pathways.lshtm.ac.uk [email protected] @ pathwaysncrm
DESCRIPTION
Allostatic load and health: a crossed-lagged analysis of the English Longitudinal Study of Ageing (ELSA) Sanna Read and Emily Grundy . http://pathways.lshtm.ac.uk [email protected] @ PathwaysNCRM. Allostatic load and health. - PowerPoint PPT PresentationTRANSCRIPT
Allostatic load and health: a crossed-lagged analysis of the
English Longitudinal Study of Ageing (ELSA)
Sanna Read and Emily Grundy
http://pathways.lshtm.ac.uk [email protected]
@PathwaysNCRM
Allostatic load and health
• Need for early indicators of health problems: self-rated health has been used as a predictor, but it is subjective measure → could allostatic load be one?
• Allostatic load is an objective composite measure of accumulated physical wear and tear (McEwen & Stellar, 1993).
frequent and long-term environmental demands → chronic stress→ early signs in primary mediators (stress hormones and anti-inflammatory cytokines) → activation of secondary outcomes (metabolic, cardiovascular and immune systems) → tertiary outcomes (poor health, diseases and eventually death)
• Previous research suggest that allostatic load could be a useful measure of early health problems, but very few longitudinal studies using repeated measures on the topic.
• Disablement process (Verbrugge & Jette ,1994) Pathological changes → Impairments → Functional Limitations → Disability
http://pathways.lshtm.ac.uk
Study direction of sequences
• Disablement process and accumulation of allostatic load assume a causal path between the factors.
• To study the directions longitudinal methods are needed.• An effective method to detect direction of sequences of
effects in longitudinal settings is to apply cross-lagged models.
http://pathways.lshtm.ac.uk
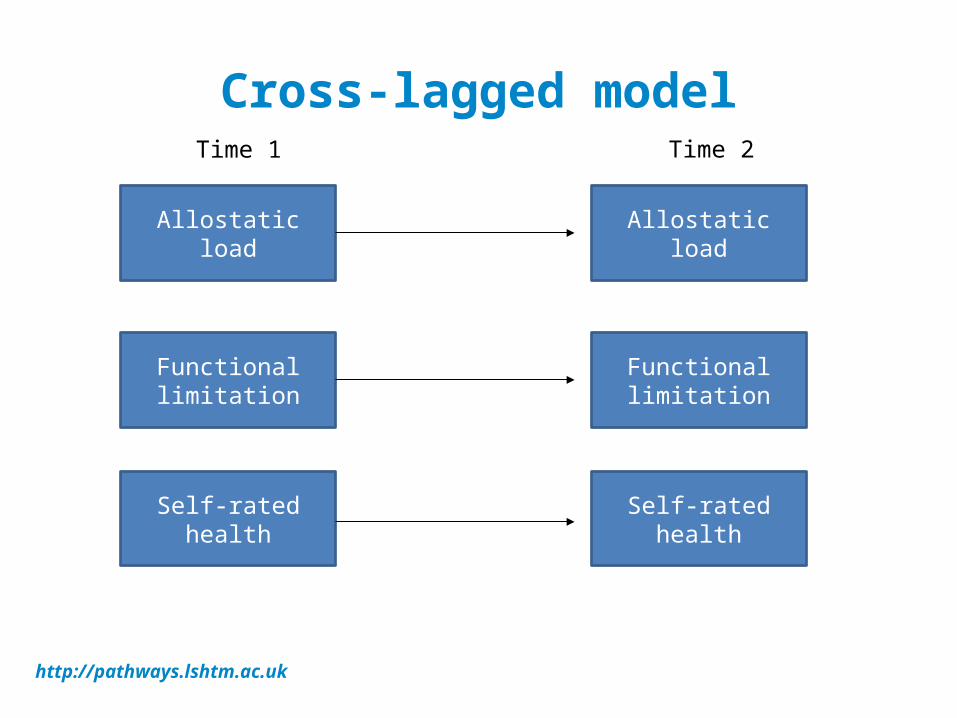
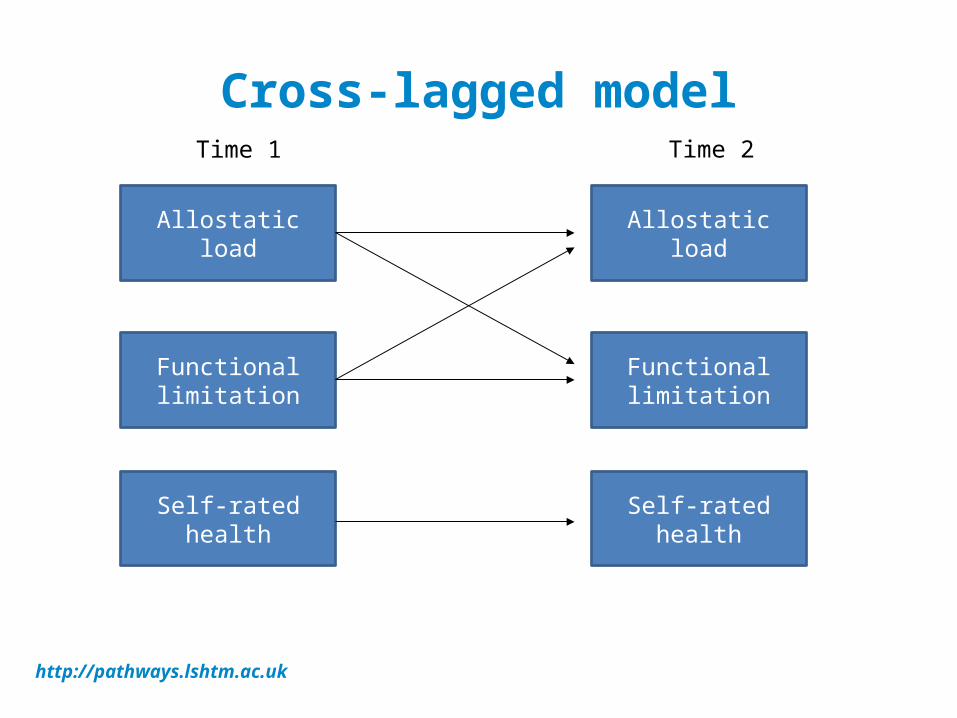
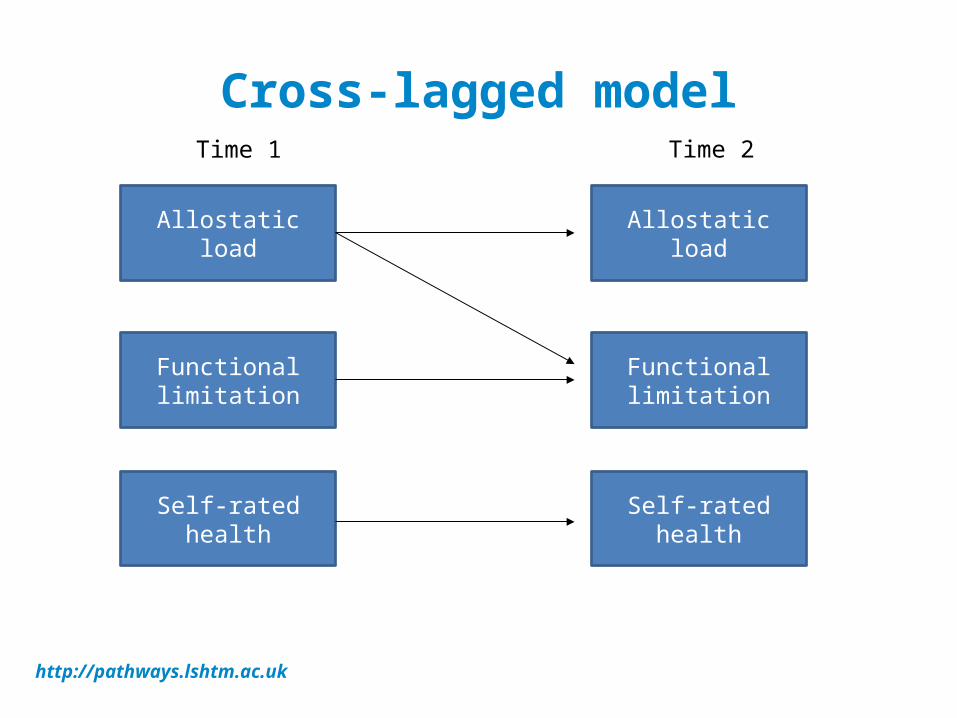
Cross-lagged model
http://pathways.lshtm.ac.uk
Functional limitation
Self-rated health
Functional limitation
Self-rated health
Time 1 Time 2
Allostatic load Allostatic load
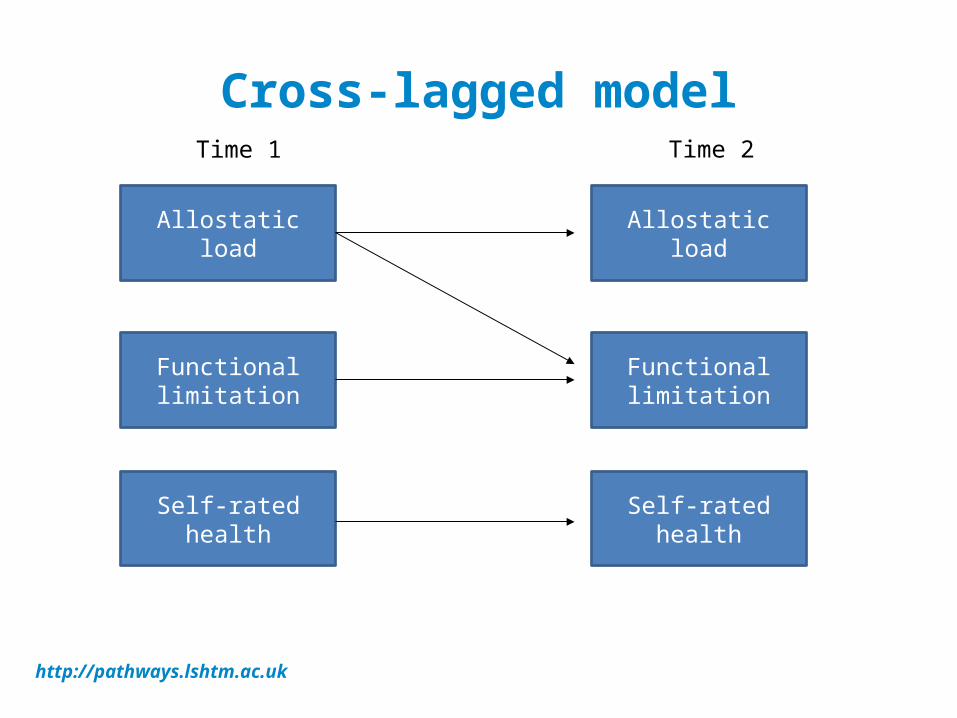
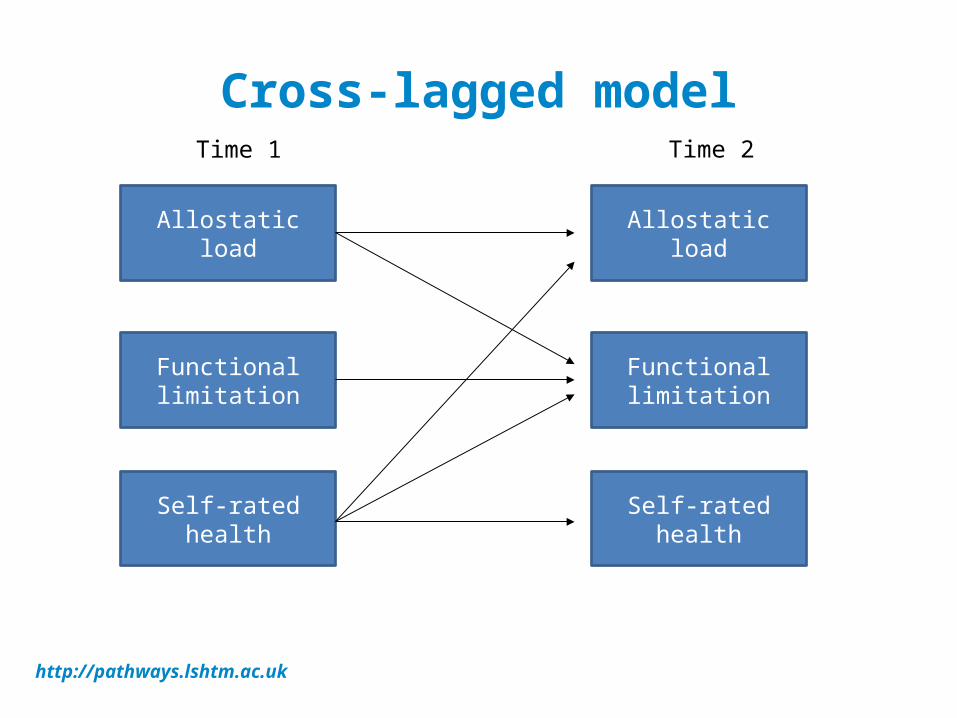
Cross-lagged model
http://pathways.lshtm.ac.uk
Functional limitation
Self-rated health
Functional limitation
Self-rated health
Time 1 Time 2
Allostatic load Allostatic load
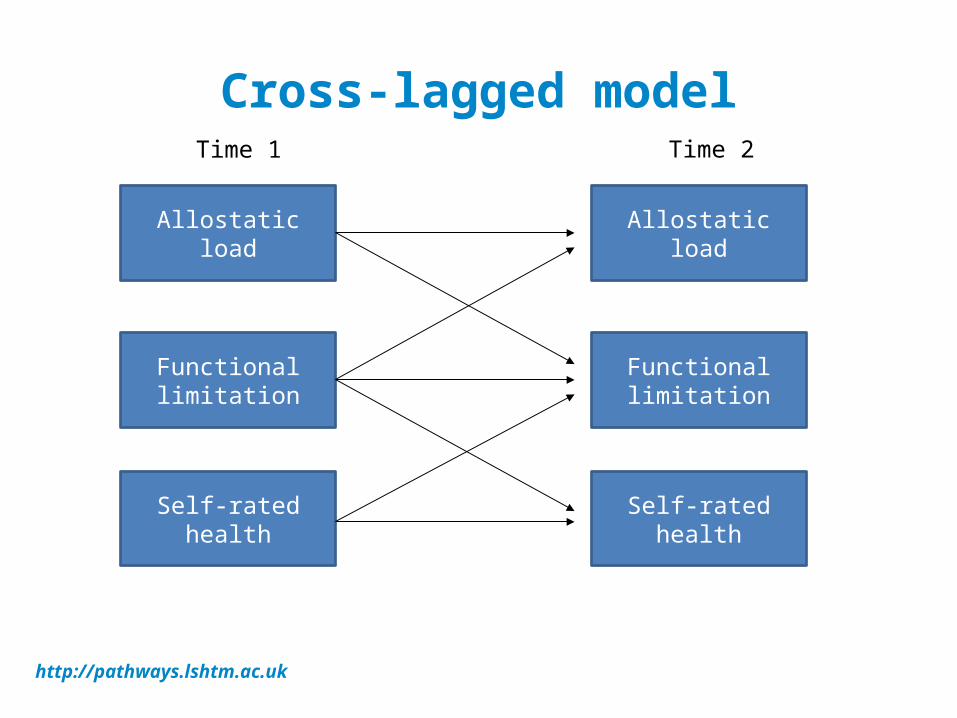
Cross-lagged model
http://pathways.lshtm.ac.uk
Functional limitation
Self-rated health
Functional limitation
Self-rated health
Time 1 Time 2
Allostatic load Allostatic load
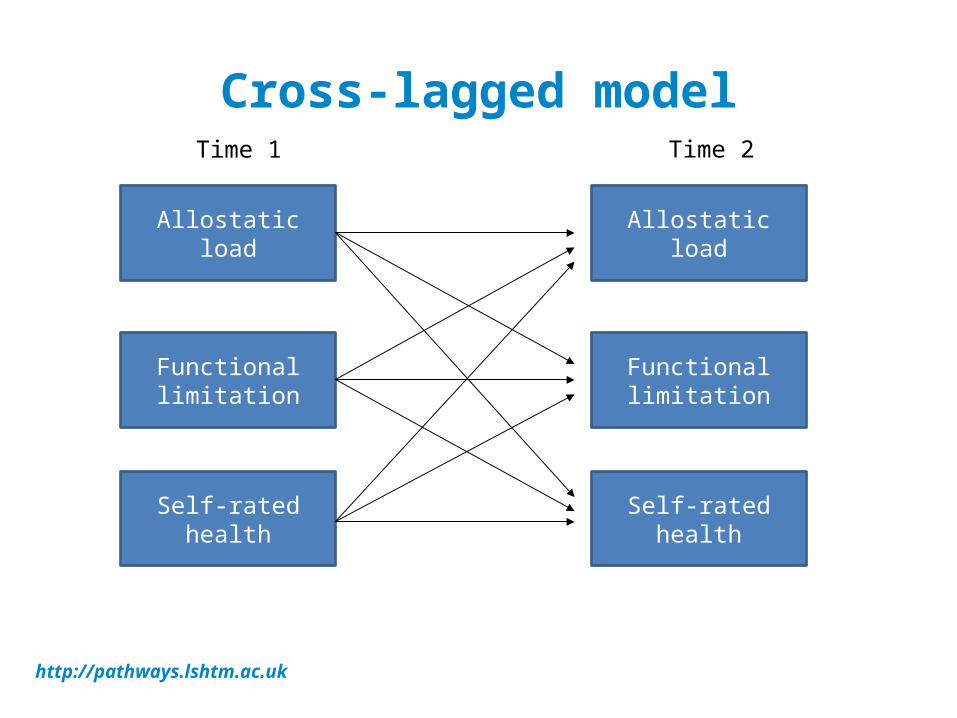
Cross-lagged model
http://pathways.lshtm.ac.uk
Functional limitation
Self-rated health
Functional limitation
Self-rated health
Time 1 Time 2
Allostatic load Allostatic load
Cross-lagged model
http://pathways.lshtm.ac.uk
Functional limitation
Self-rated health
Functional limitation
Self-rated health
Time 1 Time 2
Allostatic load Allostatic load

Aim
• To investigate the reciprocal association between allostatic load, self-rated health and walking speed as a measure of functional limitation.– allostatic load would predict functional limitation– the association between self-rated health and allostatic
load may be reciprocal or self-rated health may even precede allostatic load.
http://pathways.lshtm.ac.uk
Cross-lagged model
http://pathways.lshtm.ac.uk
Functional limitation
Self-rated health
Functional limitation
Self-rated health
Time 1 Time 2
Allostatic load Allostatic load

Aim
• To investigate the reciprocal association between allostatic load, self-rated health and walking speed as a measure of functional limitation.– allostatic load would predict functional limitation– the association between self-rated health and allostatic
load may be reciprocal or self-rated health may even precede allostatic load.
http://pathways.lshtm.ac.uk

Cross-lagged model
http://pathways.lshtm.ac.uk
Functional limitation
Self-rated health
Functional limitation
Self-rated health
Time 1 Time 2
Allostatic load Allostatic load
Cross-lagged model
http://pathways.lshtm.ac.uk
Functional limitation
Self-rated health
Functional limitation
Self-rated health
Time 1 Time 2
Allostatic load Allostatic load

Data
• English Longitudinal Study of Ageing (ELSA) waves 2 and 4 (2004 and 2008) - nationally representative survey of men and women aged 50+ (mean = 63, SD = 9.2 in wave 1). In the present study those aged 60+ in Wave 2 (n = 6132) were used (walking speed available only among 60+)
• Socio-demographic information and self reported health collected in all waves
• Detailed health data including biomarkers collected in alternate waves –biomarker data used to derive an index of allostatic load
http://pathways.lshtm.ac.uk

MeasuresHealth measures:
Allostatic load; self-rated health; walking speed (functional limitation) (Wave 2 and Wave 4)
Covariates:Age, gender, education (Wave 2)Married/not married; wealth; smoking; physical activity; social support; (Wave 2 and Wave 4)
http://pathways.lshtm.ac.uk
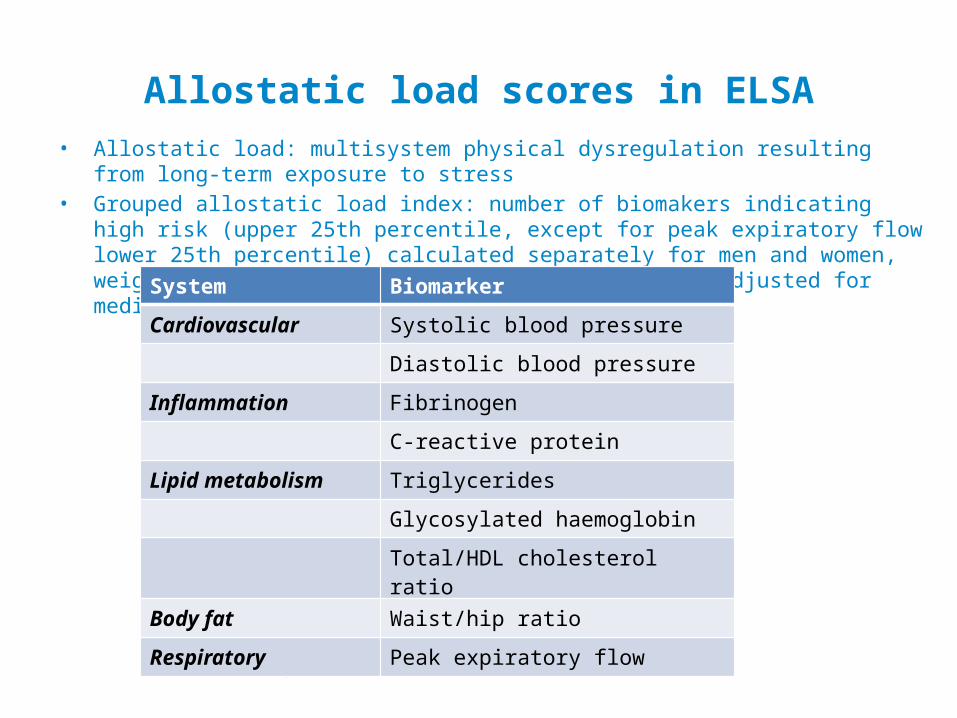
Allostatic load scores in ELSA• Allostatic load: multisystem physical dysregulation resulting from long-term exposure to stress• Grouped allostatic load index: number of biomakers indicating high risk (upper 25th percentile,
except for peak expiratory flow lower 25th percentile) calculated separately for men and women, weighted by the number of markers per system and adjusted for medication and fasting
http://pathways.lshtm.ac.uk
System Biomarker
Cardiovascular Systolic blood pressure
Diastolic blood pressure
Inflammation Fibrinogen
C-reactive protein
Lipid metabolism Triglycerides
Glycosylated haemoglobin
Total/HDL cholesterol ratio
Body fat Waist/hip ratio
Respiratory Peak expiratory flow
Self-rated health
Walking speed
Walking speed
Self-rated health
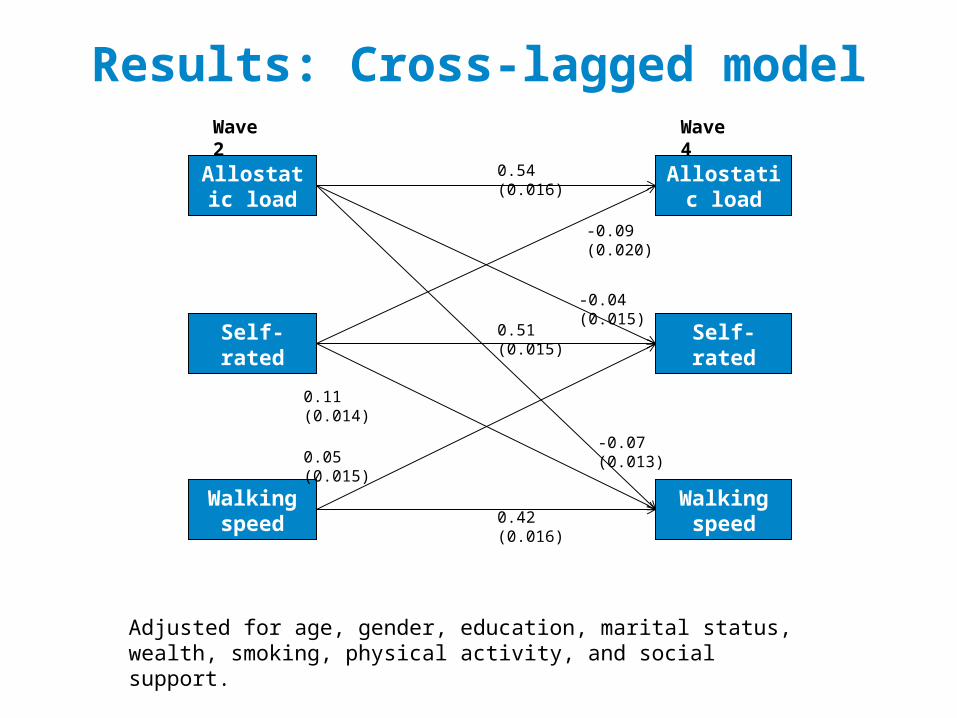
Wave 2 Wave 4
0.51 (0.015)
0.42 (0.016)
0.05 (0.015)
Allostatic load
Allostatic load
0.54 (0.016)
-0.09 (0.020)
-0.07 (0.013)
0.11 (0.014)
-0.04 (0.015)
Results: Cross-lagged model
Adjusted for age, gender, education, marital status, wealth, smoking, physical activity, and social support.
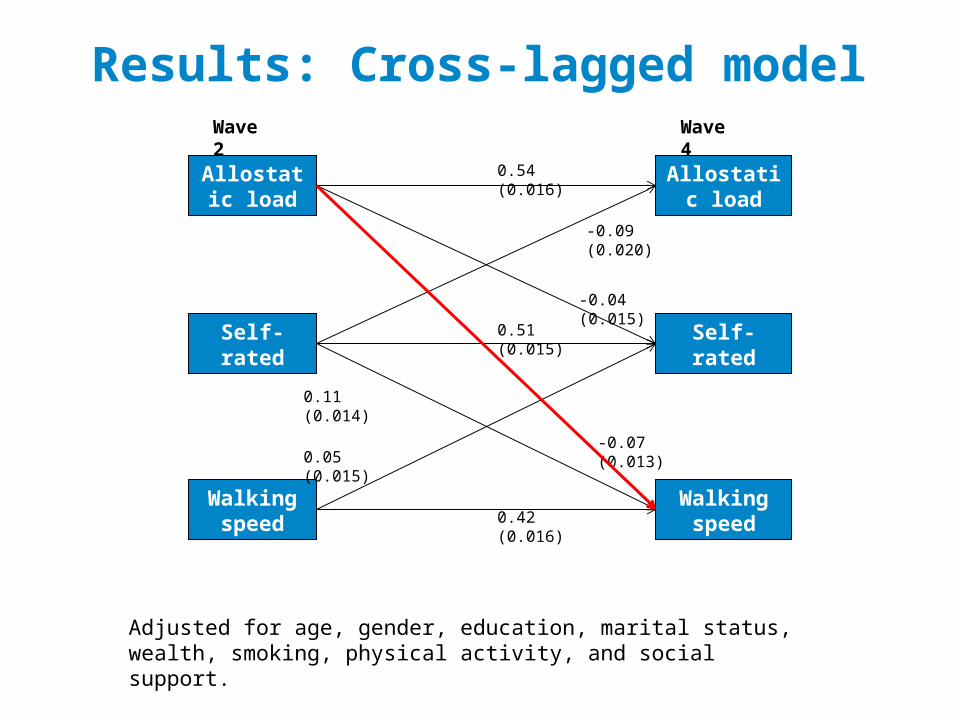
Self-rated health
Walking speed
Walking speed
Self-rated health
Wave 2 Wave 4
0.51 (0.015)
0.42 (0.016)
0.05 (0.015)
Allostatic load
Allostatic load
0.54 (0.016)
-0.09 (0.020)
-0.07 (0.013)
0.11 (0.014)
-0.04 (0.015)
Results: Cross-lagged model
Adjusted for age, gender, education, marital status, wealth, smoking, physical activity, and social support.
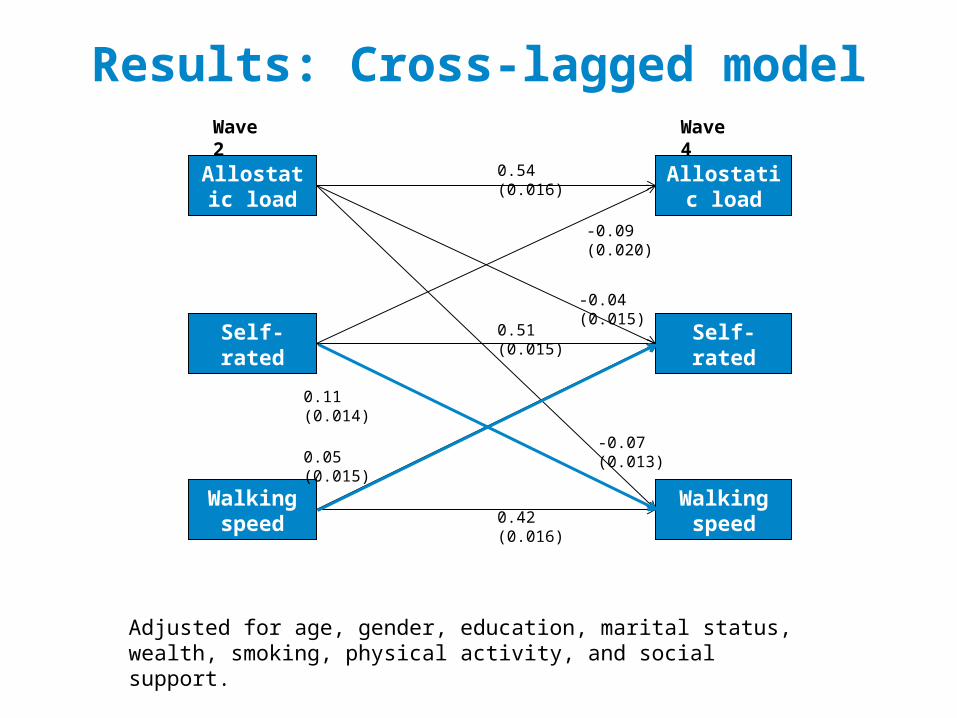
Self-rated health
Walking speed
Walking speed
Self-rated health
Wave 2 Wave 4
0.51 (0.015)
0.42 (0.016)
0.05 (0.015)
Allostatic load
Allostatic load
0.54 (0.016)
-0.09 (0.020)
-0.07 (0.013)
0.11 (0.014)
-0.04 (0.015)
Results: Cross-lagged model
Adjusted for age, gender, education, marital status, wealth, smoking, physical activity, and social support.
Conclusions & Discussion• Allostatic load predicts functional limitation
→ allostatic load may be a useful early objective indicator of health problems. The drawbacks of using it is that it is a complex composite measure which involves invasive data collection methods and therefore subject to refusal and drop-out. No standardized way of measuring it.
• The association between self-rated health and allostatic load and functional limitations were reciprocal, although the strength of the associations suggested that self-rated health may be an earlier indicator of health problems → The role of self-rate health in the disablement process seem to be less clear: it predicts better functioning, but it is also an outcome of good functioning. Self-rated health is simple and quick to use with high response rates. The limitations are its subjective content and variation from one population to another.
http://pathways.lshtm.ac.uk
Conclusions & Discussion• As hypothesised, allostatic load predicts later functional
limitations. In the future, it is important to include earlier indicators of chronic stress (neuroendocrine and inflammatory markers) and study longer time spans from middle adulthood to old age to detect the accumulation of stress.
http://pathways.lshtm.ac.uk
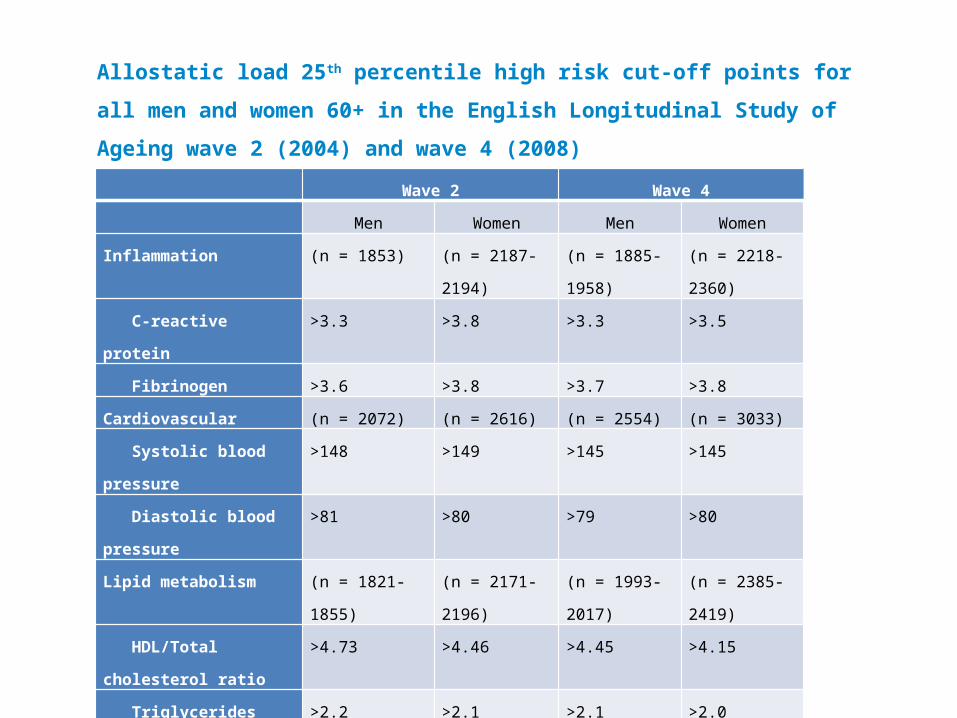
Wave 2 Wave 4
Men Women Men Women
Inflammation (n = 1853) (n = 2187-2194) (n = 1885-1958) (n = 2218-2360)
C-reactive protein >3.3 >3.8 >3.3 >3.5
Fibrinogen >3.6 >3.8 >3.7 >3.8
Cardiovascular (n = 2072) (n = 2616) (n = 2554) (n = 3033)
Systolic blood pressure >148 >149 >145 >145
Diastolic blood pressure >81 >80 >79 >80
Lipid metabolism (n = 1821-1855) (n = 2171-2196) (n = 1993-2017) (n = 2385-2419)
HDL/Total cholesterol ratio >4.73 >4.46 >4.45 >4.15
Triglycerides >2.2 >2.1 >2.1 >2.0
Glycosylated haemoglobin >5.8 >5.8 >6.1 >6.1
Body fat (n = 2304) (n = 2850) (n = 2653) (n = 3152)
Waist/hip ratio >1.00 >0.89 >1.00 >0.90
Respiratory (n = 2199) (n = 2642) (n = 2461) (n = 2882)
Peak expiratory flow <323 <208 <334 <214
Allostatic load 25th percentile high risk cut-off points for all men and women 60+ in the
English Longitudinal Study of Ageing wave 2 (2004) and wave 4 (2008)
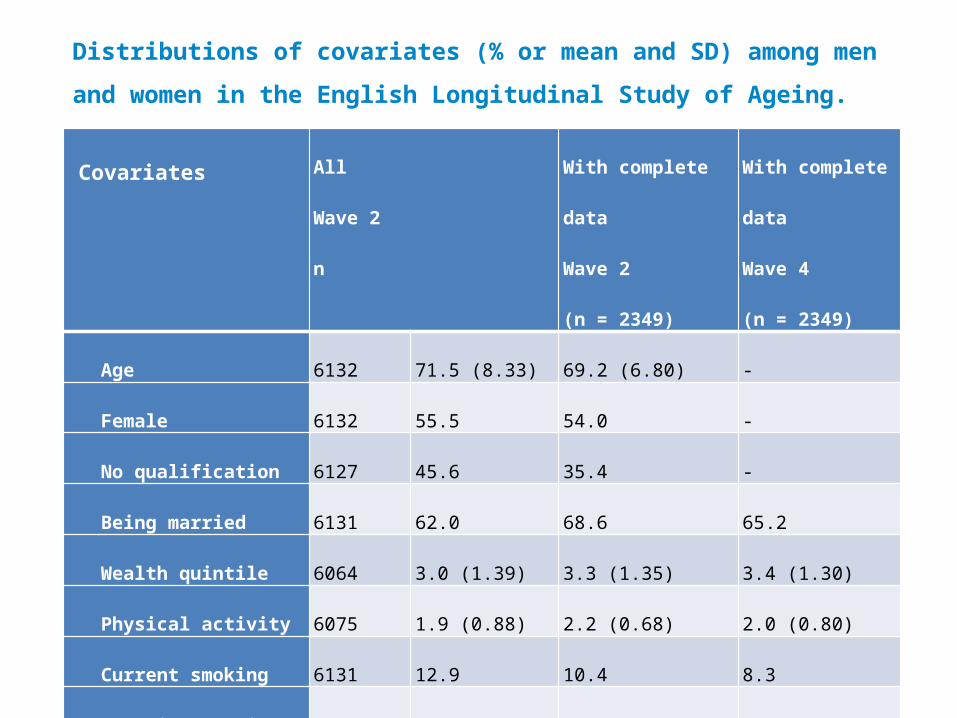
Covariates All
Wave 2
n
With complete data
Wave 2
(n = 2349)
With complete data
Wave 4
(n = 2349)
Age 6132 71.5 (8.33) 69.2 (6.80) -
Female 6132 55.5 54.0 -
No qualification 6127 45.6 35.4 -
Being married 6131 62.0 68.6 65.2
Wealth quintile 6064 3.0 (1.39) 3.3 (1.35) 3.4 (1.30)
Physical activity 6075 1.9 (0.88) 2.2 (0.68) 2.0 (0.80)
Current smoking 6131 12.9 10.4 8.3
Perceived social support 5399 4.2 (0.52) 4.2 (0.49) 4.2 (0.50)
Distributions of covariates (% or mean and SD) among men and women in the
English Longitudinal Study of Ageing.
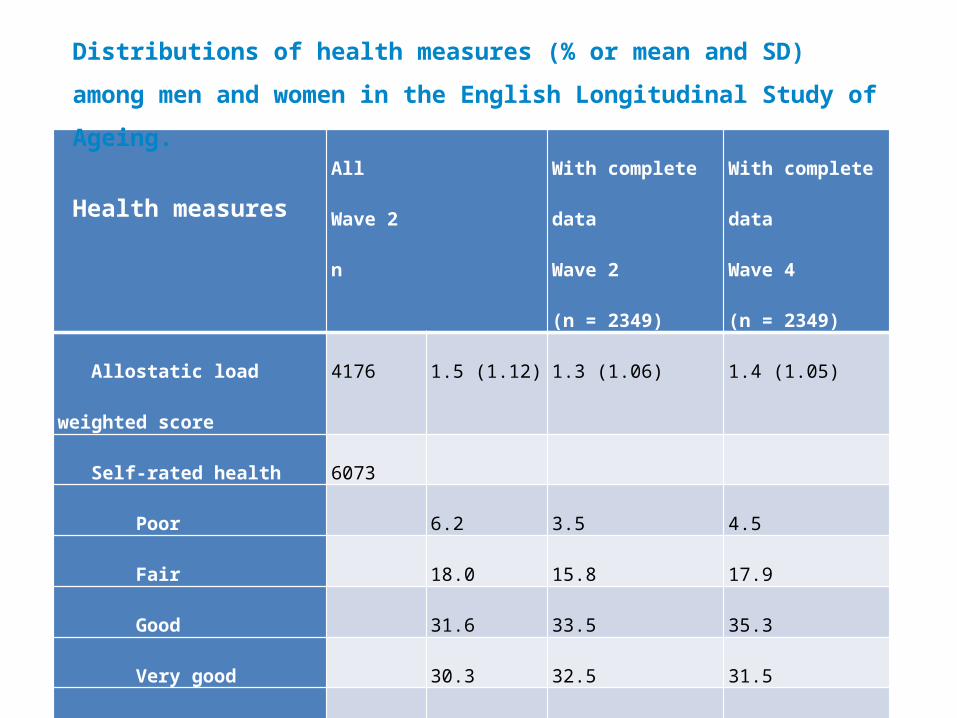
All
Wave 2
n
With complete data
Wave 2
(n = 2349)
With complete data
Wave 4
(n = 2349)
Allostatic load weighted score 4176 1.5 (1.12) 1.3 (1.06) 1.4 (1.05)
Self-rated health 6073
Poor 6.2 3.5 4.5
Fair 18.0 15.8 17.9
Good 31.6 33.5 35.3
Very good 30.3 32.5 31.5
Excellent 13.9 14.7 10.8
Walking speed (m/s) 5438 0.8 (0.28) 0.9 (0.25) 0.8 (0.26)
Distributions of health measures (% or mean and SD) among men and women in
the English Longitudinal Study of Ageing.
Health measures