بسم الله الرحمن الرحيم. pain management 1. pharmacotherapy salah n a el-tallawy...
TRANSCRIPT
بسم الله الرحمن الرحيم

PAIN MANAGEMENTPAIN MANAGEMENT
1. PHARMACOTHERAPY1. PHARMACOTHERAPY
Salah N A El-TallawyProf. of Anesthesia and Pain Management,
Faculty of Medicine, Minia University & NCI, Cairo University, Egypt
Associate Prof. KSU, KSA

Objectives
Introduction.
Pain control strategies.
Special painful conditions.
Rules for pharmacotherapy.
Algorithms for pain management.

“Pain is a Sensory and Emotional experience,
associated with actual or potential tissue
damage or described in terms of such damage”
(IASP)
What’s the definition of pain?
Pain is under-treated ???
Lack of Knowledge
Barriers:
in the health care
in the regulatory systems
with the patients

The “Costs” of Uncontrolled Pain
Stress response Hypothalamo-Pituitary-Adrenal axis: Disturbed cytokine cascade. Impairment of immune function. Increased catabolism. Negative nitrogen balance.
Pain Chronicity. Cardiovascular Respiratory GIT Neuro-psychiatric Impairment of mobility, Gait disturbances.

Peripheral Peripheral sensitizatiosensitizationn
CentralCentralSensitizatioSensitizatio
nn
• Tissue damageTissue damage
• Inflammatory Inflammatory soapsoap
• SympatheticSympathetic stimulationstimulation
• Nociceptive Nociceptive inputinput
• Excitability Excitability of DHNof DHN
• Mechanical Mechanical allodyniaallodynia
1ry 1ry Hyperalgesia Hyperalgesia
2ry2ry
HyperalgesiaHyperalgesia
Injury Injury or or
TraumaTrauma

Causes of Acute Pain Post-operative
Obstetric - Labor
Burns
Trauma
Infective / Inflammatory conditions
Ischaemic pain
Visceral pain

Causes of Post-Operative Pain
Incisional skin and subcutaneous tissue Deep cutting, coagulation, trauma Positional nerve compression, traction & bed sore. IV site needle trauma, extravasation, venous irritation Tubes drains, nasogastric tube, ETT Respiratory from ETT, coughing, deep breathing Rehab physiotherapy, movement, ambulation Surgical complication of surgery Others cast, dressing too tight, urinary retention

Causes of Chronic Pain
Cancer pain Cancer related From cancer therapy Cancer unrelated
Non-cancer Nociceptive Neuropathic Idiopathic

Good assessment = Successful management
Pain Assessment
NN
RR
SS

• Subjective:• Pain Scores:
• Unidimentional Acute pain• VRS, VAS & NRS.• Facial expression.
• Multidimentional Chronic pain• McGill & Pain Inventory.
• Objective:– Behavioral: refusal to move, cough & deep breath
– Physiological: PR, RR, ABP, sweatiness & dilated pupils
– Neuro-endocrinal: RBS, Stress hormones
– Algometry.
Pain Assessment

Numeric Rating Scale (NRS)
Visual Analogue Scale (VAS)
0 10
Pain Scores

Wong-Baker “Faces Scale”
Verbal scale
NoPain
Mild ModerateSeverePain


Questions to Ask about Pain
P A I N P A I N Pattern: onset, course & duration
Area: location
Intensity
Nature: burning, colic, …

Questions to Ask about Pain
P Q R S TP Q R S T (ECG format)
Provocation
Quality - characters of pain
Referred / Radiating
Severity
Timing

Questions to Ask about Pain
L O C A T E S L O C A T E S L – Location.
O – Other Symptoms.
C – Character: deep, burning, throbbing…
A – Aggravating and Alleviating factors.
T – Timing.
E – Effect: your daily routine?
S – Severity.

Personal opinion # Patient self report ?

–Pharmacotherapy– Anesthetic approaches– Implantable devices– Neurostimulation approaches– Alternative approaches– Surgical approaches– Rehabilitative approaches– Lifestyle changes– Psychological approaches
Pain Control Strategies

Drug Strategies Non Opioid Analgesics:– NSAA– NSAIDs
• Non-selective COX inhibitors• Selective COX-2 inhibitors
Opioids– Weak Opioids.– Strong opioids.– Mixed agonist – antagonists
Adjuvants– Antidepressants– Anticonvulsants– Substance P inhibitors– NMDA inhibitors– LA– Drugs for Headache– Drugs for Bone pain– Others .

Alternative medicine:– Acupuncture
– TENS
– Cupping
– Chiropractice
Physical Therapy– ice, heat, massage
Exercise Psychological therapy
– Cognitive-behavioral therapy
– Relaxation techniques
– Biofeedback
– Hypnosis
Non-Drug Strategies

WHO step Ladder
1 mild
2 moderate
3 severe
Morphine
Hydromorphone
Methadone
Pethidine
Fentanyl
Oxycodone
± Adjuvants
Codeine
Hydrocodone
Oxycodone
Dihydrocodeine
Tramadol
± Adjuvants
ASA
Acetaminophen
NSAIDs
± Adjuvants

1. Drug Therapy1) Non Opioid Analgesics:
– NSAAs
– Analgesic /Antipyretic e.g.
– Acetaminophen (COX-3 ---) & Antipyrine
– Analgesic/Anti-inflammatory/Antipyretic e.g.
– Salicylic acid
– NSAIDs
• Non-selective COX inhibitors
• Selective COX-2 inhibitors

Drug Name Usual Adult Oral Dose (mg)
Usual dose interval (Hrs)
Pediatric Dose (Mg/Kg)
Maximal Daily Dose (Mg/Day)
Other Comments
Aspirin 325-1000 4-6 10-15 g 4-6 4000 Not for use in children younger than 12 with possible viral illness due to Reye’s syndrome
Acetaminophen 500-1000 4-6 10-15 q 4-6 4000 Significant liver toxicity in overdose. May increase INR in patients taking warfarin.
Choline Magnesium Trisalicylate
1000-1500 12 25 bid 2000-3000 No effect on platelet function. Avoid in children younger than 12 with possible viral illness.
Ibuprofen 200-800 6 10 q 6-8 2400-3200 Relatively infrequent GI side effects
Naproxen 250-500 6-12 5 bid 750-1250 May be beneficial for headaches of migraines
Ketoprofen 12.5-50 6-8 Not recommended 300 Slightly increased GI side effects
Flurbiprofen 50-100 Bid-tid Not recommended 300 Potent anti-inflammatory properties
Oxaprozin 1200 24 Not recommended 1800 Onset delayed for 3-6 hours
Sulindac 150-200 Bid Not recommended 400 Prodrug with decreased GI side effects
Etodolac 200-400 6-12 Not recommended 1000 Balanced COX-1/COX-2 with decreased GI side effects
Indomethacin 25-50 8-12 Not recommended 100 Limit use to 2 weeks if possible
Ketorolac 30 mg IV/IM 6 None 120, except 150 first day
Efficacy similar to 4 mg morphine. Not for use for more than 5 days
Piroxicam 20 24 Not recommended 20 About half of patients intolerant of GI effects
Nabumetone 500-1000 12 Not recommended 2000 Low incidence of GI effects
Celecoxib 100-200 12-24 Not recommended 400 Primarily COX-2 inhibitor
Rofecoxib 12.5-50 24 Not recommended 50 Primarily COX-2 inhibitor. Increased incidence of cardiac events in VIGOR trial
Commonly Used NSAIDs

1.a.) NSAA - Acetaminophen• Acetaminophen blocks prostaglandin synthesis centrally
antipyretic effect.
• However, it does not act on prostaglandins peripherally
so it cannot block local inflammation.
• Clinical use:• Fever and mild pain• Can be used in children• Can be used during pregnancy & breast-feeding• May be used in combination with caffeine or propoxyphen• IV forms are available for post-op pain.
• Side effects:
• Long-term or large doses are both hepatotoxic and nephrotoxic.

Recently, COX-3 activity is selectively inhibited by
analgesic/antipyretic drugs such as acetaminophen,
phenacetin and
Inhibition of COX -3 could represent a primary central
mechanism by which these drugs decrease pain and
possibly fever
NSAA – AcetaminophenCOX-3 inhibitor

Salicylates (e.g. aspirin)
• Aspirine has:• Antipyretic and analgesic, • Anti-inflammatory actions (> 3 gm/d),• Anticoagulant.
• These actions result from the anti-PGs activity,
• Centrally and Peripherally.
• Unfortunately, these additional actions • GIT problems: gastritis, bleeding ulcer.

1.b.) NSAIDs
NSAIDs

NSAIDs
Blocks the production of Prostaglandin
Very effective in mild – moderate pain
Effective in other types of pain e.g. – Musculoskeletal pain
– OR & RA
– Cancer Pain
May be used alone or in combination with opioids

Practical guide for NSAID’s In Postoperative sitting:
Pre-op administration post-op pain.
– e.g. Leroxicam 8-16 mg IV or Celebrex 400mg, P.O. pre-op
Ketorolac & Leroxicam are effective in acute pain (IV)
Precautions:
– Gastric effects:
• PPI are the drugs of choice to treat gastric complications.
• H2 blockers only mask the disease
– Check the renal function routinely prior to administration
– COX2 inhibitors doesn’t affect the platelet function
Practical guide for NSAID’s Usage (Contin)
All specific or non-specific NSAID’s may cause:
Water retention and edema
Hypertension
Renal dysfunction
May delay bony fusion in chronic usage

Mechanism of Renal dysfunction: PGE2 and PGI2 are medullary VD. TXA2 is:
– cortical VC,
– regulate the renal vascular resistance and Renin secretion.
Both can influence:– The action of ADH.
– Loss of local renal Haemo-regulation (e.g. in hypotension)
– Reduction of GFR.
Electrolyte and Na imbalance. PGDs depletion can result in:
– Acute tubular necrosis & papillary necrosis,
– Interstitial nephritis
Practical guide for NSAID’s Usage (Contin)

Choice of NSAIDs
1. NSAIDs with Low Potency & Short t½
e.g. Ibuprofen
• Acute pain: 200 – 800 mg
• Chronic pain: 2 – 3 gm/day

Choice of NSAIDs
2. NSAIDs with High Potency & Short t½
e.g. Diclofenac• Less against COX-1 compared to COX-2
– Less GIT side effects.
• 1st pass metabolism – oral bioavailability 50% Liver toxicity.
– Other drugs: • Indomethacin• Ketoprofen

Choice of NSAIDs
3. NSAIDs with Intermittent Potency & t½
e.g. Naproxen
– Clinical use in:
• Migraine
• Musculoskeletal pain

Choice of NSAIDs
4. NSAIDs with High Potency & Long t½
e.g. Oxicams (melo-, piro- & teno-xicam).– They are not recommended in:
• Acute pain,• Pain of short duration
– Recommended in:• Inflammatory pain that persist for longer duration
– Arthritis & bone pain & cancer pain
– The High Potency & Long t½ of side effects• GIT & renal.

Selective COX-2 Inhibitors
Examples T-maz t½ Bioavail. Daily dose
Celecoxib 2-4 hs 9-15 hs 100 200 – 400 mg
Rofecoxib 2-4 hs 12 hs 100 25 mg
They are poor candidate for acute pain Effective in chronic pain e.g. OA & RA They are comparable to non specific NSAIDs More safe in elderly, GIT pts. More safe with other medications e.g. steroids & anticoagulants Less GIT toxicity ~ risk of CV events in pt at risk.

COX-2 inh. & GIT:– COX-1 confer cytoprotection in the GIT
– COX-2 inhibitors improve risk/benefit regarding GIT safety
COX-2 inh. & Kidney:– they do not spare kidney ~ edema & HP
COX-2 inh. & CVS: prostacyclin ++
– Do not – platelet COX-1
– ~ -- throm. /prost. balance thrombogenic risk– Some studies reported IHD in some pts received celecoxib.
Selective COX-2 Inhibitors

Drug Therapy
2. Opioids
- Weak Opioids.- Strong opioids.
- Mixed agonist – antagonists

Weak Opioids
e.g. Tramadol hydrochloride
– Potency: 100 mg equivalent to 100 mg pethidine.
– Dose 200 – 400 mg/d.
– Advantages:• Less postoperative respiratory depression.
• Efficient in reduction of postoperative shivering.
• Acute & Chronic pain
• Cancer & non cancer pain
– Side effects: Nausea and vomiting.

Strong Opioids
e.g. Morphine, Pethidine and Fentanyl. Duration of action is:
– Morphine: (10 mg) 3-4 hours.
– Pethidine: (100 mg) 3-4 hours.
– Fentanyl: (100 g) 45- 60 minutes.
Main side effects:– Nausea and vomiting.
– Respiratory depression.
– Extrapyramidal rigidity.

Agonist Antagonist Opioids
Members are:
– Butorphanol “Stadol” (2 mg)
– Nalbuphine “Nubain” (10 mg)
Duration of action is very short ( 2 hours).
Suitable to be used in infusion pumps and PCA.
Side effects: Hallucination is a famous one.
Opioid / Local Anesthetic Mixture
Epidural Marcaine and fentanyl is a useful mixture:
– Used epidurally
– Can be used in pediatrics.
– High quality of pain relief.
– Potentiation for action and duration.

Positioning of Opioid Therapy
Opioid therapy is the mainstay approach for
• Acute pain
• Cancer pain
• Pain in advanced illnesses
• Moderate - Severe non cancer pain
• AIDS pain

Opioid Therapy in Chronic Non-Cancer Pain
Under-treatment is a major problem because:• Published experience of multidisciplinary pain programs
showed that opioids associated with: • Poor function
• Psychiatric disorders
• Poor outcome
Consider the following:• Are opioids likely to work well? • Are there reasonable alternatives?• Are drug-related behaviors likely to be used?

Opioid Therapy:
Prescribing Principles Prescribing principles
1. Drug selection
2. Dosing to optimize effects
3. Route of administration
4. Treating side effects
5. Managing the poorly responsive patient
Opioid Therapy: 1. Drug Selection
Immediate-release preparations
– Used mainly
• For acute pain
• For stabilization phase
• For “rescue” dosing
– Can be used for long-term management in select patients

Immediate-release preparations
– Single-entity drugs e.g.
• Tramadol
• Morphine
– Combination products
• Codeine + ASA
• Propoxene + Acetaminophen.
Opioid Therapy: Drug Selection

Extended-release preparations
– Preferred because of improved pt’s compliance.
– Morphine, oxycodone, hydromorphone, codeine, tramadol,
buprenorphine
Fentanyl-TTS (72 hs).
Opioid Therapy: Drug Selection

2. Dose adjustments for opioids
Increase the dose (not the number of opioids) until:– pain relief is adequate or – intolerable side effects occur
Only one long acting opioid should be ordered at any
given time.– (e.g. Oramorph, Oxycontin, Duragesic)
Only one opioid combination should be ordered at any
given time.

3. Poor Opioid Responsiveness
If dose escalation adverse effects
– Strategy to lower opioid requirement• + Add non-opioid analgesic
• + Adjuvant analgesic
• + Non-pharmacologic strategy.
– Changes of opioid therapy:• Change the route: e.g. Spinal opioids
• “Opioid rotation”

4. Opioid Rotation
Based on inter individual variation in response to
different opioids
Reduce equianalgesic dose by 25%–50%:
– Reduce less if pain is severe
– Reduce less if same drug by different route
– Reduce less fentanyl
– Reduce more methadone (75%–90%)

5. The Equianalgesia
Drug Oral IV Duration
morphine 30mg 10mg 3-4h
hydromorphone 7.5mg 1.5mg 3-4h
codeine 200mg 130mg 3-4h
oxycodone 30mg - 3-4h
hydrocodone 30mg - 3-4h
meperidine 300mg 100mg 2-3h
• The amount (mg) required to deliver the same degree of analgesia varies from one opioid to another

TTS-Fentanyl dose based on oral morphine dose
Oral Morphine (mg/day)45 - 134135 - 224225 - 314315 - 404405 - 494495 - 584585 - 674675 -764765 - 854855 - 944 945 - 1034
1035 - 1124
TTS Fentanyl Patch25 g / hour50 g / hour75 g / hour
100 g / hour125 g / hour150 g / hour175 g / hour200 g / hour225 g / hour250 g / hour275 g / hour300 g / hour

6. Opioid Therapy: Side Effects Common
– Constipation
– Somnolence, mental clouding
Less common– N / V – Sweating
– Myoclonus – Amenorrhea
– Itch – Sexual dysfunction
– Urinary retention – Headache

Prevention # management of constipation
“The hand that writes the “opioid order”
also writes the bowel regimen”
In every patient receiving opioids
– Increase fluids and fibers
– Scheduled stool softeners/stimulant laxatives

Addiction
• It is associated with:
• Genetic, psychosocial, and environmental factors.
• It is characterized by behavioral changes:
• impaired control over drug use,
• compulsive use,
• continued use despite harm & craving.
• Quality of life is not improved

Tolerance
Tolerance is a state of adaptation; in which exposure
to a drug results in a diminution of the drug's effects
over time.
- 1st in duration of action;
- 2nd in overall effectiveness.

Pseudotolerance
Pseudotolerance is the need to increase due to other factors such as:
• disease progression,
• new disease,
• increased physical activity,
• lack of compliance,
• change in medication formulation,
• drug interaction.

Physical Dependence
Physical dependence is a state of adaptation that is manifested specific withdrawal syndrome that can be produced:
• by abrupt withdrawal,
• rapid dose reduction,
• decreasing blood level of the drug,
• or administration of an antagonist.

Opioid Pseudoaddiction
An iatrogenic syndrome in which patients develop
certain behavioral characteristics of psychological
dependence as a consequence of inadequate pain
treatment.

Drug Therapy
3. Adjuvant's Therapy

3. Adjuvant Therapy
Clonidine Anxiolytic drugs Anticonvulsants Antidepressants Ketamine LA Corticosteroids Others

Clonidine
Alpha-2 agonist.
Routes of adminstration: Oral, neuraxial & TTS
Pain control properties by itself
Excellent adjuvant for opioid dependent patients
Decrease the requirement of opioids
Decrease tolerance
Effective control for neuropathic pain
Caudal block for children 1g/kg pain relief / 24h

Ketamine NMDA receptors antagonist Neuropathic pain
Potent analgesic effect
Small doses in combination of opioids pain control
Post-op in chronic opioid users:
– Bolus dose of 100 g/kg followed by a continuous drip of 1-3
g/kg/min.

Anti-Convulsant Drugs in Pain
Gabapentin
Carbamazipine
Phenytoin
Depakine

Mechanisms of Anti-Convulsant Drugs in Pain

Usage of Anti-Convulsants Drugs in Acute Pain
Gabapentin: Mainly for neuropathic pain
Studies showed that:
– giving 600-1200 mg of Gabapentin 1 h pre-op.:• decreases the opioids requirement post-op &• better pain relief without increased sedation
– Combining Gabapentin + opioids is ideal for:• re-do back surgery cases • with chronic opioids usage
These class of drugs are also mode stabilizers

Antidepressant Drugs in Pain Managements
This type of drug may be divided into 4 categories:
1. Drugs that inhibit synaptic neurotransmitter reuptake.
2. Drugs that have direct receptor stimulation.
3. Drugs that produce receptor blockade.
4. Drugs that inhibit the activity of enzymes such as monoamine oxidase.

Mechanism of Action of Antidepressants
Name Dosage
Presynaptic Mechanism of
Action
Postsynaptic Mechanism of
Action Fluoxetine (Prozac) “SSRI”
20–80 mg Inhibits serotonin reuptake
Paroxetine (Paxil) SSRI
20–50 mg Inhibits serotonin reuptake
Mirtazapine (Remeron) 15–45 mg Stimulates norepinephrine and serotonin release
Blocks 5-HT2 and 5-HT3 receptors
Tricyclic antidepressant
10 – 50 mg inhibiting reuptakeof catecholamines, as well as indolamines

Adjuvant Analgesics for Musculoskeletal Pain
“Muscle relaxants”
Refers to numerous drugs: e.g.
cyclobenzaprine, orphenadrine, methocarbamol.
Centrally-acting analgesics.

Adjuvant Analgesics for Cancer Pain
For bone pain
– Bisphosphonates (e.g. pamidronate, clodronate),
– Calcitonin,
– Radiopharmaceuticals (e.g. Sr89, Sm153)
For bowel obstruction pain
– Anticholinergics, octreotide

Adjuvant Analgesics for Chronic Headache
Beta blockers
Anticonvulsants
Antidepressants
Alpha-2 adrenergic agonists
Vasoactive drugs
Triptans Mimic 5-HT involved in migraine Only indicated for migraine pain

Other Adjuvant Analgesics
Miscellaneous drugs Calcitonin
– RCTs in CRPS and phantom pain– Bone pain
Baclofen– RCT in trigeminal neuralgia– 30–200 mg/d or higher– Taper before discontinuation

NMDA-receptor antagonists
N-methyl-D-aspartate receptor involved in
neuropathic pain
Commercially-available drugs are analgesic:
ketamine, amantadine, dextromethorpan.
Other Adjuvant Analgesics

Topical Adjuvant Analgesics
For neuropathic pain
- Local anesthetics
• Lidocaine patch
• Cream: lidocaine 5%, EMLA
- Capsaicin
For musculoskeletal pains
• NSAIDs

Routes of Drug Administration Oral Rectal SQ IM IV TTS Neuraxial. Others

Routes of Administrations
Use the oral route whenever possible– Except e.g. post op period,
– Try other routes e.g.• buccal, sublingual, or rectal routes before initiating parenteral routes
Parenteral: – SQ and IV preferred &
– feasible for short-term therapy
Always avoid IM.
Oral and transdermal: preferred

I.M. not recommended but it is commonly used:– Painful
– Serum levels are unpredictable.
Rectal route:– For pediatric patients.
– Simple procedures.
– Slow absorption: longer duration.
Neuraxial: – Intrathecal generally preferred for long-term use
– Epidural for a shorter periods.
Routes of Administrations

Intravenous Route
Desired.
Easy titrated.
Serum level is controllable.
Can be used in:– drip form ,
– by pumps ,
– best is by PCA.
Routes of Administrations

Used for IV, SC & Epidural.
Pre-set by the physician.
Activated by the patient.
Programming modalities include:1. Loading dose or infusion.2. Demand bolus dose.3. Constant background infusion rate.4. Lock-out interval. 5. Maximum hourly dose. } Safety} Safety
Routes of Administrations - PCA

Advantages:
– Patients can titrate their own analgesia
– Improved:• Pain relief• Pulmonary function.
– Decreased:• Total daily dose.• Over sedation.• Postoperative complications.
Routes of Administrations - PCA

Non-permeable protective Non-permeable protective covercover
Drug Drug ReservoirReservoir
- Alcohol is added- Alcohol is added- Hydroxy-ethyl- Hydroxy-ethylcellulose matrixcellulose matrix
Rate controlling Rate controlling membrane membrane
Adhesive Adhesive layerlayer Protective Protective
LinerLiner
Transdermal Therapeutic System TTS
“Fentanyl-TTS”

TTS- Fentanyl
Dose
25g/hour
50g/hour
75 g/hour
100g/hour
Patch sizePatch size
10 cm10 cm22
20 cm20 cm22
30 cm30 cm22
40 cm40 cm22
CCmaxmax
ng/mlng/ml
0.3-1.20.3-1.2
0.6-1.80.6-1.8
1.1-2.61.1-2.6
1.9-3.81.9-3.8
TTmaxmax
Range in hoursRange in hours
26-7826-78
24-7224-72
24-4824-48
25-7225-72
Character of the patch:
• The composition of the patch/unit area is fixed (2.5 mg/10 cm2).• The dose is dependent upon the patch size.

Advantages of the TTS routeAdvantages of the TTS route
1. Reduction in the variability of in the plasma levels.
2. Avoidance of 1st pass metabolism.
3. Bioavailability: 92 %
4. Prolonged duration of action: 72 hrs.
5. Improved compliance.
6. Less side effects e.g. constipation.

Disadvantages of TTS-fentanyl
- It has a delayed onset of action (12-17 hours).
- The time to reach Cmax. is ranged from 26-72 hours.
- Followed by residual effects after removal of the patch
up to 17 hours.
Pain Management Algorithm

• Quality of pain.• Distribution of pain• Course.• Sleep disturbances• Mental changes• Drugs, toxins.• Alcoholism• Systemic illness• Trigger points
• Sensory examination: Pin prick, pain, T, Position, vibration.• Allodynia or Hyperalgesia• Motor examination: Strength, atrophy, fascisulations• Reflexes• Vasomotor changes
• EMG & NC study• Blood: CBC, FBS, ESR, B12, folate, heavy metals, immune fixation,• Electrophoresis.• Radiological.• Lumbar puncture• Nerve biopsy.
Initial Assessment
HistoryHistory Physical / Neurologic Physical / Neurologic examinationexamination InvestigationsInvestigations
Algorithm for Management of Neuropathic Pain

Central Pain
1st line therapy1st line therapy
2nd line therapy 2nd line therapy
• Mexiletine• SSRIs• Phenytoin• Lamotrigine
4th line therapy
3rd line therapy
Trigeminal Neuralgia Other Neuropathies
1st line therapy
2nd line therapy
• Carbamazepine
• Baclofen• Gabapentin• Lamotrigine • Valporate• Phenytoin
• Amitryptiline
• Opioids
3rd line therapy
• Gabapentin/TCA
• Carbamazepine• Tramadol• Capsaicin,lidocain
• Mexiletine
Anticonvusants:• Carbamazepine• Gapapentine• Valporate
Algorithm for Management of Neuropathic Pain
El-Tallawy

Trauma pain management Algorithm
Trea t w ith an ym od a lit ies
C lear m en ta ls ta tu s
S m all d oses o fop io id s (cod e in e )o r/w ith K e to ro lac
U n c lear m en ta ls ta tu s
H ead in ju ryp a tien ts
Head Injury

E p id u ra l an a lg es iaop io id s o r
loca l an es th e tics
B on e in ju ry
E p id u ra l an a lg es iaO p io id s on ly
P C A
yes
E p id u ra l op io id sw ith o r w ith ou t
loca l an es th e tics
P erip h era ln erve b lock
N o
N erve fu n c tionm on ito rin g
P erip h era l n erve o r vascu la rin ju ry
E xtrem ity in ju ry
Trauma pain management Algorithm
Extremity Injury

E p id u ra l an a lg es ia
S u rg ery req u ired
P C A
S u rg ery n o t rq u ired
A b d om in a l in ju ry
Trauma pain management Algorithm
Abdominal Injury
P C A
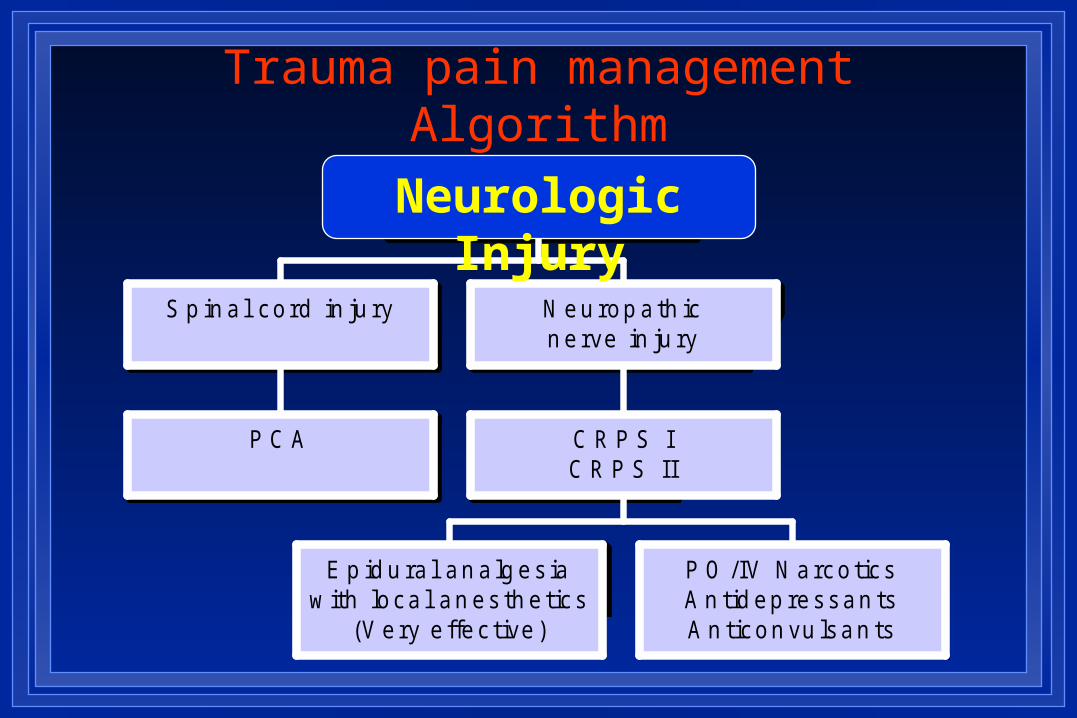
S p in a l co rd in ju ry
E p id u ra l an a lg es iaw ith loca l an es th e tic s
(V ery e ffec tive )
P O /IV N arco tic sA n tid ep ressan tsA n ticon vu lsan ts
C R P S IC R P S II
N eu rop a th icn erve in ju ry
N eu ro log ic in ju ries
Trauma pain management Algorithm
Neurologic Injury

Th orac ic ep id u ra lan a lg es ia
In te rcos ta ln erve b lock
P C A
R ead y fo rextu b a tion
IV n arco ticsP C A
In tu b a tedp a tien ts
Th orac ic ep id u ra lan a lg es ia
In te rcos ta ln erve b lock
P C A
N ot In tu b a tedp a tien ts
Th orac ic trau m a
Trauma pain management Algorithm
Thoracic Injury

Summary of Pain Management
…the basics

Do Not Use Placebos!
Unethical
They don’t work
Not helpful in diagnosis
Effect is short lived
Destroys trust

Match the therapy to the type of pain Intensity of pain
– Mild, moderate or severe.
Type of pain e.g.– Somatic & Visceral pain # Neuropathic pain
Duration of pain– Continuous # intermittent pain.
Acute # chronic Drug combinations
– Never order more than one SR preparation at a time
– Only one combination analgesic should be ordered at a time
Basics of Pain Management
1st step: is the good pain assessment.
Pain medications must be taken:
when the pain is first perceived.
Doses of opioids are increased:
with the patient’s report of pain
Adjuvant medications are used for:
opioid non-responsive & neuropathic pain.
Non-pharmacologic approaches are always a part of any pain management protocol.

Pain Management in the late 18th century

“By any reasonable code, freedom from pain should be a basic human right, limited only by our knowledge to achieve it ...”
Wall P & Melzack R 1987

