“ frontotemporal dementia and related disorders : organic psychoses?”
DESCRIPTION
Diana De Ronchi , Anna Rita Atti. “ Frontotemporal Dementia and Related Disorders : Organic Psychoses?”. Ferrara, 26 ottobre 2012. Outline. FTD “Psicosi organiche” AD/Psicosi – Psicosi/AD. - PowerPoint PPT PresentationTRANSCRIPT
“Frontotemporal Dementia and Related Disorders: Organic Psychoses?”
Ferrara, 26 ottobre 2012
Diana De Ronchi , Anna Rita Atti
Outline
FTD “Psicosi organiche” AD/Psicosi – Psicosi/AD
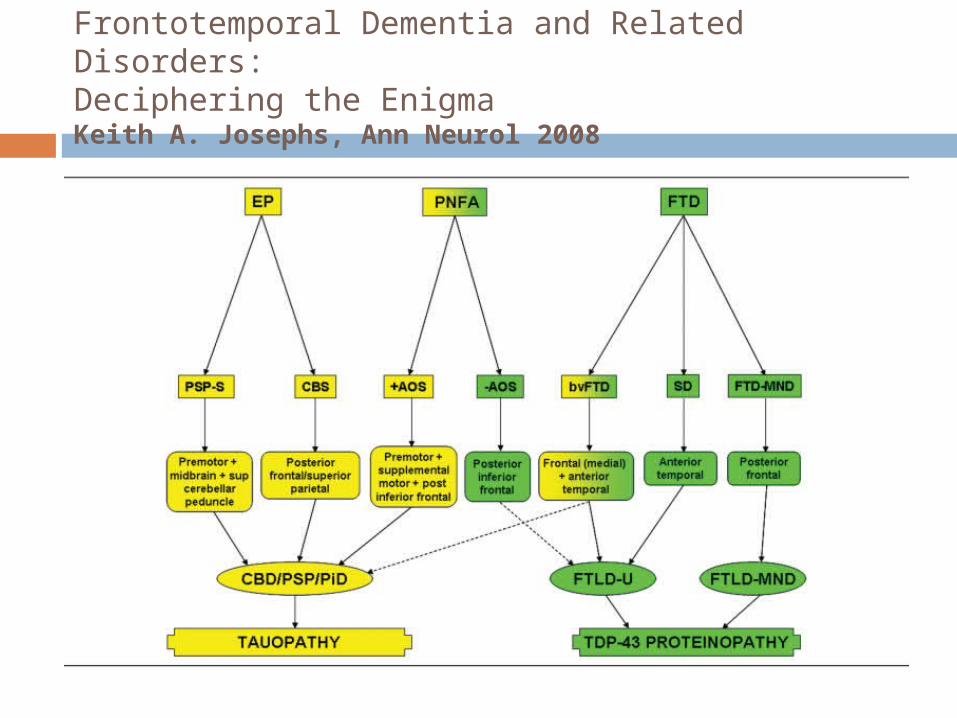
Frontotemporal Dementia and Related Disorders: Deciphering the EnigmaKeith A. Josephs, Ann Neurol 2008
FTD is an umbrella term that includes a number of different syndromic variants, all characterized by the presence of behavioral and personality changes ±aphasia.
bvFTD (behavioral variant) SD (semantic dementia) and FTD-MND (FTD with motor neuron
disease)
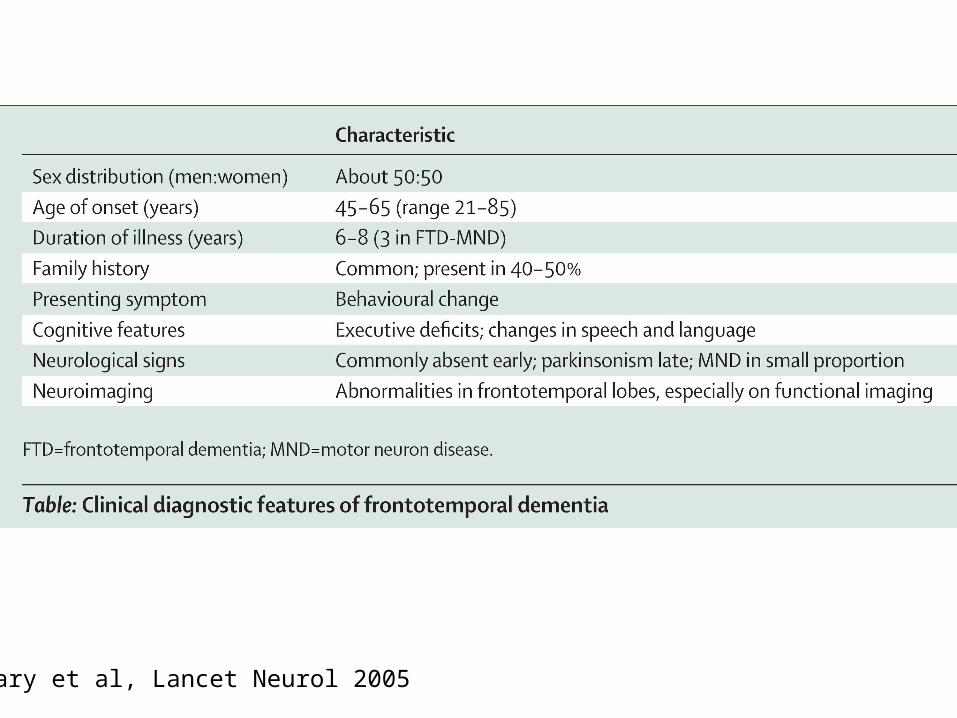
Neary et al, Lancet Neurol 2005
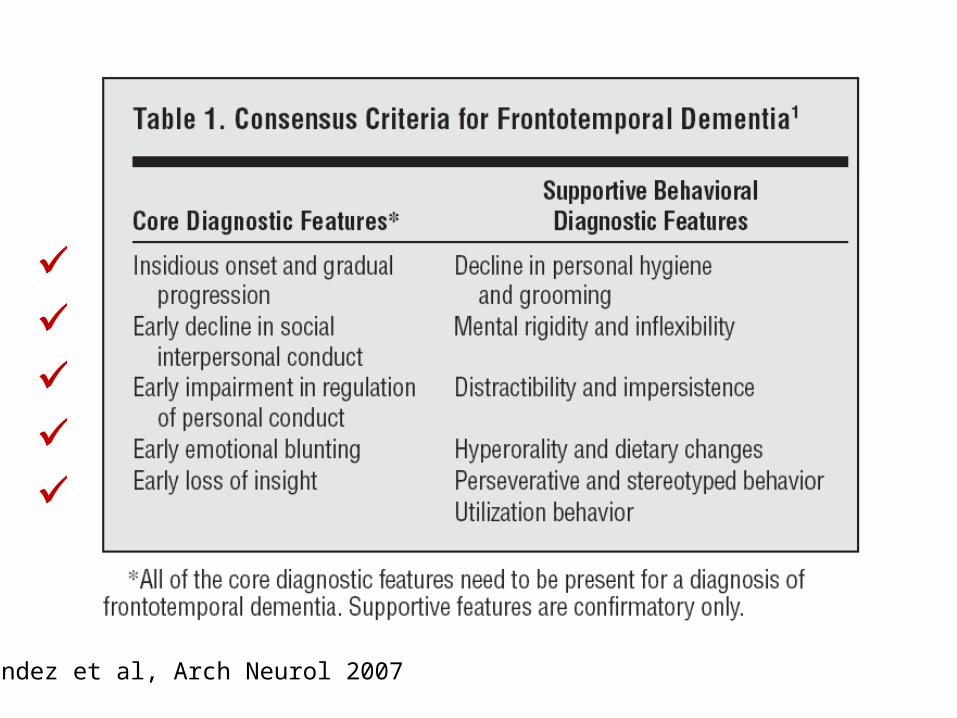
m m M m m
Mendez et al, Arch Neurol 2007
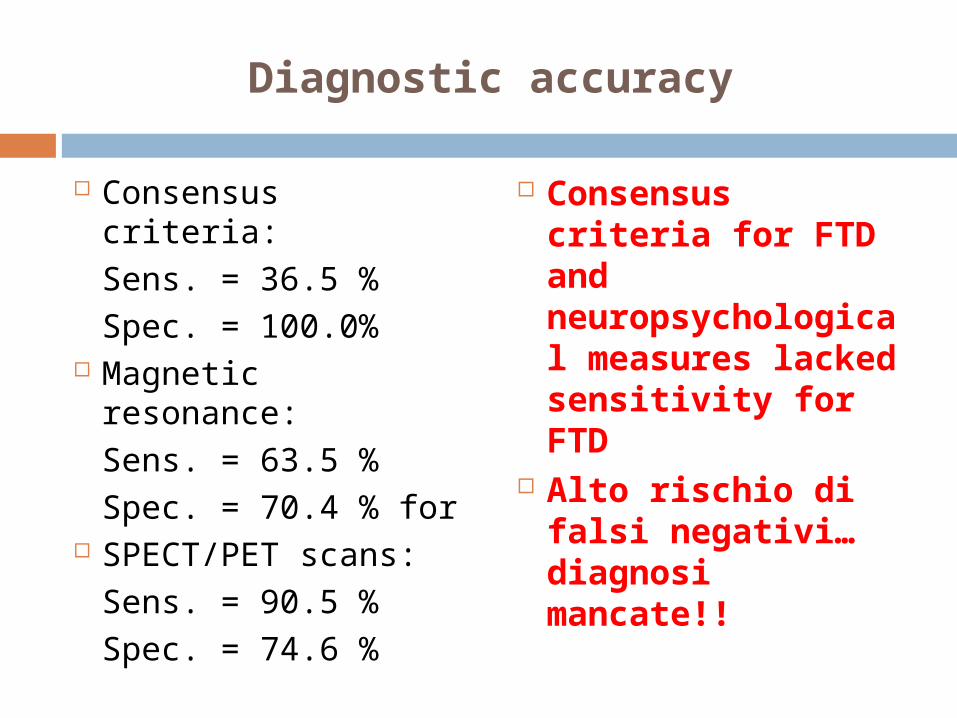
Diagnostic accuracy
Consensus criteria:Sens. = 36.5 %Spec. = 100.0%
Magnetic resonance:Sens. = 63.5 % Spec. = 70.4 % for
SPECT/PET scans:Sens. = 90.5 % Spec. = 74.6 %
Consensus criteria for FTD and neuropsychological measures lacked sensitivity for FTD
Alto rischio di falsi negativi…diagnosi mancate!!
FTD presenting as schizophrenia-like psychosis
organic psychoses, secondary schizophrenias Symptomatic schizophrenias
5 of 17 patients with FTD had presented with a psychosis (schizophrenia/schizoaffective disorder n=4, bipolar disorder n=1) an average of 5 years prior to the dementia diagnosis
Literature review: 828 cases of frontotemporal dementia in 205 publications.
Velakoulis, D. et al. The British Journal of Psychiatry 2009;194:298-305

Patients with psychosis were younger at onset (40.2 years v. 52.4 y) and experienced a longer delay between onset and subsequent presentation (11.3 years v. 2.2) compared with the larger frontotemporal dementia group.
Prevalence of schizophrenia-like psychosis in patients with frontotemporal dementia
Velakoulis, D. et al. The British Journal of Psychiatry 2009;194:298-305

Explaining the findings: more than a frontotemporal coincidence?
non-specific, psychotic response to insult by the developing (young) brain
i.e. the occurrence of a pathological process in the same brain regions of young adults leads to a similar clinical phenotype
interaction between neuropathology and normal central nervous system development
shared localisation of brain pathology
Velakoulis, D. et al. The British Journal of Psychiatry 2009;194:298-305

Despite the strong evidence for frontotemporal deficits in schizophrenia, few modern authors have drawn parallels between schizophrenia and frontotemporal dementia
subgroup of patients who are diagnosed with schizophrenia have an insidious, slowly evolving FTD associated with motor neuron disease like pathology beginning in the hippocampus
Finally...
Velakoulis, D. et al. The British Journal of Psychiatry 2009;194:298-305

Possible explanations for cognitive decline with
neuroleptics
Neuroleptics –through D2 receptor antagonism?- reduce the expression of Brain Derived Neurotrophic Factor increase in senile plaque and neurofibrillary tangle (Chlan-Fourney et al, Brain Res 2002)
Anti-muscarinic agents increase tangles (Perry et al, Ann Neurol 2003)
Outline
FTD “Psicosi organiche” AD/Psicosi – Psicosi/AD
Systemic Medical Conditions for Organic Psychoses:
Systemic infections: HIV, Mono, Hepatitis Endocrine: Thyroid, Parathyroid,
Cushings, Addison’s, Pituitary Adenoma Vitamin Deficiencies: B12, Folate, Niacin Uremia, Dialysis Acute Intermittent Porphyria
Neurological Conditions for Organic Psychoses:
Parkinson’s, Huntington’s (basal ganglia) Stroke, Tumor, Trauma, Infections Autoimmune: Multiple Sclerosis, Lupus Migraine headaches Dementia Sensory deprivation or over-stimulation
(“ICU psychosis”)
Variety of substances (over-the-counter, Prescription, Recreational, and toxins) may cause psychosis
Substance-Induced Psychosis

Sedative/Hypnotics: Barbiturates Benzodiazepines (withdrawal) Alcohol (withdrawal)
Steroids and Hormones: Oral Contraceptive Pills Prednisone Corticosteroids Anabolic steroids
Substance-Induced Psychosis
Substance-Induced Psychosis
Stimulants: amphetamine, cocaine, ephedra
Analgesics Antimicrobials Antidepressants (rarely) Antihistamines, anticholinergics Thyroid hormones Antiparkinsonian agents: L-dopa,
bromocriptine, amantadine, etc Cardiovascular Drugs
Mental Disorders with Psychosis:
Autism Mental Retardation Obsessive Compulsive Disorder with
Poor Insight Post-Traumatic Stress Disorder Malingering (Simulazione)
Outline
FTD “Psicosi organiche” AD/Psicosi – Psicosi/AD
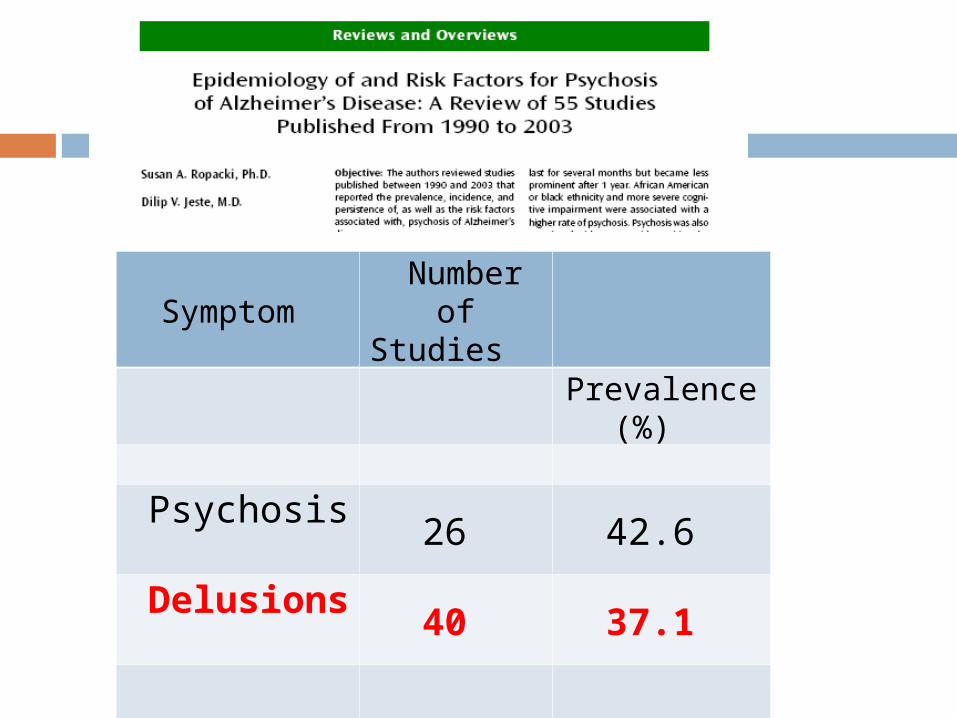
Symptom Number of Studies
Prevalence (%)
Psychosis 26 42.6
Delusions 40 37.1
Hallucinations 39 19.9
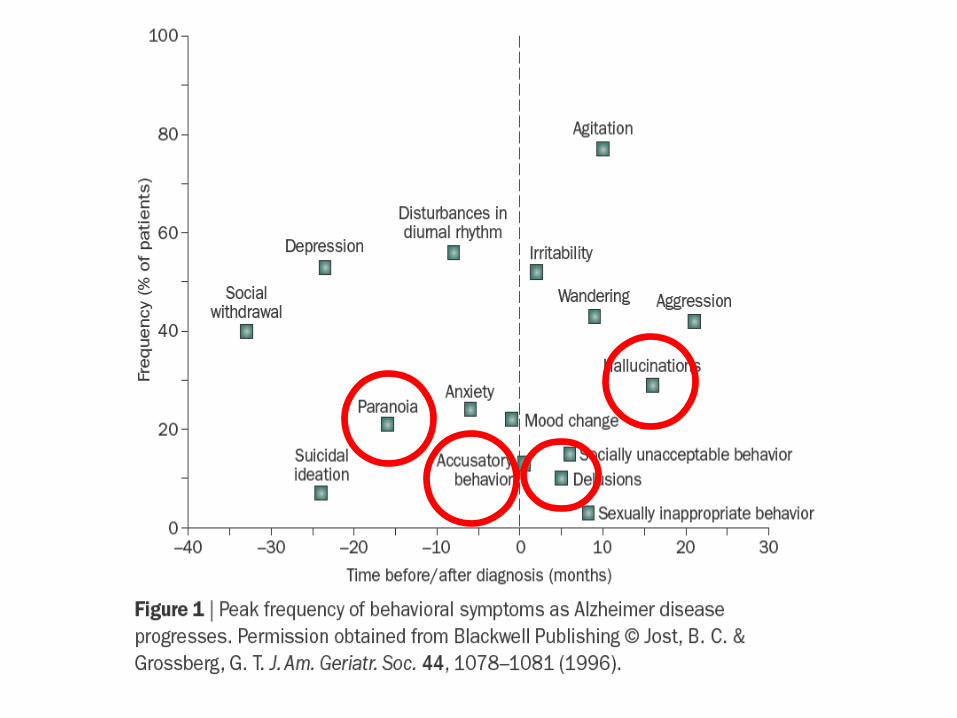

the delusions in AD are typically paranoid type, non-bizarre and simple Misidentification phenomena belief that people are stealing things from
them, that they are in danger and/or others are planning to harm them, that their spouse and/or other caregiver is an imposter (or not who they say they are), that their house is not their home, that their spouse is having an affair, that their family members are planning to abandon them, that unwelcome guests and/or television figures are actually present in the home

Ropacki & Jeste, Am J Psych 2005
Is psychosis a possible risk factor for dementia?
evidence that patients with psychosis of AD show a more rapid cognitive decline (role of AP?)
Is psychosis an early symptom of dementia? subjects with late-onset acute and transient
psychosis are at 11 times higher risk of subsequently getting a diagnosis of dementia (Kørner et al, 2009)
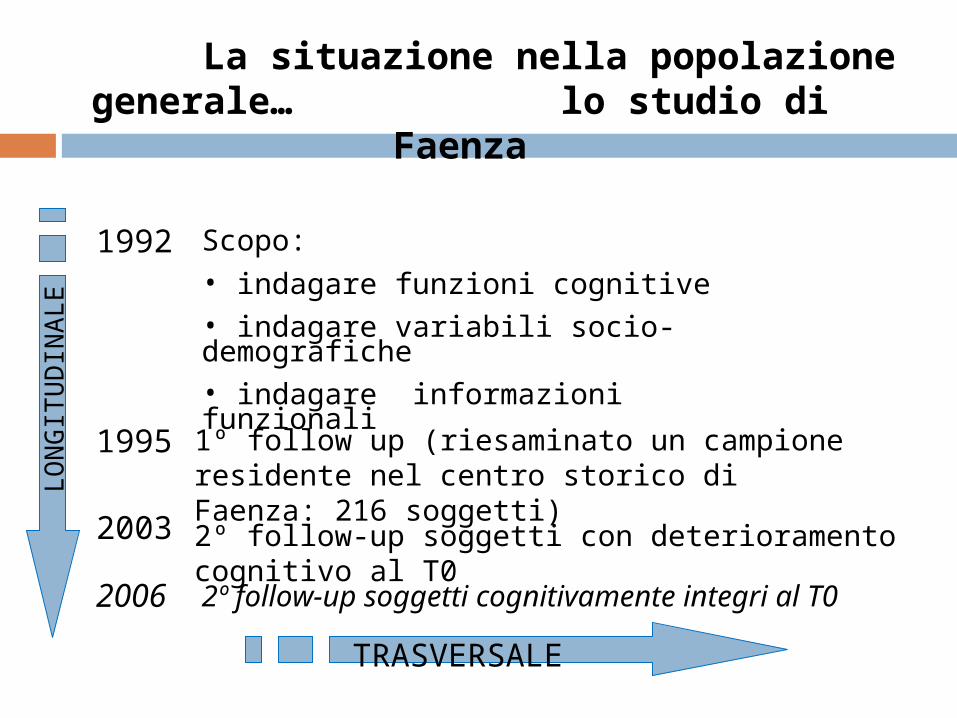
La situazione nella popolazione generale… lo studio di Faenza
1992
1995
2006
TRASVERSALE
LO
NG
ITU
DIN
AL
E
Scopo:
• indagare funzioni cognitive• indagare variabili socio-demografiche • indagare informazioni funzionali
1º follow up (riesaminato un campione residente nel centro storico di Faenza: 216 soggetti)
2º follow-up soggetti cognitivamente integri al T0
2003 2º follow-up soggetti con deterioramento cognitivo al T0
OBIETTIVO
Stimare la prevalenza di: Demenza Episodio Depressivo Maggiore (MDE) Disturbo d’Ansia Generalizzato
(GAD) Sintomi Psicotici Ideazione Suicidaria Abuso Alcolico

Prevalenze dei disturbi
4,2
19 20
0
5
10
15
20
25
DEPRESSIONEMAGGIORE
DEMENZA ANSIA GENERALIZZATA
p
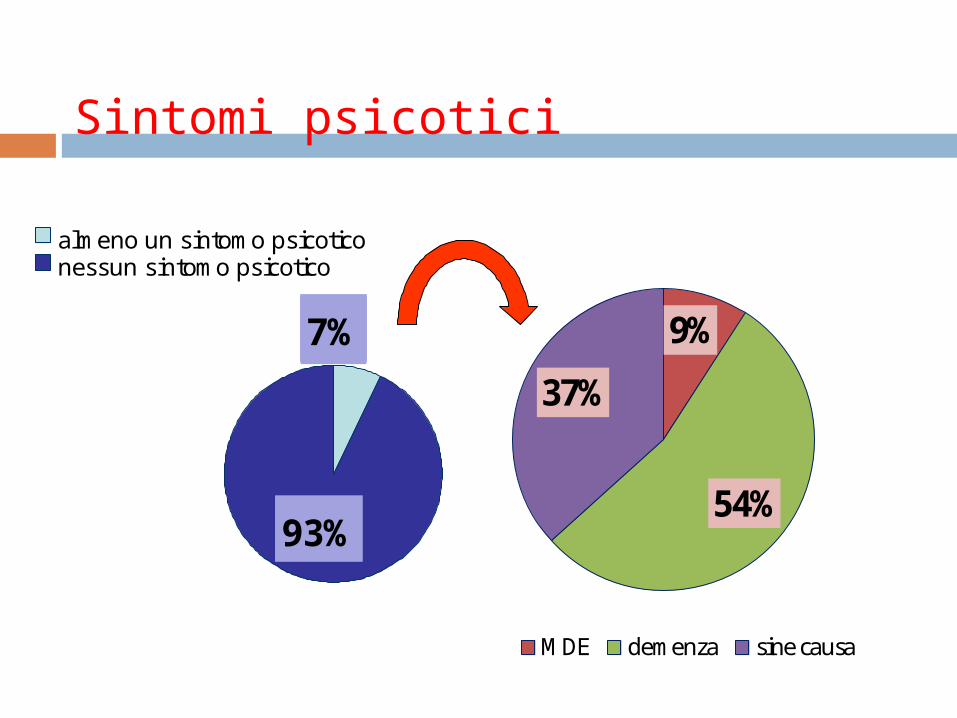
Sintomi psicotici
9%
54%
37%
MDE demenza sine causa
0%0%7%
93%
almeno un sintomo psicoticonessun sintomo psicotico
