+ preconception health and racial/ethnic disparities in birth weight: a national study kelly l....
TRANSCRIPT
+Preconception Health and Racial/Ethnic Disparities in Birth Weight: A National Study
Kelly L. Strutz, MPHLiana J. Richardson, PhD, MPH
Jon M. Hussey, PhD, MPH
University of North Carolina at Chapel Hill3rd National Summit on Preconception Health and Health Care
June 13, 2011

+Introduction:
Evidence regarding the relationship between preconception health and birth outcomes is limited.
Even less is known about the contribution of preconception health to racial/ethnic disparities in birth outcomes.
This represents a critical gap in the knowledge base needed to inform MCH policy and practice.

+Study Questions:
How does preconception health impact birth weight?
Does preconception health contribute to racial/ethnic disparities in birth weight?
Does preconception health impact all racial/ethnic groups equally?

+Data and Analytic Sample:
National Longitudinal Study of Adolescent Health (Add Health), a nationally representative probability sample of US adolescents in the 1994-95 school year
Respondent interviews Wave I (1994-95): Adolescents in 7th-12th grades Wave III (2001-02): Young Adults aged 18-26 Wave IV (2007-08): Adults aged 24-32
Analytic sample 3046 singleton births conceived after Wave III and reported at Wave IV to non-Hispanic White, non-Hispanic Black,
Mexican-Origin Latina, and Asian/Pacific Islander mothers
+Measures and Analysis:
Infant birth weight Reported by respondentAdjusted for preterm birth
Preconception Health Indicators Cigarette smoking, alcohol
consumption, physical activity, and obesity status
Measured prospectively at Waves I and III
+Measures and Analysis:
Confounders Respondent’s age and parity at birth, nativity,
and early life SES
Mediators Respondent’s prenatal smoking and alcohol
consumption, and trimester began prenatal care
Statistical Analysis Univariate and bivariate analyses Linear regression Accounted for complex survey design

+Results: Mean Birth Weight (g)
Series12200
2400
2600
2800
3000
3200
3400
WhiteBlackLatinaAsian

+Results: Any Smoking

+Results: Heavy Drinking

+Results: Overweight/Obese

+Results: Physically Active

+Results: Contribution to Disparities
Model 1: Race/Ethnicity
Model 2: R/E + Smoking
Model 3: R/E + Smoking + Prenatal
Latina -- -- --
Black
Asian
Any Smoking
Wave I Only
Wave III Only -- --
Both Waves

+Results: Contribution to Disparities
Model 1: Race/Ethnicity
Model 3: R/E + Obesity
Model 4: R/E + Obesity + Prenatal
Latina -- -- --
Black
Asian -- --
Overwt/Obese
Wave I Only --
Wave III Only
Both Waves

+Results: Contribution to Disparities
Model 1: Race/Ethnicity
Model 6: R/E + Activity
Model 7: R/E + Activity + Prenatal
Latina -- -- --
Black
Asian
Physically Active
Wave I Only -- --
Wave III Only
Both Waves
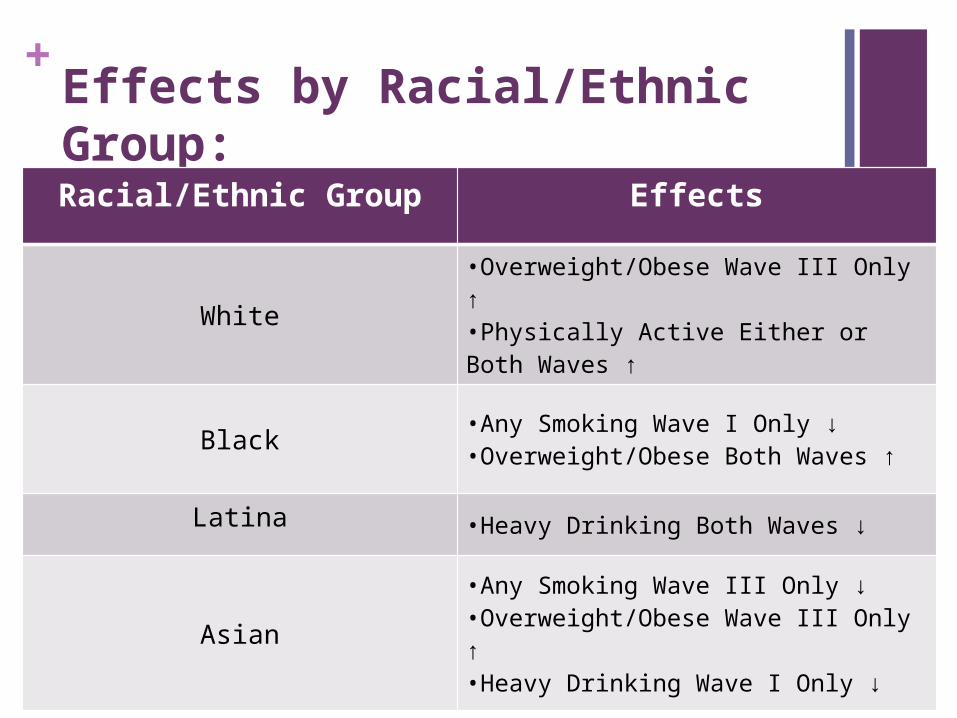
+Effects by Racial/Ethnic Group:Racial/Ethnic Group Effects
White•Overweight/Obese Wave III Only ↑•Physically Active Either or Both Waves ↑
Black •Any Smoking Wave I Only ↓•Overweight/Obese Both Waves ↑
Latina •Heavy Drinking Both Waves ↓
Asian•Any Smoking Wave III Only ↓ •Overweight/Obese Wave III Only ↑ •Heavy Drinking Wave I Only ↓

+Discussion:
FindingsOverall associations between birth
weight and preconception health indicators
Varied by racial/ethnic groupEffects of adjusting for preconception
factors on Black/White and Asian/White disparities in birth weight

+Discussion:
Strengths Prospective measures of preconception health
and subsequent birth weight Diverse national cohort
Limitations Adequacy of available data and measures
Public Health Significance Utility of applying a life course perspective Further research is needed to identify modifiable
preconception factors

+Acknowledgments Alexis Dennis and Chirayath Suchindran
This work was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development (grant numbers R01-HD057073, R01-HD058535, and T32-HD052468-02)
This research used data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (http://www.cpc.unc.edu/addhealth). No direct support was received from grant P01-HD31921 for this analysis.

+Contact
Kelly StrutzUniversity of North Carolina at Chapel HillCarolina Population CenterCB# 8120, University Square123 West Franklin StreetChapel Hill, NC [email protected]