1 0
20-29 1989 (7.1%)
0.2 0.5 2.9
30-39 3159 (10.5%)
0.9 1.4 6.8
40-49 5466 (17.3%)
2.9 2.4 9.2
50-59 8461 (28.9%)
9.3 4.2 11.6
60-69 10905 (45.5%)
21.9 10.6 20.8
70-79 10064 (59.1%)
33.8 30.6 27.1
>80 6387 (60.8%)
31.1 40.0 21.7NDT 2008 23:556-561

Management of CKD in primary care
Aims of Management of CKD patients
• Slow progression– hypertension– proteinuria
• Manage cardiovascular risk– hypertension– proteinuria– statins/aspirin
• Manage renal-specific complications/risks– anaemia– bone disease– Diet
• Prepare for renal replacement therapy / conservative management
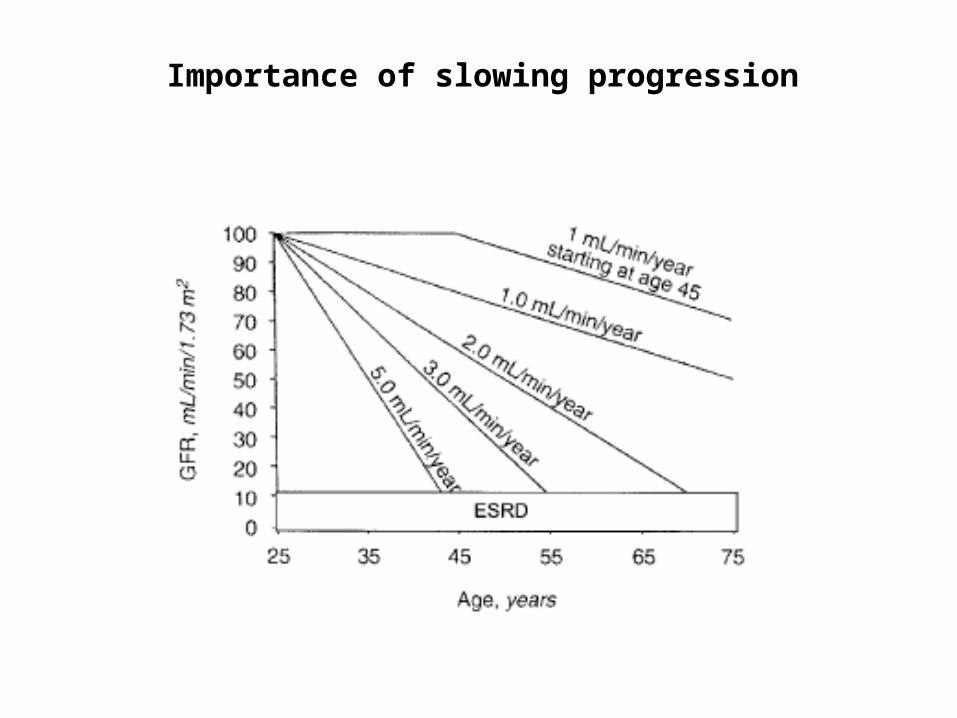
Importance of slowing progression

Proteinuria
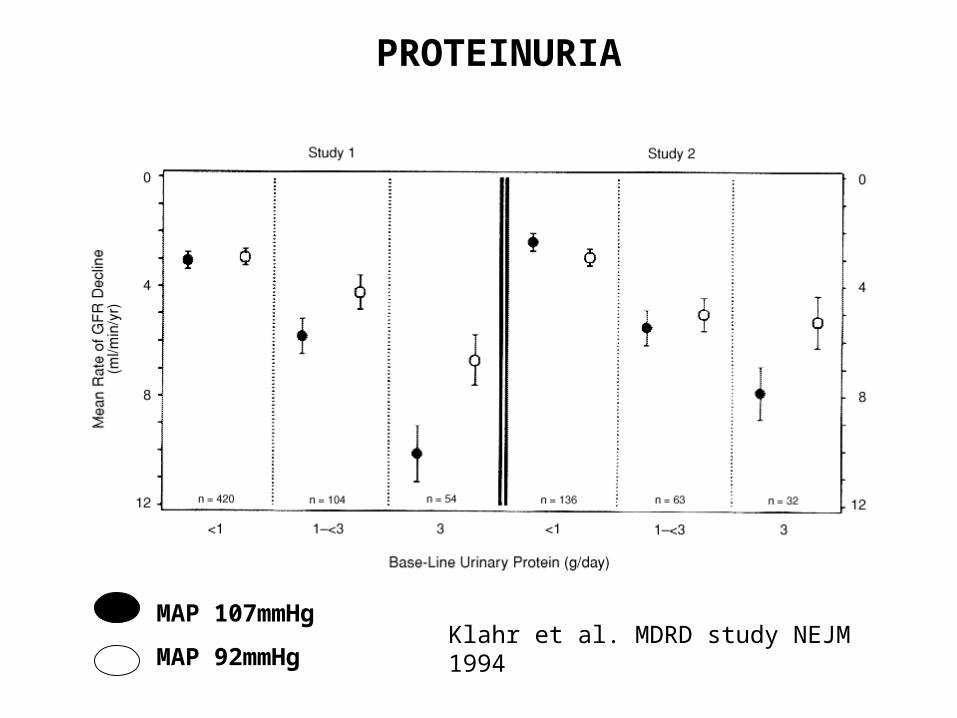
PROTEINURIA
Klahr et al. MDRD study NEJM 1994
MAP 107mmHg
MAP 92mmHg

Copyright ©2006 BMJ Publishing Group Ltd.
Tonelli, M. et al. BMJ 2006;332:1426
Fig 1 Time to clinical outcomes by proteinuria and kidney dysfunction

Copyright ©2006 BMJ Publishing Group Ltd.
Tonelli, M. et al. BMJ 2006;332:1426
Fig 2 Adjusted risk of all cause mortality according to proteinuria and kidney dysfunction

Screening for Proteinuria
Proteinuria
Urine dipstick - limitations
– rely on estimation of protein concentration
(dependent on urine flow rate)
- influenced by factors other than degree of proteinuria
e.g. false +ve: dehydration, exercise, infection, alkaline urine false –ve: excessive hydration
- predominantly sensitive to albumin not to total protein

Proteinuria
Current NICE guidelines
Use ACR in preference to PCR or urine dipstick to detect and quantify proteinuria in patients with CKD
If ACR <70mg/mmol or PCR<100mg/mmol confirm with emu sample
Indications for renal referral
ACR≥30mg/mmol or PCR≥50mg/mmol in assoc with haematuria
ACR ≥70mg/mmol or PCR≥100mg/mmol in absence of haematuria
N.B. Protein Creatinine Ratio (PCR) is different to Protein Creatinine
Index (PCI)
PCI = PCR x 10

Hypertension
• Well established that treatment of hypertension reduces CVD risk and slows progression of renal disease
• Now looking for “extra value”– blockade of renin / angiotensin / aldosterone


Guidelines for BP in Renal Disease
• Renal Association– 125/75 for CKD patients with proteinuria– 130/80 for non-proteinuric CKD patients– ACEi/ARB as first line
• NICE guidelines- Aim to keep SBP <140 (target range 120-139)
DBP <90
- Diabetic patients with CKD or proteinuria aim to keep SBP <130 (120-129) and DBP <80
- Offer ACEi and ARB if proteinuria (microalbuminuria in diabetes)

Antihypertensive agents
• Anti-proteinuric effect of ACEi and ARBs are equivalent
• Combination of ACEi/ARB is more anti-proteinuric than ACEi or ARB alone
• Non-dihydropyridine calcium channel blockers – diltiazem and verapamil have significant anti-proteinuric effects
• Dihydropyridine calcium channel blockers – amlodipine, nifedipine have no significant effect on proteinuria
• Sympathetic blockers e.g. methyldopa have little effect on protein excretion
• Beta blockers, diuretics and alpha blockers usually have a lesser anti-proteinuric effect

Aims of Management of CKD 3-5 patients
• Slow progression– hypertension– proteinuria
• Manage cardiovascular risk– hypertension– proteinuria – Statins/aspirin
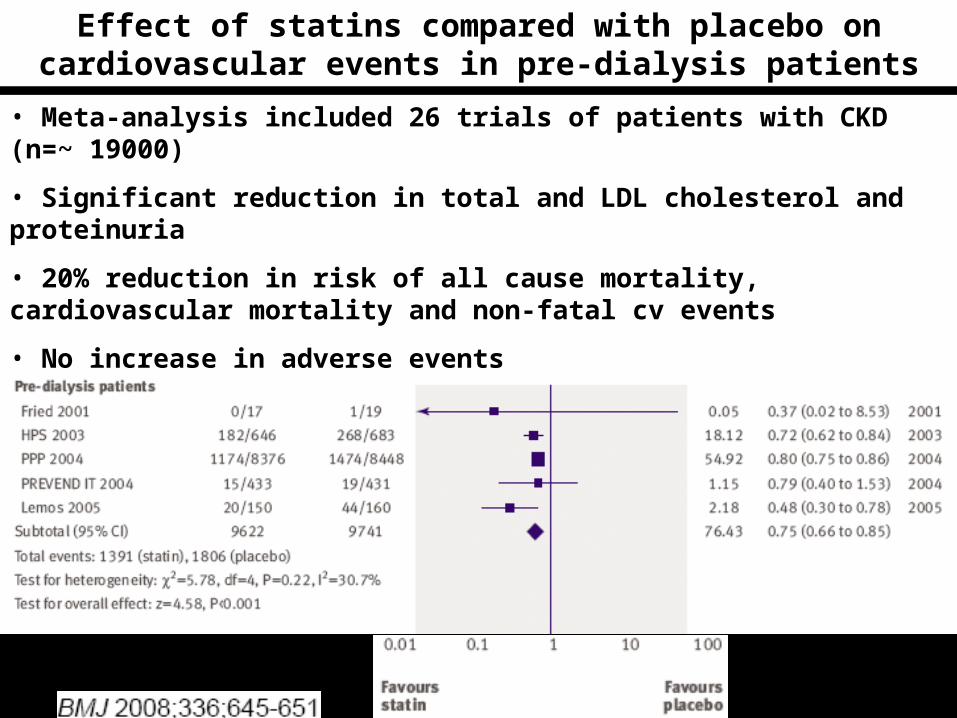
Effect of statins compared with placebo on cardiovascular events in pre-dialysis patients
• Meta-analysis included 26 trials of patients with CKD (n=~ 19000)
• Significant reduction in total and LDL cholesterol and proteinuria
• 20% reduction in risk of all cause mortality, cardiovascular mortality and non-fatal cv events
• No increase in adverse events

Monitoring
• Check eGFR - annually in all at risk groups- during intercurrent illness
• Stage 1 & 2 – 12 monthly• Stage 3a & 3b – 6 monthly• Stage 4 – 3 monthly• Stage 5 – 6 weekly
Management of CKD in primary care
• Address CV risk factors
• Avoid or minimise nephrotoxic drugs
• BP control
- Aim to keep SBP <140 (target range 120-139), DBP <90
- Diabetic patients with CKD or proteinuria aim to keep SBP <130 (120-129) and DBP <80
- Offer ACEi and ARB if proteinuria (microalbuminuria in diabetes)
• Regular monitoring – stage 1&2 – annual 3 - 6 monthly
4 – 3 monthly 5 – 6 monthly
• Immunization – influenza, pneumococcal
• Refer to renal team if progressive decline in renal function etc.
Summary
• Identification of patients with CKD is important
• Greatest risk for CKD patients is CVD
• Hypertension management is important, and part of a general CV disease management protocol
• Proteinuria is important prognostic indicator for renal and cardiovascular risk
• Angiotensin blockade (ACEi/ARB) is superior to other antihypertensives
• Targets are <140/90 or <130/80 in proteinuric/diabetic (high risk) patients
Who to refer?
If eGFR <60ml/min• Review previous creatinine/eGFR to assess rate of deterioration
• Repeat bloods within 1-2 weeks to exclude rapid progression if new finding
• Review medication, particularly recent additions
• Assess patient – urinary symptoms, palpable bladder, BP, hypovolaemia, heart failure, systemic symptoms
• Dipstick urine for blood and protein, send for ACR/PCR
• Bloods – FBC, calcium, cholesterol, HbA1c
• Renal USS
• Review need to refer for further assessment

Proteinuria
CKD - Who to refer?
• Malignant hypertension
• Hyperkalaemia (K+ >7mmol/l)
• Nephrotic syndrome
• Suspected underlying systemic illness
• Uncontrolled BP despite multiple (4) agents
• Isolated proteinuria (PCR >100mg/mmol, ACR >70mg/mmol)
• Haematoproteinuria (PCR>50mg/mmol, ACR >30mg/mmol)
• Declining eGFR >5-10ml/min/year
• Renal anaemia
• Stage 4 & 5 CKD (if appropriate)
• Suspected renal artery stenosis
• Diabetic patients with atypical features
Indicators of non-diabetic renal disease
• Absence of retinopathy (especially in type 1DM)
• Sudden rapid onset of significant proteinuria (urine ACR>70mg/mmol)
- duration of DM <5 years- abnormal evolution without transition through usual
stages
• Macroscopic haematuria
• Rapid decline in renal function or renal dysfunction without significant proteinuria
• >25% decline in eGFR post ACEi/ARB (RAS)
• Atypical biochemical/serological abnormalities

Guidelines
• Multiple sources – difficult to weigh thoroughness against usefulness - among the best are from renal association (www.renal.org) and follow the links
• www.ckdonline.org
• www.nice.org.uk/guidance

Renal Anaemia
• Very unusual to develop unless stage 4-5


Renal Anaemia
• Very unusual to develop unless stage 4-5
• Exclude other possible causes
• Optimise iron levels (ferritin 150-500, % hypochromic red blood cells <6%)
• Consider erythropoietin if remains anaemic despite being iron replete

RENAL BONE DISEASE
• Management aims to prevent development of:– metabolic bone disease– established hyperparathyroidism and parathyroid
hyperplasia
• Prevalence of vitamin D deficiency increases with age – 24% women aged >75 years are deficient
• NICE guidelines – routine measurement of calcium, phosphate and PTH not required in patients with stage 1-3b CKD, but to be measured in stage 4/5.

RENAL BONE DISEASE
• If concerns about vitamin D deficiency (diet/sunlight exposure/race/age) – check calcium and vitamin D levels and replace with cholecalciferol or ergocalciferol if vitamin D deficient.
• In stage 4/5 if PTH ≥3x upper limit of normal – indicator of secondary hyperparathyroidism, but intervention depends on calcium and phosphate level (i.e. is individual to specific patient)
