· front cover image: angiogram taken ... teaches a popular course for the acr and hosts our...
TRANSCRIPT
2006 - 2010 DEPARTMENT OF RADIOLOGY

Front cover image: angiogram taken during coil embolization of a posterior communicatingartery aneurysm at DHMC by interventional neuroradiologist Clifford Eskey. Advanced capabilitiesof current-generation imaging technology, such as the Siemens biplane angiography system on which this image was captured, have fueled rapid growth in precise minimally-invasive neurointerventional procedures. (The patient in this instance arrived at DHMC in a coma as aresult of an acute subarachnoid hemorrhage. Following the embolization procedure depictedhere, he made a complete recovery.)

1
TABLE OF CONTENTS
Chair’s Overview
Education Programs
Residency
Medical Students
Clinical Divisions
Body Cross-Sectional Imaging
Gastrointestinal Radiology
Ultrasound Imaging
Neuroradiology
Musculoskeletal Radiology
Breast Imaging
Cardiothoracic Radiology
Vascular and Interventional
Nuclear Imaging
Pediatric Radiology
Uroradiology
VA Hospital
Diagnostic Physics
Clinical Programs Outreach
Radiologic Technologists
Nurses in Radiology
Information Systems
Imaging Systems
Medical Imaging Research
Diagnostic Radiology Faculty
Faculty Publications
100 years of Dartmouth Radiology
Facilities Map
3
8
12
14
16
17
18
20
21
22
24
26
28
29
30
31
32
34
36
37
38
40
46
48
54
56
Department of RadiologyDartmouth-Hitchcock Medical CenterOne Medical Center DriveLebanon, NH 03756(603) 650-4488www.dhmc.org/goto/radiology
This report was produced by the Department of
Radiology with contributions from numerous faculty
and administrative staff members, and with the
support of the Department of Public Affairs and
Marketing. Overall design based on a template
developed for DHMC department reports by
Mary di Paola and the Department of Public
Affairs and Marketing. Photograpy by DHMC
Staff Photographer Mark Washburn, with additional
images provided by Daniel Deneen and Jeff Nintzel.
Manuscript layout and print preparation by Robert
Hagen of The Hagen Group. Project management,
editing, original text contributions, and cover design
by Daniel Deneen. Special thanks to Mat Doyle at
Heron Graphic Arts, Erin Higgins, Katherine Beinder,
Bob Manwaring at SPC, Jessica Rider, Leah Christiano,
and Marie O'Quinn.

With gratitude and fondness, we dedicate this report to our friend, facilities manager Paul Roy, retiring this spring after 26 years of commitment to the mission and the people of this department.
The Department of Radiology, in concert with the entire medical, academic and research staff of Dartmouth-Hitchcock Health,seeks to lead the transformation of health care in our region, settingthe standard for our nation in achieving the healthiest population possible. Through research, education, clinical practice and community partnerships, we are committed to the mission of advancing health, providing each person the best care, in the right place, at the right time, every time.

I take this occasion to offer an overview of the department, toreflect on the challenges and achievements of the four yearssince our last report, and to highlight ongoing initiatives andpriorities for the future. These years have included difficultperiods in which economic turmoil and rancorous debate onhealthcare policy have tested our communities in many ways.So it is with great pleasure and gratitude I can report that thededication and commitment to excellence which characterizesthe entire Radiology staff remains intact. Across the spectrumof our endeavors—in the quality of our teaching and clinicalcare, our imaging capabilities, our leadership roles, and theimpact of our research and scholarly work—we have achievedthe results that reaffirm our standing among the nation’s finestradiology services.
We have made several outstanding additions to our physicianstaff. Dr. Elizabeth Dann, a former resident and DHMC fellow,has already made significant contributions and now leads ourBreast MRI service. Dr. David Pastel, a superb addition to ourgrowing neuroradiology staff, was also with us as a resident andfellow. The neuroradiology staff is further enhanced with the2009 arrival of Dr. Clifford Belden, from Albany MedicalCollege, who brings more than ten years’ experience in clinicalneuroradiology, fMRI, and a strong track record in research.(Drs. Belden and Pastel almost immediately made us proud,sweeping top honors at the 2009 American Society ofNeuroradiology Annual Meeting with a pair of scientific
exhibits on hypopharynx imaging.) Dr. Julianna Czum joinedus in 2006 as a specialist in non-invasive cardiac and vascularimaging and now directs cardiothoracic imaging. We have hadthe pleasure of welcoming longtime VA Hospital colleague Dr. Nancy McNulty to the full-time staff. Along with providing imaging expertise in several modalities and clinicaldivisions, Dr. McNulty plays an active and innovative role inthe Medical Student Education program. Finally, we await the arrival this August of Dr. Albert Song, who will join the musculoskeletal division, bringing a much appreciated expertise in tumor imaging. We look forward to the contributions our new colleagues will bring in patient care,scholarship and teaching.
The faculty continues to play leadership roles within and beyond the institution—of which I note here but a few examples. Dr. Jocelyn Chertoff, department Vice Chair andformer director of the residency program, serves as AssistantDean for Clinical Affairs, chairs the Hitchcock Foundation, is active in various other institutional capacities, and fills key leadership positions at several of the country’s most influential radiology and medical education organizations. Dr. Clifford Eskey serves on the institution’s InpatientCoverage and Care Committee, is President of the EasternNeuroradiological Society, and serves on the Editorial Boardof the American Journal of Neuroradiology. Dr. John Gemeryrepresents the department on the Ongoing ProfessionalPerformance Evaluation (OPPE) Committee. Dr. Alan Siegelis an active proponent for the uses of new communicationstechnologies in medicine; he serves on the InformationSystems Steering Committee and the Clinical InformaticsGroup. Dr. Marc Seltzer, a nationally-recognized expert onPET-CT, teaches a popular course for the ACR and hosts ourannual PET-CT conference. Dr. Clifford Belden sits on theCommittee for the Protection of Human Subjects, and hastaken over for Dr. Robert Harris as director of the RadiologyResearch Committee. Dr. Harris, who recently completed theMPH program at TDI, has developed a program for introducingportable ultrasound equipment and training to obstetric clinicsin remote settings in under-developed regions around theworld. Dr. Petra Lewis plays a major role in national medicalstudent education; she and Dr. Nancy McNulty have authored various online education resources widely used both withinand outside this institution.
Among recent D-H management changes, I note in particularthe departure of Clinical Services VP, Ron Sliwinski, whosewisdom and ingenuity have helped build and guide the
CHAIRMAN’S OVERVIEW
3DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
Peter K. Spiegel, MDDepartment of Radiology Chair

4
department for the past twenty years. We welcome MaryOseid, who brings a record of institutional accomplishment andextensive systems knowledge to her new appointment as VP ofAmbulatory Care; and with equal enthusiasm welcome Dr. JamesWeinstein—skilled orthopedic surgeon, TDI director, and medical outcomes advocate—to his new role as Dartmouth-Hitchcock Clinic president.
Department veteran Jim Roberts—more than once tapped totake on key roles when needed—accepted the position ofAdministrative Director in mid-2008. His organizational andcommunication skills are already much in evidence, and withover 30 years as an imaging technologist and manager at DHMC,he brings insights and experience that will benefit the department
in years to come. The position of Clinical Operations Manager,previously filled by Jim, is now held by the team of ChrissKvinlaug (for CT, VIR, nuclear imaging, and MRI ) and KarenBurgess (for DX, mammo, and ultrasound). Chriss, taking onthis role just as we go to press, has been a highly effectivedirector of the radiologic nursing staff for many years, and wehave strong expectations that she will provide excellent leadershipin this new role as well. Karen, very ably serving in her presentcapacity since 2008, began her radiology career with us as anRT over 20 years ago, returning now after a successful interludein regional mammography research and clinical practice. A finalnote on administration changes includes a farewell to FacilitiesManager, Paul Roy. In his 26 years of service, Paul played a keyrole in building the department and sustaining our technologi-cal edge—his skill and dedication will be missed and longremembered.
Clinical Programs In FY 2009 the department completednearly 246,000 exams and procedures, representing a 31%increase in the four years since FY 2005—a 7% annualizedgrowth rate. This volume growth has occurred in all majorimaging modalities. Our teams in the DX core performed30,000 more exams and procedures in 2009 than in 2005. MRIand ultrasound saw strong growth on a percentage basis, of 35%and 42%, respectively. The more regular use of obstetric screeningexplains part of the growth in ultrasound, but volume growth inall diagnostic modalities generally has been strong. The increasein the number (and variety) of image-guided interventionalprocedures has been even more dramatic. While the VIR team,with its comprehensive array of interventional procedures,accounts for much of angiography’s 45% volume growth, therehas also been an expansion in the number and complexity ofimage-guided procedures done outside the angiography suite—fluoroscopic PICC guidance, MR-guided procedures, and,especially, interventional CT.
Current generation CT systems permit highly accurate instrumentplacement for an expanding range of percutaneous interventionswhen highly detailed structural imaging is essential. In FY 2009,we performed over seven hundred CT-guided procedures, anincrease of 88% in the past four years. The growth of CT-IR is expected to continue, driven by strong demand, increasedversatility, and a superb new wide-bore scanner ideal for interventional cases. The neuroradiology interventional servicebegun in 2005 now offers the full range of endovascular treatments for cerebrovascular diseases; the biplane angiographysuite opened in 2009 is expected to spur expansion in both thenumber and variety of procedures. In early 2010, followinginstallation of a powerful new 3T magnet, Dr. Belden openednorthern New England’s first clinical fMRI service, providingclinicians with precise pre-surgical localization of brain struc-tures. We anticipate continued growth in neuroradiology, withinitiatives that include a new stroke service, additional neuro-IRprocedures, and the possible establishment of a neuroradiologycenter of excellence.
James E. Roberts, Administrative Director
Modality
ANGIO
CT
DX
MAMMO
MRI
NUC MED
ULTRASOUND
FY 2005
4,025
30,998
98,163
16,108
15,858
8,040
13,930
187,122
FY 2009
5,856
39,835
128,518
20,365
21,456
10,061
19,853
245,935
% ∆
45.5
28.5
30.9
26.4
35.3
25.1
42.5
31.4

Our Musculoskeletal division continues to experience growingdemand. Equipment upgrades and purchases (such as the innovative 1.5T small-bore MR “extremity” magnet installedlast year) and hiring new staff, such as Dr. Song, are part of anongoing expansion which includes the possible creation of amulti-discipline MSK Center.
Several other services introduced in recent years have become well-established. Breast MRI has grown in response to increasing awareness of the modality’s utility for high-risk andpre-operative patients. Dr. Czum, one of only several New England physicians certified in cardiovascular CT, heads up ourcardiac CT program. While volume growth has lagged expectations, the service has become a key element in theinstitution’s multi-disciplinary cardiovascular program. Drs.Michael Tsapakos and Nancy McNulty now offer CT (“virtual”)colonoscopy for failed colonoscopies, providing an importantservice even as wider use of CT colonography for screeningpurposes remains on hold pending regulatory agency review.
The contributions of our nurses and radiologic technologists remain central to the success of our clinical programs and thedepartment’s overall mission. In all modalities, the RT staffexcels not only in meeting the technical and patient-caredemands of their clinical role, but in the many ancillary wayswhich illustrate their dedication and resilience—as teachers andmentors, as innovators, as originators of quality and safetyimprovements. I note with gratitude the legacy of dedicationand innovation left by former DX Core team leader GeraldBergen, retired recently after 30 years of service.
Imaging and Information Systems Radiology relies upon the availability of increasingly complex and powerful imaging systems—and the rapid pace of technical innovation in thisfield presents both opportunities and challenges. Highlights of recent imaging acquisitions include: two new 1.5T MRscanners; the extremity MRI scanner noted earlier; a state-of-the-art interventional angiography suite featuring a new flatpanel biplane system; upgraded mammography units includinga stereotactic prone biopsy system; a cutting-edge Hologicbreast tomosynthesis unit; a SPECT-CT system to bolsteralready strong capabilities in nuclear imaging; a wide-bore“adaptive” CT scanner with fluoroscopy that delivers instantmulti-planar reformatting; and finally, a new 3T MRI systemthat enhances our MR capabilities generally, but especially infacilitating services in neuroradiology such as a clinical fMRI.
Maintaining the quality and competitiveness of our capacities in traditional diagnostic X-Ray systems—where roughly
half of our volumes are still generated—remains a priority. We have upgraded equipment in our rapidly-growing bonedensitometry (DXA) suite; installed upgraded X-ray units andtouch-screen workstations in the DX core and the ED;expanded capabilities in mammography with a specialized suitefor supine MR breast interventions; and we were among thefirst institutions to test and use portable X-ray wireless units.
Current generation radiographic, MR, and nuclear imaging systems can quickly generate studies containing thousands of images that form the basis for complex, customized reconstructions of almost endless variety. John Sundnas,RIS/PACS Administrator, continues to guide us in new information-systems acquisitions and to ensure the reliability of the data systems needed to support the work of our staff.Recent initiatives include: extending our RIS and PACS to theHitchcock Clinic facilities in southern New Hampshire and theimplementation of an effective interim solution for managingpatient studies from outside institutions conveyed on disc, even aswe continue development of a more ideal system of direct hospitalto hospital digital transfer.
Outcomes and Quality Assurance The department has a twenty-year record of support for outcomes-based medicine, andin recent years has been proactive in implementing the newstandards of quality management. The Radiology OutcomesGroup is responsible for promoting outcomes-based QI initia-tives, and draws on the ideas and resources of The DartmouthInstitute (TDI), one of the nation’s leading centers for compara-tive effectiveness research. The group includes TDI pioneer Dr.William Black and five other faculty graduates of the institute’sMS or MPH programs.
5DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
6
A noteworthy safety initiative undertaken last year concernedthe problem of “unexpected findings”—indications of seriouspathology unrelated to an exam’s primary condition of interest.The standard practice had been to note the finding in the radiologist’s report communicated to the attending physicianvia CIS—leaving open the possibility of the note being overlooked. With support from the institution’s RiskManagement Department, we designed and implemented an improved process that ensures follow-up, and established the position of Results Reporting Coordinator to ensure compliance.
Radiology Education The success of our residency programowes much to the expertise and dedication of Dr. JocelynChertoff, who steps down this summer after 17 years as Residency Director. During the years of Dr. Chertoff ’s leadership,the program doubled in size, kept pace with frequent changesin ACGME requirements, and saw steady improvements in all aspects of resident education. Most recently, Dr. Chertoff spearheaded the expansion of the resident complement to 20,
and guided us to a third consecutive unconditional five-yearACGME accreditation. Dr. Anne Silas, our new ResidencyDirector, is a multi-talented physician with expertise in cardiacCT, VIR and uroradiology, and four years’ experience asAssociate Director. Willo Sullivan, recruited two years ago asProgram Coordinator has significantly enhanced the efficiencyand value of candidate visits, for students and faculty alike. Formy part, meeting candidates—with their remarkably diverseacademic, regional and cultural backgrounds—remains a greatpleasure, and provides me a chance to speak on some of myfavorite themes—our rich institutional history, the strengths ofour program, and the attractions of life in the Upper Valley.
Our fellowship programs—cross-sectional, MRI, neuroradiology,and VIR—continue to attract highly qualified candidates.Many of our residents end up staying on as fellows—testimonyto both the quality of the residency and the appeal of our fellowships.
The Medical Student Education program, directed by Dr. Lewis, actively involves much of our faculty and remains one ofour key priorities. Roughly 10% of DMS students have beenchoosing radiology residencies—a measure of the program’ssuccess. Spanning all four years, the program features a solidgrounding in the basics of radiology and a final-year electivewhich is among the most heavily subscribed electives at DMS.Drs. Lewis and McNulty have been energetic proponents forinnovative approaches to the curriculum, and have designed avariety of online resources widely used within the institutionand at radiology education programs across the country.
Medical Imaging Research Imaging research, a central element in our mission, includes clinical trials and studies led by staffradiologists, basic-science investigations in advanced imagingtechniques, and a number of major collaborative programs.Members of the clinical staff conduct clinical studies on aspectsof imaging techniques and outcomes. The interventional radiology division is particularly active—Drs. Hoffer, Silas,Forauer, Gemery and McNulty have in recent years publishedon a variety of IR topics, including subcutaneous access, CTsummation in RFA, endovascular stent-grafts, liver biopsy, andarterial closure. Dr. Lewis received considerable attention forher AJR-published study on MRI in breast-cancer screening.Dr. Cheung has published a series of recent pieces on MRI for detecting ligament injury in ankle fractures; she is recognized as an authority of tendon-injury imaging and has been repeatedly invited to present courses and lecturesat RSNA Annual Meetings and elsewhere. Drs. Eskey, Merlis, and Belden, with other colleagues from the

neuroradiology division, have published on aspects of MRimaging of the brain, optic nerve, and the spine. Dr. Chertoffhas recently published on abdominal imaging, in addition tovarious articles on issues in medical education. Members of the Radiology staff are centrally involved in several of the institution’s most significant clinical trials and research programs:Dr. Poplack directs the clinical component of the alternativebreast imaging program; Dr. Black is among the architects of the National Lung Cancer Screening Trial (NLST) and is PI for a new NIH-funded program on advanced cancerimaging outcomes.
Recent developments at the department’s ElectronParamagnetic Resonance (EPR) Center have dramaticallyunderscored Dartmouth’s prominent role in this field. EPRCenter founder and director Dr. Harold Swartz now leads aconsortium of four institutions seeking to develop EPR-basedportable dosimetry devices that can be used for medical triagein the event of catastrophic radiation exposure events. To befunded by an NIH “U19” grant expected to total nearly $16.6million over the next five years, this Dartmouth-led group willcompromise one of NIAID’s “Centers for MedicalCountermeasures against Radiation” (CMCR). Significant
additional funding for the development of an EPR tooth-dosimetry device is also expected later this year.
The Nuclear Magnetic Resonance (NMR) Lab conducts studies on hemodynamics, brain oxygenation andfunctional MRI—research which will be enhanced with theinstallation of a new 9.4T small-bore magnet in late 2010.NMR Director Dr. Risto Kauppinen is joined this year by Dr.Barjor Gimi—a gifted scientist with a background in physics,electrical engineering, bioengineering, and radiology—whobrings extensive experience in molecular magnetic resonance microimaging and is known for groundbreakingwork in encapsulation nanotechnology.
Cross-discipline collaboration is a central feature of the extended Dartmouth research community—and is decidedlythe case in imaging research, which includes a number of jointinvestigations involving faculty and staff from our department,other DMS disciplines, the Norris Cotton Cancer Center, andthe Thayer School of Engineering. The ten-year, NIH-fundedAlternative Breast Cancer Imaging (ABCI) program is ourlargest and longest-running research project. Led by Dr. KeithPaulson, Professor of Engineering and of Radiology, with thecontinuous support of Dr. Steven Poplack and faculty colleaguesin the Breast Imaging Division , ABCI is one of the mostextensive studies of its kind anywhere, and a prime example of Dartmouth’s success in generating solid results through collaborative research. Despite the difficult economy, the pastyear has brought over $10 million of NIH awards for multi-disciplinary medical imaging programs that include renewalfunding for the ABCI and related projects; a new RO1 grantfor digital breast tomosynthesis studies; and a $4 million “GO”grant for a cancer-imaging outcomes study led by Dr. Blackand Dr. Anna Tosteson that may include the establishment of aDHMC-based comparative effectiveness research center.
It is now 114 years since Hanover physician Gilman Frost teamed up with two Dartmouth physicists—his brother, EdwinFrost, and Frank Austin—to perform the nation’s first clinicalX-ray, producing an image of 14-year-old Eddie McCarthy’sfractured wrist. From that time to the present, Dartmouth-Hitchcock has maintained its place as one of America’s premierimaging centers, providing direct patient care and diagnosticsupport to all clinical areas of the hospital while training newgenerations of radiologists, and supporting a range of researchactivities designed to improve the utility of modern medicalimaging. It has been a privilege to be custodian of this richtradition, and to have served as facilitator for a faculty and staffwhich will most assuredly be among tomorrow’s leaders inradiologic services, patient care, and medical innovation.
7DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
fMRI brain images from the Philips 3T magnet in the Advanced Imaging Center,reconstructed on SPM software.

RESIDENCY TRAINING PROGRAM
8
Anne M. Silas, MDProgram Director
STAFF
Jocelyn D. Chertoff, MD, MSAssociate Director
Petra J. Lewis, MDAssistant Director
Anthony L. Merlis, MDAssistant Director
The DHMC Radiology Residency program trains residents to the higheststandards of competency across the spectrum of imaging modalities and procedures. Prepared for independentexercise of medical judgment and initiative, our residents continue to beselected for highly competitive subspecialtyfellowships. In 2009, we added four positions, expanding the program to 20residents. The larger complement createsflexibility in meeting the clinical trainingneeds of our residents, greater opportunityfor resident research, helps meet thedemands of new ACGME call requirements,takes advantage of a strengthened facultyand state-of-the-art imaging equipment,and will contribute to improved clinicalcare. In April 2010 the program wasawarded ACGME’s strongest possibleendorsement—unconditional five-yearaccreditation. We strive to make the resident recruitment process, especially thevisits of residency candidates, as informativeand congenial as possible. We begin theinterview season early, and emphasize ahighly individualized experience: eachapplicant meets with radiology attendingsone-on-one, for up to a half-hour, and allcandidates meet with the RadiologyDepartment chair.
Residency directors and the faculty subject the curriculum to an ongoingassessment that includes close attention to new ideas in radiology education, areadiness to implement innovative changes,and responsiveness to feedback from ourresident staff. The core curriculum followsAmerican Board of Radiology (ABR)guidelines: modality-based sections andtwo-year series of conferences, with standardized annual evaluations. TheABR’s proposed change on oral boardspromises a more clinically-focused fourthyear and an exciting opportunity for initiatives throughout the program; anticipated changes include a more intensiveresearch elective and increased collaboration
with Dartmouth College. Our ManagedCare Curriculum—designed to address outcomes research, evaluative sciences,ethics, and management—has been adoptedas a model for the radiology curriculumbeing developed by the Association ofProgram Directors in Radiology (APDR)and the American College of Radiology(ACR). One of the best of the web-basedradiology learning portfolio systems is theACGME Learning Portfolio (ALP)—forwhich we participated as one of a handfulof alpha test sites.
The radiology residency stresses hands-on experience, view-box teaching, and joint teaching conferences with facultyfrom Urology, General Surgery,Gastroenterology, Pulmonary Medicine,Thoracic Surgery, ENT, Maternal/FetalMedicine, Neurology, Neurosurgery, andPediatrics. We are privileged to be amonga select group of institutions that offer residents a comprehensive course in radiological physics. Off-campus rotationsinclude the VA Hospital in White RiverJunction, VT, providing an excellent opportunity for integrated patient care andgraduated responsibility; Boston Children’sHospital—a core experience in pediatricradiology that supplements the month ofpediatric rotation at DHMC and theChildren’s Hospital at Dartmouth (CHaD);and a month at the Armed Forces Institute
Jocelyn D. Chertoff, MD, MSProgram Director, 1993-2010

of Pathology in Washington, DC, for agrounding in radiologic-pathologic correlations—a key step in building theconceptual framework for transformingoceans of data into the integrated knowledge needed in medical practice.The program also includes an unusuallyprominent role for residents in medical student education. Recent changes affecting the quality of resident lifeinclude a reduction of holiday call responsibilities to a maximum of 12hours, and a noon-time start for daysresidents are scheduled for call. Anactive program for guest lecturers bringsdiverse ideas and exposure to medicalleaders from around the nation and theworld. Residents present grand roundsin a program of formal lectures that alsoincludes presentations by fellows and faculty. Monthly Journal Club meetingsprovide an informal setting for discussionand critical evaluation of timely issuesand peer-reviewed journal articles. The University of Vermont has a tradition of highly effective Mock BoardExaminations, to which our residents areregular invited participants.
Many of the radiology teaching staff are closely connected, as graduates and faculty, to the Dartmouth Institutefor Health Policy and Clinical Practice(TDI), bringing to residency instructionthe insights of one of the nation’s leading institutions for research method-ologies and evidence-based medicine.Our residents are encouraged to pursueTDI training through the LeadershipPreventive Medicine Residency, a two-yearprogram leading to the MPH degreeand board-eligibility in PreventiveMedicine and Radiology.
The incorporation of innovative, computer- and web-based learningresources is a key component of ourprogram. The Radiology LearningLaboratory includes the ACR’s teachingfile, with thousands of referenced, annotated cases on film, CD-ROM and laser disc format, and audiovisual
seminars in general radiology and emergency radiology. We have developedcomputer-based tutorials for residentsand medical students. To validate andimprove our teaching, we participate in the ACR In-Training Examination,which permits comparison with examresults from residents in programsthroughout the country. To ensure thatresidents are ready for independent examinterpretations and taking call, we relyon a variety of rigorous assessments thatinclude competency checklists and theRadiology Resident Pre-Call Evaluationexam. Developed by Dr. Lewis, the pre-call exam asks students to providepreliminary reads on up to 55 differentcases in a PACS-like environment characteristic of what can be expectedon call; the exam has been used here for the past three years, and is now available online to other institutionsvia MedEdPORTAL.
Residents contribute to the research activities of the department, independentlyor in collaborations which may includepartnerships with the department’s regular faculty or dedicated researchstaff. Attendance at national meetings is
encouraged, and meaningful scholarlyactivities—abstracts, conference presentations, journal articles—areexpected of residents, as well as participation in the design and implementation of quality improvementinitiatives. A partial list of resident-authored studies published in peer-reviewed journals is included in theappendix.
Residents are encouraged to attend thescientific sessions of the New EnglandRoentgen Ray Society and the NHRadiological Society. Our chief residentsattend the annual meeting of theAssociation of University Radiologists(AUR). Residents are nominated forthe highly competitive Introduction toAcademic Radiology program presented atthe RSNA Scientific Assembly and theARRS Scientific Meeting, and also forthe Siemens-AUR Radiology ResidentAcademic Development (SARRAD) program. The department participates inthe Roentgen Research Award program;recent resident alumni award winnersinclude Scott Napinsky (2006), RihanKhan (2007), Jeremy Hopkins (2008)and Kiley Perrich (2009).
9DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
10
Program Administration
From 1993 to July 2010, the residency program was directed by Dr. Chertoff,department Vice-Chair and Director ofGastrointestinal Radiology. She plays anactive management and policy-makingrole at DHMC and DMS, and is currentChair of the Hitchcock Foundation. Dr. Chertoff is Co-Vice Chair of the Commission on Education at theAmerican College of Radiology, and is directing development of the gastrointestinal portion of the core ABRexam; she holds key positions in medicaleducation organizations including theAlliance of Clinician-Educators inRadiology, the AUR, the Association of Program Directors in Radiology
(APDR), and the Accreditation Councilfor Graduate Medical Education(ACGME).
Dr. Silas, who assumes the role ofResidency Program Director in July2010, will be assisted by Dr. Chertoff,who continues active participation in theprogram as Associate Program Director,and by Assistant Directors, Drs. Merlis and Lewis, all of whom pursue medicaleducation interests within the institutionand in national organizations. Dr. Silas, an active member of the APDR and the AUR, had been responsible for therotation and call schedule, and for programmanagement in the Director’s absence.
Dr. Lewis, who also serves the departmentas Director of Medical Student Education,serves in a variety of leadership capacitiesat various professional organizations,including a recent term as President ofthe Alliance of Medical Student Educatorsin Radiology (AMSER.) Dr. Lewis has been an energetic advocate for incorporating informatics technologiesinto the curriculum, and has developed a number of innovative online tools forresident education, including theRadiology Resident Pre-Call Evaluationexam mentioned above.
Recent Alumni: Post-Residency
E. Patrick Farley 2010 Neuroradiology Fellowship, University of North Carolina, Chapel Hill
Jonathan Kullnat 2010 Neuroradiology Fellowship, Oregon Health and Science University
Alexei Viazmenski 2010 MRI Fellowship, DHMCStephen J. Guerin 2010 Neuroradiology Fellowship, DHMC
Jennifer Krawitt 2009 Body MRI Fellowship, DHMCSteven Krohmer 2009 VIR Fellowship, Johns Hopkins School of MedicineKiley Perrich 2009 MSK Fellowship, University of Washington, SeattleDagmar Savellano 2009 Instructor in Radiology, DHMCScott Smith 2009 Neuroradiology Fellowship, DHMC
Michael Beckerman 2008 MRI Fellowship, DHMCDianne Brann 2008 Private practice, Lexington, KYTien Burns 2008 Body Imaging Fellowship, Fletcher Allen Health,
Burlington VTAssistant Professor of Radiology, DHMC/VA Hospital
Paul Farris 2008 Cross-Sectional Fellowship, DHMCSeattle Radiologists, Seattle WA
Jeremy Hopkin 2008 Neuroradiology Fellowship, Barrow Neurological Institute, Phoenix
David Pastel 2008 Neuroradiology Fellowship, DHMCAssistant Professor of Radiology, DHMC
Lesly Benodin 2007 Private practice, Meriden Health, NJElizabeth Dann 2007 Women’s Imaging Fellowship, DHMC
Assistant Professor of Radiology, DHMCRihan Khan 2007 Neuroradiology Fellowship, Barrow Neurological
Institute, Phoenix Michael Meszaros 2007 Neuroradiology Fellowship, DHMC
Marc Mancuso 2006 Childrens Hospital, Boston MAScott Naspinsky 2006 Diagnostic Imaging Flight, Elmendorf AFB AKElena Wechsler 2006 Mass General Hospital, Boston MA
Shervin Dean 2005 MRI Fellowship, DHMCTatum S. Johnson 2005 Pediatric Radiology Fellowship, MallinckrodtTimothy Mahoney 2005 VIR Fellowship, DHMCDavid Siepmann 2005 University of Wisconsin, Madison WI
11DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
MEDICAL STUDENT EDUCATION
12
Petra J. Lewis, MDProgram Director and Year 3-4
Coordinator
Nancy J. McNulty, MDYear 1-2 Coordinator
Our faculty plays a major role in theDartmouth Medical School curriculum,with multi-year courses intended toadvance several overlapping goals: theeffective use of medical imaging resourcesas learning tools in the clinical curriculum;a thorough introduction to the purposesand methods of modern radiology; and,for interested students, a clinical electivesprogram designed to provide an in-depthunderstanding of the appropriate uses of medical imaging and interventionalprocedures, exam methodologies, thebasics of image interpretation, and cost-effective image management.
Some measure of the program’s ongoing success can be found in a number ofquantifiable achievements. Basic ClinicalRadiology, our fully-subscribed fourth-yearelective, is one of the most popular DMSelectives, chosen by roughly 60% of allstudents. The number of our studentselecting radiology residencies remainslarge—averaging over 9% in the pastdecade, significantly above the comparable
6% national rate—and shows little sign ofabating, as witnessed by the 14% of theDMS class of 2009 who chose residenciesin radiology. And finally, we cannot helpbut take pride in the fact that for each ofthe past eleven years, our students seekingradiology residencies have succeeded in a100% match rate.
First and Second Year Courses
The first-year anatomy curriculumincludes Dr. McNulty’s classes on anatom-ical-radiological correlation, and routinelyutilizes the lessons and image-database of the radiology component (designed byDr. McNulty) of the DMS HumanAnatomy website. The second year’sScientific Basis of Medicine program includesa nine-hour introduction to medicalimaging and the pathophysiological basisof imaging abnormalities. Additional radiology opportunities for first and second-year students include the eight-week informal Spring Elective inRadiology and regular Radiology InterestGroup meetings.
The DMS Human Anatomy website receives roughly 100,000 hits/month.

13DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
Clinical Electives The centerpiece ofour program is Basic Clinical Radiology, afour-week elective offered in any of fourblocks during the fourth year, and in afifth block available to third-year students.Designed for both future radiology residents and for students aiming atother specialties, the elective includesexposure to all areas of diagnostic andinterventional radiology. Radiology residents take an active role as instructorsin the program—an involvement whichwe believe enriches the educationalvalue of the elective for residents andstudents alike. Specifically, the electivecovers the advantages and limitations ofthe key imaging modalities; the clinicalbasis for appropriate imaging requests;how images are obtained and proceduresare performed with the goal of understanding patient selection and suitability; how to provide informedadvice to patients; how imaging is incorporated into logical medical problem solving; and the basics of radiological interpretation as applied to routine and emergency medical practice. The elective includes individually-tailored clinical rotationsthrough the subspecialty areas, as well as student presentations and work-shops. Students are expected to spend anevening on call with one of the residents,and to take advantage of the department’sextensive electronic and web-basedresources during the scheduled blocksreserved for self-teaching. Image management workshops, and livelyinteractive sessions including “imagejeopardy” and an “imaging lingo” conference form an additional part of a curriculum designed to emphasize multiple teaching methods. For theduration of the elective, students arewelcomed to participate in all academicand social activities of the department.
In addition to this basic clinical elective,fourth-year students may choose fromseveral shadowing-type electives. These2 to 4 week courses are limited to oneor two students and include the highlypersonalized Flexi-Elective; subspecialtyelectives in neuroradiology, interventionalradiology and women’s imaging; and a research elective which forms the basis for short or long-term researchprojects which students are encouragedto undertake.
Education Leadership Drs. Lewis andMcNulty are advocates for the use ofelectronic and web-based technologies,with respect to both the application of radiologic resources to all areas ofmedical student education, and for medical imaging instruction specifically.Working together or individually, theyhave developed a number of onlineresources for medical student education:
• The Basic Clinical Elective utilizes a Blackboard™-based collection of web-based teaching files, scheduling applications, evaluation tools, and thefinal exam.
• Human Anatomy Learning Modulesis a popular (100,000 hits/month)web-based curriculum now incorporated into the DMS anatomycurriculum (and at U. Penn andU.S.C.) Dr. McNulty created andcontinues to develop the site’sradiologic component.(www.dartmouth.edu/~anatomy)
• Radiology ExamWeb, part of a nationalinitiative for standardized testing inradiology, was designed by Drs. Lewisand McNulty; funded by the RSNAand the Hudson Foundation, theproject now includes 22 institutionsnationwide.(http://radiology.examweb.com)
• CORE (Case-orientated RadiologyEducation) is a web-based radiologycurriculum for 3rd and 4th yearmedical students; developed byDr. Lewis, CORE is now usedthroughout the medical schoolcurriculum for case-based simulationsand problem-solving exercises withinthe surgery, pediatrics, medicine andneurology clinical clerkships.(http://core.instruct.de)
• The AMSER Shared Resourceswebsite, developed by Dr. Lewis andavailable to all AMSER members,includes a multi-institutional databaseof images which have been founduseful in teaching, and a separatedatabase of shared documentsincluding curricula, lectures, exams,games and other resources.(www.dartmouth.edu/~amserimages)
In addition, a web-based teaching file application under development by Dr. Siegel, with support from a DMSVenture Fund grant, will become a significant additional resource uponimplementation later this year. BothDrs. Lewis and McNulty are active withnational organizations dedicated to medical student and residency education.Dr. Lewis served as president of theAlliance of Medical Student Educatorsin Radiology (AMSER) in 2006-2007,and now chairs its ElectronicCommunications Committee. Dr. Lewisholds committee assignments at theAssociation of Program Directors inRadiology, at the American Board ofRadiology (various faculty and resident certificiation committees), and atUSMLE/NBME (the Anatomy andEmbryology Exam Committee). Dr. McNulty is similarly active in nationalmedical education organizations, andserves currently as President of AMSER.

BODY CROSS-SECTIONAL / CT AND MRI
14
Michael J. Tsapakos, MD, PhDDivision Co-Director
Director, Cross-sectional and
MRI Fellowships
Nancy J. McNulty, MDDivision Co-Director
The Body Cross-Sectional ImagingDivision provides CT and MRI studiesmainly concerned with the chest,abdomen and pelvis. The division overlaps with and complements varioussubspecialties (e.g., cardiothoracic, MSK,abdominal) that also rely on cross-sectionalimaging modalities. Most of the Radiologystaff have general expertise in cross-sectional imaging, and most spend at least some of their clinical time on bodycross-sectional rotation. The divisionworks closely with a variety of clinicaldepartments. We attend the weekly theGastrointestinal Tumor Board conference,and a GI-Radiology conference to review MRI and CT studies in a casepresentation format. The division alsoactively supports the numerous investigatorsat the Norris Cotton Cancer Center,including recent collaborations concerningpancreatic imaging and treatment.
Body CT Computed tomography plays a critical role in diagnosis and management in emergent, inpatient andoutpatient settings. Our facilities includefour CT systems: two 16-slice GELightspeed scanners; a 64-slice Lightspeedmultidetector CT system capable ofextensive diagnostic evaluations includingcardiac, vascular, and 3D studies; and aversatile wide-bore “adaptive scanner”installed last year—the Siemens SomatomDefinition AS. Featuring fluoroscopiccapabilities and instant multi-planar reformatting, the new Siemens system significantly facilitates CT-guided interventional procedures such as biopsies,drainages, and thermal ablation therapies.Interventional CT has been a rapidlygrowing component of our practice—698CT-guided interventions were performedlast year, a 150% increase over the 277done in 2004.
CT has benefited from Radiology’s PACS system, which displays digital CT,Ultrasound and MR Images, and linksthem to the electronic patient record.The impact of PACS continues to be
remarkable, allowing much quicker readingtimes and much quicker turnarounds ofinterpretations to referring clinicians.
Patient care and safety remains at the forefront of our mission. CT imaging is apowerful modality that has providedadvances in diagnostic accuracy. Usedappropriately, the medical benefits of CT far outweigh the risks associated with exposure to ionizing radiation.Monitoring patient dosages, minimizingexposure levels, and regular review of protocols are standard safeguards and constitute priorities in our practice. Foryounger patients, the need for caution isgreater still, and the department participatesin the nation-wide Image Gently campaigndesigned to find and share opportunitiesto reduce radiation exposure in children.
CT Colonscopy The division has established a CT colonoscopy (“virtualcolonscopy”) service used on a limitedbasis in cases of failed colonscopies.High-resolution thin-section CT seriescan be reformatted on 3D workstationsfor accurate, non-invasive “fly-through”examinations of the colon lumen forpolyp detection. Drs. Tsapakos andMcNulty have both received training inthe procedure. As of spring 2010, CTcolonscopy for screening purposes remainson hold, pending regulatory agencyapproval and the availability of insurancereimbursements.
Body MRI The safety, versatility, and rangeof unique imaging attributes of magneticresonance imaging continues to driveincreases in both the variety and volumeof studies performed. In addition to itsestablished role as an adjunct to CT, MRIis widely and increasingly used as a pri-mary imaging modality for pediatricpatients and for many soft-tissue imagingpurposes, such as hepatic, kidney, pancre-atic, prostate, and adrenal gland imaging.A number of the division’s MRI servicesthat have become key areas of interestinclude:

15DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
• MR enterography, used for evaluation of patients with inflammatory diseasesof the bowel (e.g., Crohn’s), producedetailed real-time imaging and permitsradiation-free imaging for patientswho will need ongoing monitoringover a period of many years;
• MR Cholangiopancreatography (MRCP) is a growing noninvasivecorollary to Endoscopic RetrogradeCholangiopancreatography (ERCP).
• pelvic imaging, for detecting pelvic neoplasms, uterine congenital anomalies, and other ovarian and cervical pathologies;
• fetal imaging, as an adjunct to fetal ultrasound for certain types of multi-planar views;
• magnetic resonance angiography (MRA).
The department operates two permanent1.5T magnets, a mobile 1.5T scanner,and as of March 2010, a new 3.0T magnet—the GE Discovery MR750 system. Fast and powerful, the MR750provides exquisitely detailed studies thatfacilitate a range of chest, abdomen,pelvic and MSK exams, including fMRIfor localizing prostate neoplasms in pre-surgical planning. (The 3T magnetalso offers important enhancements andnew capabilities in neuroimaging—mostnotably, fMRI.)
3D Imaging With ongoing advances in 3D post-processing, the plane ofimaging has become irrelevant. Imageseries obtained from high speed multidetector CT scanners are nowreconstructed as remarkably lifelike 3Dvolumes for angiographic imaging, cardiac imaging, excretory urographicimaging, and a range of endoluminalimaging purposes. Clinicians and, inparticular, surgeons have increasinglycome to rely on such studies to helpwith surgical planning.
Since 2008, 3D capabilities are available on workstations throughout the
department, including various service-specialized applications such as PrismClinical Imaging (for fMRI reconstruc-tions) and Vitrea (for virtualcolonoscopy).Visage CS, a web-based thin-client 3Dapplication, is available at all workstations.In addition, the Body Cross-SectionalDivision maintains a 3D lab for CTangiography reconstructions. Directedby Kayla Denny, RT, the lab uses GEAdvantage workstations to generatehighly sophisticated 3D volumes.
Education Programs Education continues as a priority for the division.Didactic CT and MRI instruction isincorporated across all radiology sectionsto help residents handle the myriad CTcases they will encounter over thecourse of their residency, in both medical and surgical subspecialties. Ourfellows and residents learn the intricaciesof clinical imaging parameters and activelyparticipate in reading MRI studies. Wehave incorporated cardiac imaging intoour residency and fellowship training asan adjunct effort with Cardiology.
Cross-Sectional Imaging Fellowship
The highly competitive Cross-SectionalImaging Fellowship, now in its 17thyear, includes training in neuroradiology,abdominal imaging, musculoskeletalMRI, and ultrasound. The fellowship is unusually flexible, with opportunitiesfor tailoring the program to meet the interests of individual fellows.Electives include cardiac imaging (withthe Department of Cardiology), mammography,musculoskeletal radiology,and CT-guided interventional procedures.
MRI Fellowship Initiated in 2005, the one-year MRI fellowship programemphasizes—to an unusual degree in comparison with other such programs—a comprehensive range ofMRI training that includes cardiac, neurologic, musculoskeletal, abdominal,pelvic, MR angiography and MR-guidedinterventional procedures. The MRI fel-lowship, like the Cross-Sectional,encourages individualizing the programto meet special interests and needs.
Kidneys and aorta with stent. CT images reconstructed on a GE isovoxel 3D workstation.

GASTROINTESTINAL RADIOLOGY
GI Radiology’s success depends on ourteamwork, and on close collaboration with the departments of Gastroenterology,General Surgery, and Internal Medicine.Weekly CME-accredited multidisciplinaryGI conferences, at which students mayparticipate, feature diagnostic and therapeutic issues in a case-based format,and selected clinical advances presented bysubspecialty experts. The performance ofimaging studies in a focused, expedient, andlogical progression is one positive out-come of this multidisciplinary conference.Local physicians from outside the institutionalso participate at the conferences, as dovisiting professors of gastroenterology, surgery and radiology.
Exams are performed in three fluoroscopysuites, on pulsed digital systems (PhilipsEasyDiagnost™ Eleva) providing rapid,efficient studies while minimizing radiation exposure. Digital fluoroscopywith image transfer to PACS improvesefficiency, communication, and cost effectiveness. Our concurrent use of real-time fluoroscopy, captured on DVD,lets us further decrease radiation exposure,as well as expediting review, documentation,teaching, and communication with referringphysicians. Our radiologic technicians arehighly regarded—Philips Medical rates theDiagnostic Core and its staff as a “luminarysite,” and several technologists hold “clinicalsuper user” recognition for above-averageknowledge and skill. The division is committed to safe, child-friendly care, andworks closely with the Children’s Hospitalat Dartmouth (CHaD). We actively participate in CHaD’s Pain-Free Program,and in the Image Gently campaign, an initiative by the Alliance for RadiationSafety in Pediatric Imaging that seeks toraise awareness of the opportunities tolower radiation dose in children’s imaging.Maintaining a reassuring environment is also a priority, and the section has
enthusiastically taken on the responsibilityof making the visits of our pediatricpatients as comfortable and pleasant aspossible.
We continue to implement the corecurriculum in GI Radiology. Presentationsby department faculty are supplementedby visiting professors, New EnglandRoentgen Ray meetings, and GrandRounds. One-on-one review of teachingfile cases remain a very useful and popularpart of the fluoroscopy rotation and Dr.Chertoff ’s experience as a GI examinerfor the American Board of Radiologyexamination enhances the review sessionsheld for the senior residents.
The delivery of high-quality care to patients with complex disorders requiresclose coordination of services provided byvarious departments; the New EnglandHepatobiliary Disease Center—a collabo-ration between DHMC gastroenterologists,surgeons, and radiologists—was developedto meet this need. The Center’s goalsinclude state-of-the-art diagnostic and therapeutic services, the promotion ofresearch on hepatobiliary diseases, andhepatobiliary disease education and datasharing.
Division director Dr. Chertoff plays an active leadership role at DHMC andDMS. She chairs the Board of Directorsof the Hitchcock Foundation; is Co-ViceChair of the Commission on Education at the American College of Radiology(and is directing development of the gastrointestinal portion of the core ABRexam); and holds key positions in medicaleducation organizations including theAlliance of Clinician-Educators inRadiology, the AUR, the Association ofProgram Directors in Radiology (APDR),and the Accreditation Council forGraduate Medical Education (ACGME).
16
Jocelyn D. Chertoff, MD, MSDivision Director
STAFF
Jocelyn D. Chertoff, MD, MSJudith Austin-Strohbehn, MDDagmar Hoegemann Savellano, MDSteven K. Sargent, MDMichael J. Tsapakos, MD, Ph.D

17DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
ULTRASOUND IMAGING
Steven K. Sargent, MDDirector for Clinical Operations
Robert D. Harris, MDDirector for Education and Research
STAFF
Jocelyn D. Chertoff, MD, MSElizabeth W. Dann, MDRoberta diFlorio, MD, MSRobert D. Harris, MD, MPHPetra J. Lewis, MDSteven S. Poplack, MDSteven K. Sargent, MDAnne M. Silas, MDTherese J. Vaccaro, MDStephanie P. Yen, MD
MFM/REI STAFF
E. Rebecca Pschirrer, MD Director of OB/GYN Ultrasound
Misty Blanchette Porter, MDDirector of REI Ultrasound
Emily R. Baker, MDMichele R. Lauria, MDMichelle Russell, MD
The goals of the Division of UltrasoundImaging are to provide effective, high-qualityimaging services to patients in the mostcompassionate and stress-free manner possible; to provide high quality educationalopportunities to students across a spectrumof professional backgrounds—radiologyfellows and residents, medical students, andsonography trainees; to advance knowledgein clinical care and the technologies ofultrasound imaging; and provide an effectiveand collegial referral service to cliniciansfrom throughout the Dartmouth-Hitchcockcommunity. We work closely with theChildren’s Hospital at Dartmouth (CHaD),and with the Department of Obstetricsand Gynecology. Utilization of ultrasoundimaging has been increasing steadily—ourclinical volumes have increased at an annualrate of roughly 9% over the past five years.
Ultrasound is used for imaging all body areas except the heart and vascular system,and also plays a role in image-guidedinterventional procedures, including theProstate Biopsy Clinic at NCCC. We workin close collaboration with the membersof the Maternal-Fetal Medicine (MFM)staff and Reproductive Endocrinology/Infertility (REI) specialists, who conduct acomplementary imaging service. Analsphincter sonography is used to diagnosedefects in the sphincter, which may lead tourinary or fecal incontinence followingchildbirth or trauma. Screening programsinclude nuchal scans for the early detectionof Down’s syndrome, liver and portal veinscreening for cirrhosis.
The division employs eight sonographers,and maintains an eight-room facilityequipped with Philips Medical and Siemensultrasound systems and, new this year, theGE Logic E8. 3D imaging is increasinglycommon, as well as the use of cine clipsthat can be captured and displayed onworkstations. Dennis Seguin, ultrasoundteam leader, has been invaluable in maintaining the quality of our service and systems.
Teaching and research are key componentsof our mission. Education occurs at thepatient bedside; in resident, fellow, andmedical student training programs; insonography apprenticeships; and in monthlyconferences on ultrasound and maternal-fetal medicine. At our monthly perinatalworking group, obstetricians, neonatologists,radiologists, and geneticists gather to discussinteresting and difficult cases. With respect to technologists’ education, we arecollaborating with Lebanon College on atraining program in sonography. Ongoingresearch interests and activities include:
• A pilot trial testing the validity of compact US for use in developing countries
• A multi-center retrospective analysis of the chorionic bump, a first trimesterultrasound finding first described atDHMC
• Participation in a multi-center study of US characteristics of thyroid nodules
• the use of ultrasound-guided core needle biopsy for diagnosis of bilateraltesticular sarcoidosis
Several staff members, including Dr. Harris, are graduates of the MS or MPHprograms at The Dartmouth Institute(TDI). Last spring, the division participatedas a clinical improvement test site in a TDIcourse on continuous quality improvement.Other recent QI initiatives include theimplementation of an OB/GYN automatedreporting system aimed at decreasing thelikelihood of recording errors.
NEURORADIOLOGY
18
Clifford J. Eskey, MD, PhDDivision Director
Neuroradiology Fellowship Director
STAFF
Clifford J. Belden, MDLaurence D. Cromwell, MDClifford J. Eskey, MD, PhDJohn J. McIntyre, MDNancy J. McNulty, MDAnthony L. Merlis, MDDavid A. Pastel, MD
The Neuroradiology Division is an integralpart of the Clinical Neurosciences Programat DHMC and of the extended medicalneuroscience community of New England,for which we provide consultation services.The division conducts imaging studies ofthe brain, spine, head and neck, and offersthe full spectrum of neurointerventionalprocedures. Advancing knowledge toimprove diagnosis and treatment of brainand spine disease is a crucial part of ourmission, and we are actively involved inresearch and in the training of residents,fellows, and medical students.
Drs. Cromwell and Merlis bring many years of expertise in all areas of neuroradi-ology; in addition to clinical duties, bothare active in many aspects of departmentaladministration, scheduling, and medicaleducation. Dr. McIntyre is Director ofSpine Radiology, and is a sought-after resident mentor and national speaker. Dr.Eskey, division head and director of theneuroradiology fellowship, is skilled in arange of interventional procedures; he
serves currently as president of the EasternNeuroradiological Society and as a memberof the Editorial Board of the AmericanJournal of Neuroradiology. With rapidlyrising volumes in all areas of neuroradiology,the department has in the past two yearsrecruited several highly talented new colleagues. Dr. Belden, joining us fromAlbany Medical Center, is a seasoned neuroradiologist with expertise in headand neck imaging and fMRI. We weredelighted to welcome Dr. Pastel to thefaculty following completion of his fellowship here in 2009. Dr. McNulty,previously practicing at both DHMC and the VA Hospital, is now with thedepartment full-time, splitting her clinicalresponsibilities with neuroradiology andthe VIR division.
Our technological capabilities have expanded with the acquisition of the flat-panel biplane angiography suite lastyear, and with new and upgraded MRscanners—including a powerful GE 3Tsystem, permitting Dr. Belden to initiate
fMRI images, such as these from our GE 3T magnet, reconstructed on PRISM software, permit precise location of brain structures linked to specific neural function.

19DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
fMRI clinical service this spring. WhileDHMC has been active in fMRI researchfor years, the new service represents thefirst availability in northern NewEngland of clinical fMRI. Capable ofmapping the motor, sensory and visualcortex, as well as certain language andmemory functions, fMRI scans can bereconstructed for highly lifelike, versatileimages which significantly enhance pre-surgical planning for a range of neurological procedures. Other areas of expanded capabilities in the divisioninclude diffusion tensor imaging and CTperfusion studies.
The interventional neuroradiology service,comprising both spine and endovascularprocedures, was introduced five years ago and has been growing steadily.Working closely with the sections ofNeurosurgery, Otolaryngology, and theDepartment of Neurology, we provideendovascular treatments that include themost effective advances in bioactivecoils, cerebrovascular access devices, liquidembolic materials, stents, and clotretrieval devices. The digital biplaneangiography suite is producing studies ofexcellent quality while reducing radiationexposures. The interventional servicerelies on the contributions of our associate providers, Sharene Evans,ARNP and Anne Michaels, PA, thenursing teams, and the highly skilledcadre of CT and MR technicians.
Education is a key part of our mission, and we are proud of our role and therecognition we have received—Dr.McIntyre, for example, was the 2008recipient of the Residents’ TeachingAward. Weekly didactic or case conferences for residents provide bothstructured learning and practice withboards-style cases. In addition to thedidactic conferences, we hold regular
clinical conferences with Neurology,Neurosurgery, Otolaryngology, andPediatrics. Weekly or monthly case conferences include generalNeuroradiology, Cerebrovascular Imaging and Treatment, Neuro-oncology,Endocrinology, Pediatric Neuroimaging,and Head and Neck Oncology. TheACGME-accredited neuroradiology fellowship, now in its seventh year, provides thorough training in CT and MR imaging and interventionalprocedures, including advanced endovascular brain techniques.
Neuroimaging research is performed by the core clinical faculty and by several dedicated basic scientists. Wecontinue our collaborations with the
Dartmouth Brain Imaging Laboratoryand the Advanced Imaging Center.Projects underway cover innovation inadvanced imaging at 3T in glioblastomarecurrence, MRI in pediatric head trauma, CTA in intracerebral hemorrhageand aneurysm evaluation, imaging ofpharyngeal carcinoma, vertebroplasty, andsynovial cyst rupture.

MUSCULOSKELETAL RADIOLOGY
20
Douglas W. Goodwin, MDDivision Director
STAFF
Yvonne Y. Cheung, MDDouglas W. Goodwin, MDJohn J. McIntyre, MDMarc A. Seltzer, MDAlbert J. Song, MD
The Musculoskeletal (MSK) Radiologystaff consists of full-time specialists, Drs. Cheung and Goodwin, and the support of a part-time staff consisting of neuroradiologist and spine-imagingspecialist Dr. McIntyre, and Dr. Seltzer ofthe nuclear imaging division. The divisionprovides image interpretation, consultation,and interventional services for patientswith disease or injury of the axial andappendicular musculoskeletal system, especially of the bones and joints.Modalities include X-ray, MRI, fluoroscopy,ultrasound, CT, and DXA. Interventionalprocedures are a growing component ofour practice, and include arthrographyservices, epidural steroid injections, andimage-guided biopsies of bone and softtissue. Bone densitometry (DXA) is performed by a staff of certified technolo-gists, and interpreted by Drs. Cheung,Goodwin, and Seltzer. Volumes haveincreased strongly in all areas of our service, driven in part by the growth inorthopedics and rheumatology referrals,particularly for hand surgery and myositisimaging requests. We utilize almost allimaging modalities of the department, but would highlight several new MRacquisitions: the ONI Systems 1.5T “MSKExtreme”—a magnet which combines thesimplicity of patient comfort of smallextremity imaging with the power of afull-sized system; and the GE Discovery™
3T system installed in March of this year.
The MSK staff is committed to the department’s educational mission. TheBasic Clinical Radiology elective for DMSstudents includes an MSK rotation; somestudents additionally take the specializedMSK elective. Residents join for amonth-long MSK rotation which, in addition to the MSK lecture series,includes reading experience in the full
range of MSK imaging; arthrography andbiopsy procedures; weekly orthopaedic andrheumatology conferences; and a monthlyosteoporosis conference. We are proud ofthe recognition the MSK staff has receivedfor teaching excellence, such as Dr.Goodwin’s2008 “Outstanding Teacher Award” fromthe Society of Magnetic Resonance inMedicine.
The MSK staff is active in imaging research.Dr. Cheung, who anticipates completingthe MS program at TDI this year, recentlycompleted (with former chief resident, Dr.Kiley Perrich) a comprehensive series ofankle-ligament studies which was publishedin the AJR last year. Dr. Goodwin has collaborated with Dr. Kauppinen of ourNMR Research Center on studies of the structure and imaging properties of articularcartilage; current work includes a projectcorrelating cartilage T2 with immunohis-tochemistry of early degenerative changesin articular cartilage in the human knee.
CT with a 3D reconstruction. The pathology includesa subtalar dislocation and a dislocation of the peroneal tendons.

21DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
BREAST IMAGING
Steven Poplack, MDAssociate Professor of Radiology
and of Obstetrics and Gynecology
Division Co-Director
Helene M. Nagy, MDAssistant Professor of Radiology
Division Co-Director
STAFF
Judith Austin-Strohbehn, MDHarte C. Crow, MDElizabeth Dann, MDRoberta diFlorio, MDPetra J. Lewis, MDHelene M. Nagy, MDSteven S. Poplack, MDTherese J. Vaccaro, MD
The Breast Imaging Division is dedicatedto women’s health and to providing up-to-date and compassionate breast-cancerscreening and diagnostic care. We participatein NCCC’s Comprehensive Breast CareProgram, an integrated approach to breast-cancer patient care which coordinates carefrom the departments of radiology, surgery,oncology, pathology, and radiation oncology. The division performs screening exams utilizing both traditional mammographyand MRI. Diagnostic imaging is performedwith mammography, ultrasound and MRI.Our mammography screening takes placein five exam rooms built around an all-digital complement of Hologic Selenia™
systems designed to maximize accuracywhile subjecting patients to less radiation,fewer call-backs, and less discomfort andanxiety.
The breast-MRI program, now directedby Dr. Dann, has experienced significantgrowth in recent years, being increasinglyused for breast-cancer screening of high-risk patients, as well as for diagnostic examsfor cancer staging. Interventional proceduresin the division include a range of image-guided needle- and vacuum-assisted biopsiesutilizing all three modalities—mammography,ultrasound, and MRI. MRI exams andprocedures are facilitated by a dedicatedbreast-MRI table/coil with built-in imagingoffering greater patient comfort, increasedimaging clarity, and access for interventionalprocedures. We work with colleagues inRadiation Oncology to perform image-guided catheter placement for acceleratedpartial breast irradiation. Additional imaging services include galactography, sentinel lymphadenectomy, and lymphoscintigraphy.
The curriculum for residents emphasizesdirect clinical experience, with responsibilities
and independence increasing in each of thethree month-long rotations. At the end ofthese rotations, the resident is expected tobe proficient in the entire spectrum ofscreening, diagnostic, and interventionalbreast imaging.
The division is active in funded and unfunded research and publishing. Dr.Poplack has for over ten years been clinicaldirector for the multi-disciplinaryAlternative Breast Cancer Imaging (ABCI)Program, in which Drs. Nagy and diFloriohave also participated. Other areas ofresearch interest include assessing MRI inmonitoring tumor cryoablation, and studieson the efficacy of the MammoSite® radiationtherapy system. Dr. Lewis has recentlypublished (AJR, 2009) an investigationabout the effectiveness of preoperativeMRI on patients with newly diagnosed breast cancer.
Digital breast tomosynthesis (DBT), an imaging technology which is likely tobecome an important adjunct to traditionalmammography, continues to be a researchpriority for the division. Division membersled by Dr. Poplack have pioneered DBTclinical studies. A new experimental DBTsystem installed last year will permit a number of new studies to go forward,including comparisons of DBT and breast-MRI, and —in collaboration with Thayerbiomedical engineers—a new five-yearNCI-funded program to assess the potentialof combining DBT with near-infraredspectral tomography. The ABCI program,the DBT studies, and other breast-imagingresearch are described in detail later in this report. The division supports theresearch efforts of the New HampshireMammography Network, which gathersand collates mammographic and pathologicdata on New Hampshire women.

CARDIOTHORACIC IMAGING
22
Julianna Czum, MDDivision Director
STAFF
William C. Black, MDJulianna Czum, MDDagmar Hoegemann Savellano, MD
The divisions of Chest and CardiacImaging have been recently reorganized asCardiothoracic Imaging. The divisiondirector, Dr. Czum, is fellowship-trainedin cardiovascular MR and subspecialtyboard-certified in Cardiovascular CT. Dr.Black, an outcomes scientist and authorityon lung cancer screening, divides his timebetween clinical and research endeavors,and is on the faculty of The DartmouthInstitute for Health Policy and ClinicalResearch. Dr. Savellano is a recent graduateof our residency program, with a significantresearch background in MR imaging.
Chest radiography and chest CT comprise a significant portion of the imaging performed in the department. Chest CTincludes dedicated non-contrast imagingfor interstitial lung disease, breathingmaneuvers to assess obstructive airwaysdisease, low radiation dose technique forfollow-up evaluation of nodular disease,and contrast-enhanced CT pulmonaryangiography, as well as standard protocolsfor airspace disease and oncology staging.
Non-invasive cardiovascular modalitiesinclude cardiac CT, coronary CTA, cardiacMR, and MR angiography. Cardiac MRstructural and functional evaluation is usedto evaluate pericardial, valvular, ischemic andnon-ischemic heart disease, as well as cardiacmass evaluation. Pharmacologic stress MRperfusion imaging is an alternative tostress echocardiography and myocardialperfusion scintigraphy. The delayedenhancement technique is used to localizeand quantify infarcted and viable
myocardium, as well as to evaluate cardiomyopathies. ECG-gated 64-detectorrow CT is a robust means to non-invasivelyimage the heart and coronary arteries inappropriate clinical circumstances.
With the aim of selecting the most appropriate evidence-based modality-protocol combinations for each patient’sunique circumstances, division staff consults on a daily basis with primary careproviders and a range of specialists includingpulmonologists, thoracic surgeons, thoraciconcologists, cardiologists, electrophysiologists,and cardiac surgeons. Daily intensive-careunit team rounds, weekly multidisciplinarythoracic oncology conferences, andmonthly pulmonary-radiology conferencesare characteristic of the collaborativeapproach to cardiothoracic care at DHMC.
Single midventricular short axis slice through left and right ventricles obtained with double inversion recovery “black blood” cardiac MR technique demonstrating normal anatomy.

23DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
A variety of new technologies continue to enhance the effectiveness of cardio-thoracic imaging. Thin-client softwareavailable at all workstations permits real-time assessment of pulmonary nodulevolume doubling time—an increasinglyimportant means for discriminatingbenign from malignant lesions. Post-processing of airways image data createsvirtual bronchoscopic reconstructionsthat aid in planning of transluminalinterventions and surgery. Co-registrationof 3D cardiac-MR or CT data with electrical maps permits radiofrequencyablation of lesions with increased safety, improved accuracy, and reducedcomplications. With increased surgicalsuccess in treating pediatric victims ofcongenital heart disease, cross-sectionalMR or CT surveillance has becomeboth more effective and more essentialin monitoring chronic post-operativesequelae and in the timing of furtherinterventions.
Radiology residents spend 14 weeks in cardiothoracic imaging rotation, as 4-or 5-week blocks in the first, third andfourth years. Didactic lectures (one pulmonary lecture and one cardiac lectureeach month) are based on the knowl-edge-based objectives of the Society of Thoracic Radiology curriculum. The third and fourth year rotationsinclude a cardiology option offeringexposure to transthoracic and trans-esophageal echocardiography, invasivecoronary angiography, and electrophysi-ology procedures. Cardiology fellowsrotate through the department for experience in cardiac MR and CT, inaddition to nuclear cardiology training.Pulmonary fellows and internal medicineresidents spend the majority of theirradiology elective time in chest imaging.
Medical student education includes lectures in chest imaging during second-year courses in pulmonary medicine and cardiology by Drs. Czumand Black, both of whom have received
teaching awards. The regular fourth-yearradiology elective includes participationin chest imaging read-out sessions; and,through the individually-tailored electivesalso available to third and fourth yearstudents, the possibility of additional cardiothoracic imaging experience.
Dr. Black is one of the principal designersof the National Lung Screening Trial(NLST), a major multi-center trial comparing non-contrast CT with chestradiography in cancer screening ofsmokers; he is PI for Dartmouth-Hitchcock and also directs the study’scost-effectiveness component.
Quality improvement projects being undertaken include systematic radiationreduction for chest CT studies as well asan ongoing collaboration with radiologictechnologists using a PACS-basedreporting system for image quality assurance that has resulted in improvedproblem-solving, performance metrics,and in-service education initiatives.
Our newest MRI system, the GE MR750 3T, enhances capabilities across a broad range of indications and imaging needs, including functional MR brain imaging.
The MR750 arrives—January 2010.

VASCULAR AND INTERVENTIONAL RADIOLOGY
The Division of Vascular and InterventionalRadiology (VIR) performs image-guided,minimally invasive procedures rangingfrom basic interventions (e.g., biopsies,abscess drainage, central venous access) to more complex procedures such as pulmonary thrombectomy, Yttrium-90radioembolization for hepatic cancers,radiofrequency ablation and cryoablation(for liver, renal, bone, and lung tumors),vertebroplasty, stent-graft repair of arterialor dialysis access aneurysms, and uterineartery embolization for the treatment ofsymptomatic fibroids. Imaging modalitiesinclude fluoroscopy, ultrasound, and computed tomography. The VIR staffprovides consultation to physiciansthroughout the institution and northernNew England, and manages inpatientservice and the VIR outpatient clinic. We participate in multidisciplinary conferences in trauma, vascular surgery,oncology, urology, and gastroenterology—interdisciplinary collaborations thatunderline our commitment to providecare based on the most effective, evidence-supported therapies.
Each of our attendings holds ABMS subcertification and 9 to 19 years of subspecialty VIR experience. Dr. Hoffer,division chief since 2005, offers expertisein transcatheter embolization for traumaticinjury, stent graft repair of aortic trauma,and TIPS treatment for portal hypertension.Drs. Forauer, Gemery and Hoffer are full-time interventional radiologists; Drs.Silas and McNulty are part-time, withclinical responsibilities in other areas ofthe department. The inpatient clinicalside of the service is largely coordinatedby our versatile associate providers, nurse
practitioner Shari Evans and physicianassistant Anne Michaels. They are involvedin all phases of inpatient care—fromensuring thorough pre-treatment patientevaluations to post-discharge follow-up.The associate providers also independentlyperform routine procedures such as paracentesis, thoracentesis, chest tubes, and central venous access. Shari andAnne hold faculty positions at DMS asclinical instructors and are integral in theeducation of hospital nurses and residents,and play an active role in research andquality improvement initiatives. Thedepartment maintains a nurse-staffedPICC service—only the most difficultcases require referral to VIR.
24
Eric K. Hoffer, MDDivision Director
VIR Fellowship Director
STAFF
Andrew R. Forauer, MDJohn M. Gemery, MDEric K. Hoffer, MDNancy J. McNulty, MDAnne M. Silas, MD
ASSOCIATE PROVIDERS
Sharene Evans, ARNPAnne Michaels, PAC

DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010 25
Our facilities consist principally of 4angiographic suites, two of which utilizestate-of-the-art flat panel systems. TheSiemens digital flat panel biplane system,our most recently installed unit, includespowerful software for reconstructing axialimages from selective contrast injections—a feature which permits precise subselective catheterization for tumorembolization procedures. Each of thesesuites also contains a dedicated ultrasoundunit. In addition, CT-guided interventionsare performed on a new Siemens wide-bore fluoro-CT unit.
The division plays an active role in the training of fellows, residents, and medicalstudents. Residents typically rank VIRamong the most demanding, andrewarding, of their radiology rotations—and in recent years roughly one quarterhave chosen VIR fellowships. We aregrateful to our institution’s vascular surgeons for their role in fellow education;the endovascular rotation provides experience in the vascular ultrasound laband in clinical and endovascular treatmentof peripheral vascular disease, includingabdominal and thoracic aortic stent graftingand carotid stenting.
Research interests of the VIR staff include:endograft repair and transcatheterembolization (Dr. Hoffer); dialysis accessmaintenance and percutaneous therapiesfor renal neoplasms (Dr. Forauer); CTsummation techniques in radiofrequencyablation (Dr. Gemery); chest port place-ment and image-guided liver biopsy
(Dr. Silas); dialysis access and radiologyeducation (Dr. McNulty). Recentnational conference activities includepresentations on arterial closure devices,IVC filters, and antibiotic prophylaxis.Current or considered trials includestudies of regional cancer therapies, such asYttrium-90 radioembolization of primary
or metastatic liver disease, cryoablationfor renal tumors; dialysis access mainte-nance in the elderly; evaluation of aheparin-bonded hemodialysis catheters;and transcatheter arterial chemotherapyfor bladder neoplasms.
The Siemens Artis zee biplane angiography system, used in a range of interventional procedures (such as the embolization pictured on the cover of this report) by the VIR and neuroimaging teams.
NUCLEAR IMAGING
Alan H. Siegel, MD, MSDivision Director
STAFF
Helene M. Nagy, MDPetra J. Lewis, MDMarc A. Seltzer, MDAlan H. Siegel, MD, MSStephanie P. Yen, MD
NUCLEAR STRESS LAB STAFF
Robert S. Foote, MDCharles Herr, MD
26
Necrotic lung cancer, appearing as dark ring in lower PET images, and as a bright ring in fused PET-CT images in top row.
Nuclear Imaging traditionally has beenbased on measuring variation in tissueconcentrations of radioactive biomarkers,providing data which can be correlated to specific states of organ function andpathophysiology. The resulting functionalimages are then used to complement thestructural imaging obtained by radiographicor MR studies. The past decade, however,has seen a fundamental shift in nuclearimaging technology with the advent ofhybrid systems which combine functionaland structural imaging. Our department has been on the cutting edge of theseinnovations, adding two SPECT-CT scanners—one of which, added in 2009,includes full ring diagnostic CT—and anon-site fixed PET-CT system which wasthe first in northern New England andremains the only fixed PET-CT scanner in the state.
The Division of Nuclear Imaging providesa full range of diagnostic imaging and therapeutic procedures. To the diverseselection of studies offered, the division hasadded, within the past several years, cardiacPET imaging for myocardial viability,Zevalin® studies (imaging and therapy forlymphoma, performed in conjunction withthe Section of Radiation Oncology),Therasphere® studies (for liver malignancy,performed in conjunction with theDivision of Interventional Radiology andthe Section of Radiation Oncology.)
The Nuclear Cardiac Stress Lab, under thedirection of Dr. Foote (board certified inInternal Medicine and NuclearCardiology) is a regional referral center for noninvasive assessment of all types of cardiac pathologies. Exercise andpharmacologic stress and rest imaging

27
studies are performed to assess a varietyof diagnostic and prognostic parametersand to measure ventricular size andfunction. Research focus in the lab hasbeen on measures of exercise capacity,new myocardial imaging agents, andnovel biomarkers of myocardial ischemia.The Dartmouth group was the first inthe world to publish evidence clarifyingthe sensitivity of cardiac stress testing, aswell as the first to demonstrate elevationof certain neurohormones in the bloodof patients with transient myocardialischemia.
The division continues to play a key role in PET and PET-CT education ona national level. Under the direction ofDr. Seltzer, who serves as director of ourPET-CT program, we conduct regularsessions of the teaching seminar, Frontlineof PET-CT. This course is given severaltimes per year and has been attended by radiologists and nuclear medicine
physicians from across the United Statesand from as far away as Asia and SouthAmerica. The division hosts a highlyregarded annual symposium The Role of PET-CT in Cancer Management. Andin partnership with the AmericanCollege of Radiology, division facultyled by Dr. Seltzer conducts “ACR-Dartmouth PET/CT,” a three-daycourse offered each June, September and December in Reston, Virginia.
The division pursues a variety of researchinterests, is active in quality improvement initiatives, and has participated in severalrecently concluded or ongoing clinicaltrials. These include: a multicenter studyon the role of dopamine receptors in the diagnosis of Parkinson’s disease; theuse of fatty acid tracers for the imagingof myocardial ischemia; FDG in thediagnosis of Alzheimer’s disease; and iscurrently participating in a multi-center
trial testing the value of F-18 sodiumfluoride for defining skeletal metastases.Drs. Foote and Herr, in the CardiacStress Lab, have conducted extensivework on the use of brain natriureticpeptide (BNP) in the diagnosis of heartdisease.
Division Director Dr. Siegel also serveson the D-H Information SystemsSteering Committee, is chair of its subcommittee on Medical Imaging, andis a member of the institution’s ClinicalInformatics Committee and is Directorof Radiology Informatics. He wasrecently awarded a DMS LearningTechnology Venture Fund grant todevelop a web-based teaching file application that facilitates image-uploadsfrom any workstation, providing an easily accessible repository of cases andeducational material.
DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
Third Annual Dartmouth-Hitchcock Symposium, The Role of PET-CT on Cancer Management. March 2010, Bretton Woods, NH

PEDIATRIC RADIOLOGY
Steven K. Sargent, MDDivision Director
STAFF
Steven K. Sargent, MDTherese J. Vaccaro, MD
28
The Division of Pediatric Radiology, as a component of the Children’s Hospital at Dartmouth (CHaD), participates across a broad spectrum of clinical cases,consultations, and teaching obligations.We expect that CHaD’s caseload growth,driven in part by integration with thepediatric community in the southernHitchcock Clinic division, will result incontinued growth in imaging volumes.CHaD has three pediatric general surgeons,two pediatric neurosurgeons, three pediatriconcologists, three pediatric urologists—and, for the first time, a pediatric otolaryngologist. The Child Protectionand Advocacy Team handles referrals fromaround the region. This increase in staff isexpected to provide increasing volumes ofpediatric radiology cases.
Radiology’s PACS system makes it easy to correlate different pediatric imagingstudies and enhances both the consultativeand clinical aspects of pediatric radiology.Integration of the PACS systems betweenD-H north and south now allows viewingand consultation on cases imaged inManchester. 64-slice CT scanning andmore powerful MR imaging permits fast3D reconstructions that are especially useful for vascular anomalies. Newlyacquired Visage™ software brings this multiplanar and 3D capability to readingstations throughout the department. Thefaster scan times also reduce the need forsedation.
Minimizing radiation dose in children’s imaging is among our highest concerns.We support Image Gently, a campaign ledby The Society for Pediatric Radiologyaimed at decreasing children’s exposure toionizing radiation. Pulsed fluoroscopysystems, available in all of our fluororooms, are important components in this effort, as they permit significantly
deductions in radiation dose. The “PainFree CHaD” program has also helpedmake the pediatric sedation required bysome of our procedures (e.g., a voidingcystourethrogram) safer and less stressfulfor children and their families.
Pediatric Radiology continues its vigorousteaching service, and participates in thetwo-year core curriculum for radiologyresidents. We conduct board review sessions for senior residents, and the pediatric elective is popular with the radiology house staff. For the DMS medical student elective, we participatewith lectures, biweekly film sessions withthe Neonatal Intensive Care Unit team,and weekly sessions with both thePediatric Inpatient and Intensive CareUnit teams. Pediatric Radiology participates in the pediatric tumor board conference.
URORADIOLOGY
Anne M. Silas, MDDivision Director
29
The Uroradiology Division in recentyears has seen significant increases in bothpatient volumes and in the variety andcomplexity of cases. We conduct examsin CT, MRI and Ultrasound. Advancedimaging in the division includes multi-phasic CT imaging, CT angiography, andCT urography. 3D CT reconstructionsare a key facet in the pre-operative anddiagnostic workup of the urology patient.
Much of the growth in uroradiology cases is driven by the expansion of theinstitution’s Urology Section, which continues to add services and physicians.In 2005, a Pediatric Urology section wasestablished, led by CHaD director, Dr.Paul A. Merguerian. With the addition ofa third pediatric urologist in 2008, Dr.Leslie McQuiston, the new section hascontributed to the steady increase in thenumber of pediatric patients seen in theUroradiology Division.
The weekly uroradiology conference, used to review the diagnostic imaging
and management strategies of urologypatients, is a dynamic meeting betweenthe two specialties. During this conference, various imaging studies arepresented in an “unknown case” formatto urology residents by radiology residents. Numerous facets of diagnosisand management are discussed, and treatment options are designed.
Over the past two years, a core series of uroradiology lectures has been developed. Repeated yearly, these lectures cover a wide range of topics,from intravenous urography techniques to the evaluation of adrenal masses andhysterosalpingography. Additional sessionsfor oral boards preparation are given inthe spring. Though aimed at graduatingseniors, “boards review” is often attendedby junior residents who acquire a bettersense for “taking the unknown case” bywatching the seniors perform.
CT urogram study, AP view of 3D volume of kidneys, ureters and bladder, with and without transparent bone overlay.
DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010

VETERAN’S ADMINISTRATION
Richard A. Morse, MDActing Director of VA Radiology
30
The Veterans Affairs (VA) RegionalMedical and Office Center in WhiteRiver Junction, VT, participates withDHMC and DMS in a range of medicalstudent and residency education programs.The VA Hospital is a tertiary care hospitalthat serves veterans in northern NewHampshire and the state of Vermont. Inaddition to the main hospital, five satelliteclinics offer services to veterans in theregion.
The VA Hospital’s Department of Radiology is completely digitized with a PACS that includes voice-recognitiontranscriptions. Facilities include a mobileMRI unit operating four days/week, a64-slice MDCT scanner, two GE Logic 9ultrasound units, DXA bone densitometryscanning, and a newly renovated angiosuite with a tilt table. Mobile PET/CTimaging, on a weekly basis, is expected to become available in the near future.Plans for a $7 million imaging centerhave been approved, with constructionslated to begin later this year; among theenhancements provided by the new center will be the addition of a fixed MRI system. The Radiology Departmentis staffed by four full-time radiologists andone part-time radiologist. Dr. Morse, fellowship trained in cross-sectional imaging, leads the department as the
Acting Chief of Radiology. Dr. Harpercoordinates the resident rotation at theVA, is DMS Assistant Dean of MedicalEducation (responsible for the residencyadvising process for medical students) andserves as DMS representative for theNational Residency Matching Program.Dr. Lenz heads the InterventionalRadiology Section. Dr. Smith practicesgeneral radiology with a focus on CT and MR imaging. Dr. Burns, a formerDHMC radiology resident, recentlyjoined the VA staff after completion of a cross-sectional imaging fellowship atFletcher-Allen.
Two vital aspects of the VA’s mission are education and research. Teaching of medical residents and students is offeredthrough a daily radiology/medicine conference as well as the weekly TumorBoard. Radiology residents rotatethrough the department three days perweek in two week blocks, with a focus on CT, plain films and fluoroscopy, as well as participation in the daily conferences. The VA faculty is currentlyinvolved in research collaborations withthe sections of Oncology and Urology, and participates in the VA’s NationalCancer Care Collaborative qualityimprovement projects.
Susan N. Harper, MDDirector of VA Radiology ResidentEducation
STAFF
Tien Burns, MDSusan N. Harper, MDJames Lenz, MDRichard A. Morse, MDEdward Smith, MD

DIAGNOSTIC PHYSICS
John B. Weaver, PhDDivision Director
31
The Division of Diagnostic Physics, in addition to research and teachingactivities, is responsible for quality control(QC) for all imaging modalities.Specifically, this entails meeting the regulatory and radiation safety require-ments of the Radiology Department and the medical center, as well as thoseof outside organizations, including ACRaccreditation for the Breast ImagingCenter, the State of New Hampshire, and the FDA.
The primary goal of QC is to insure optimal performance of all componentsof the imaging environment—achievingthe highest possible image quality at the lowest possible radiation dose.Representative X-ray exposures for themost common procedures are measuredannually for each X-ray producingdevice. Results are kept on record andare available for use in patient-physicianconsultations on request. Finally, the QCprogram seeks to help contain costs byidentifying unnecessary or unproductivesteps in the complex chain leading tofinished and useful studies.
Dr. Weaver teaches essential diagnostic physics to radiology residents, with thecurriculum regularly updated for changesin the ABR physics exam, such as thenew emphasis on conceptual questions.Dr. Weaver continues to teach biomedicalengineering and bioinformatics at theThayer School of Engineering, and nowteaches a biannual course for cardiologyfellows on the physics of imaging.
Dr. Weaver plays a key role in imaging research conducted within the departmentand in collaboration with investigators
throughout the Dartmouth community—particularly with the divisions of neuro-radiology and breast imaging, and withthe biomedical engineering faculty atThayer. Many of these investigationshave emphasized the development ofnew imaging modalities or clinical applications involving new combinationsof existing techniques. Described ingreater detail later in this report, high-lights of recently concluded or ongoingstudies include:
• Magnetic resonance elastography for thedetection of breast cancer, in which amodified MR scanner creates imagesbased on the differing elasticity ofbreast tissue;
• techniques for enhanced and more versatile monitoring of neoadjuvantchemotherapy progress;
• the development of techniques forimaging soft-tissue properties in thediabetic foot, with the clinical goal ofearlier detection of foot infection inthis vulnerable population;
• Frequency Domain Optical Imaging ofBreast Cancer, which aims at establishingthe diagnostic potential of a singleplatform combining the functional-imaging advantages of NIR with thespatial resolution of MR;
• MR Microwave Absorption and TomographyImaging, seeking the development ofhybrid imaging modalities (possiblyin a single combined platform) basedon magnetic resonance microwaveabsorption and magnetic resonance-compatible microwave tomography.
DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
SPEARE MEMORIAL HOSPITAL
The department provides radiology services to Speare Memorial, a recentlyrenovated and expanded critical-accesshospital in Plymouth, NH. Dr. Troughtdirects the program, heading up a part-time DHMC-based staff which includes Drs. Crow, Nagy, Harris, Hoegemann-Savellano, and Sargent. The staff alsointerprets studies generated—and directlyentered into the Speare PACS—at thenew Boulder Point off-site outpatientfacility.
Radiology facilities are fully digital andinclude standard diagnostic radiographysystems, a Philips Eleva fluoroscopy unit,an upgraded (to 16-slice) Philips CTscanner, and a new Hologic digitalmammography unit. All studies are displayed and stored on a Philips PACS,with dictations processed by MedQuist’sSpeechQ™ voice recognition system.MRI and nuclear medicine exams areperformed on mobile units; the MR
system was recently upgraded, and thenuclear imaging system is slated for new software and an upgrade to a dual-head camera.
Speare Radiology plays an active role in medical education. The radiologyelective for DMS students includes visits to Speare for insight into the practice of radiology in a small community hospital. DHMC fellowsand senior residents are encouraged toinclude rotations at Speare, a voluntaryposting which provides the experience ofa small-hospital setting and a degree ofindependent practice not as easily foundat the Lebanon campus. All residents, aspart of routine on-call responsibilities,participate in reading overnight examstransmitted from Speare.
SOUTHERN NEW HAMPSHIREDartmouth Hitchcock Medical Centerand Dartmouth Medical School are components in the Dartmouth-Hitchcock healthcare system, which also includes a network of independentmulti-specialty community group practices, mainly in southern NewHampshire, of which the most significantare at Concord, Manchester, Nashua, and Keene. CHaD, the Children’sHospital at Dartmouth, operates facilitiesin Manchester, Plymouth, and atWentworth-Douglass Hospital in Dover.A network of smaller community practices are found in a half-dozen otherNH locations.
The major D-H facilities in southern NH are now linked to the department’sPACS/RIS system, providing a seamlessimaging and patient-records network in which cooperation is facilitated and encouraged—and the quality of
patient care significantly enhanced. Our residents rotate through the radiology departments of these affiliatedinstitutions, and physicians from theseaffiliates frequently participate in collaborative and educational events at our campus. The various radiology
facilities of these affiliates are now members of an organizationally coherent single department under the leadership of Daniel Abbis, DO,Radiology Director for Southern New Hampshire.
MOBILE PET-CTDr. Seltzer directs our outreach programof providing interpretations of PET-CTscans performed at regional institutions by a mobile PET-CT scanner operatedby New Hampshire Imaging Services.At present, we receive and read studiesperformed once weekly at Weeks MedicalCenter Hospital, Lancaster, NH.
CLINICAL PROGRAMS OUTREACH
32
William S. Trought, MD, FACRDirector, Spear Radiology
Daniel J. Abbis, DODirector, So. NH Radiology

DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010 33
PORTABLE ULTRASOUND INITIATIVE
Dr. Harris, Director of UltrasoundEducation and Research, has been conducting research and taking directpersonal involvement into the plight ofwomen facing pregnancy and birth inless-developed areas around the globe.No single diagnostic technology holdsmore promise than ultrasound in preventing maternal, fetal and neonataldeaths—and serious complications such as obstetric fistula. Dr. Harris isamong a group of informally affiliated
radiologists who have been bringinglow-cost portable ultrasound units to rural clinics. In the past several years, he has delivered ultrasound units andprovided instruction to clinics inVietnam, Nicaragua, Serbia, SierraLeone, and, earlier this year, Haiti—avisit coinciding with the devastatingearthquake. Dr. Harris’ review articledescribing this public health initiativewas published in 2009 in the Journal ofUltrasound in Medicine.
Robert D. Harris, MD, MPH, with patient in a rural clinic in Sierra Leone, demonstrates scanning procedures with a portable ultrasound unit he has delivered.

Radiologic Technologists (RTs) are atthe heart of our clinical mission—theimaging specialists whose work in X-ray,CT, MRI, ultrasound, mammography,nuclear medicine, and interventionalradiology produce the images used fordiagnosis and, increasingly, for image-guided treatments. Skilled technologistsare truly multi-faceted, their workrequiring not only technical expertise intheir imaging specialties, but competenceand compassion in communication—with physicians, equipment technicians,and most of all, with patients. RTs areto a large extent the “human face” of our practice, responsible for fostering a clinical environment which encouragestrust and confidence. They greetpatients, provide reassurance and guidance,and ensure that patients understand andare comfortable with post-procedureinstructions when needed. And ofcourse technologists conduct the examitself, responsible for patient safety andcomfort while providing high-qualityimaging results for radiologists and referring physicians.
INNOVATION
RTs work hard to promote an environmentof collaboration and innovation, andplay a major role in the introduction andimplementation of quality-of-care andpatient safety improvement. The RTstaff has embraced, with other areas ofthe institution, a number ofStuderGroup Hardwiring Excellencerecommendations. These include teamleader “rounding,” a formalized two-way communications process for proactively identifying problems andopportunities, and other programs (e.g.,“AIDET”) for improving provider-patient communication skills.
The RT staff took a leading role in theshift to an all-digital imaging work-place—a transformation that could nothave happened without their dedicationand innovativeness. The conversionrequired enormous modifications inworkflow practices at a time when protocols for digital imaging had not yet
been fully determined or standardized. Gerry Bergen, recently retired DX teamleader, wrote Digital Image Standards forRoutine Radiography, a reference manualdesigned to fill that vacuum; it remains a key resource not only here, where it has been updated and reprinted severaltimes, but for RTs throughout the countryand internationally.
When CT tech Kayla Denny was askedto take on 3D Lab responsibilities, sheresponded with the resourcefulness typicalof the RT staff. With mentorship fromDrs. Zhen and Tsapakos, she quicklymastered the necessary techniques,assembled an illustrated manual systematizing 3D protocols, trained additional RT’s, and paved the way for“24/7” service in 3D reconstruction.Innovation need not be purely technical:warming and humanizing the clinicalenvironment remain an important aspect of the RT staff ’s dedication tocompassionate professionalism. Many ofour pediatric patients are seen in rooms full of murals, toys, coloring books,dinosaurs and Disney characters—allproducts of the individual talents andinitiative of our staff.
TECHNOLOGISTS IN RADIOLOGY
34
Front row: Rick Mazurek RT, Chriss Kvinlaug RN, Robert Ferranti RT, and Administrative Director JamesRoberts. Back row: Terri Lorandeau RT, and Dan Pluta RT.
Karen Burgess, M.Ed., RTClinical Operations Manager for DX,Mammo and Ultrasound

35
EDUCATION
Several of our technologists have beendesignated Philips Healthcare “super-users” for their comprehensive knowledgeand skill in the use of specific imagingequipment, and since 2006 we havebeen designated a luminary site forPhilips. DX-core technologists hostdemonstrations and training in for visitors,an important teaching role and also anopportunity for our staff to share insightswith representatives of other institutions.The relationship also provides earlyaccess and preferential pricing to the
newest of Philips’ X-ray systems—in2009, wireless digital X-ray detectors forthe first time become available andDHMC Radiology was the first U.S.institution to beta-test the Philips’ entryinto this market.
For almost 20 years, the RT staff, led by DX co-team leader Brenda Sleasman,has conducted spring and fall radiologyeducational conferences. RT specialists,industry representatives and radiologistsprovide instruction, demonstrations andworkshops on issues across the spectrumof imaging modalities. Widely attendedby our technologist staff as well as RTsfrom other institutions, the conferences
represent an efficient and valuable wayfor RTs to earn CME credit and staycurrent with changes and innovations inthe field.
DHMC Radiology collaborates with Lebanon College and the New HampshireTechnical Institute, hosting the clinicalrotations for their radiographer trainingprograms. The programs provide valuableexperience for our staff to share theirexperience with future generations ofradiographers, and significantly improvethe regional availability of well-trainedRTs. A new ultrasound training programis in the early stages of development. Tobe modeled on the current program atLebanon College, the project involvesthe participation of several other hospitalsin our region. RTs also play a key role in medical student instruction andresident training.
LEADERSHIP
Technologists are encouraged to pursuecareer development, including newmodalities training, the assumption ofmanagement responsibilities, and ultimatepositions as team leaders. Filling management roles from within has longbeen a feature of the department, and isone of the key factors in the remarkablestability of our staff. Six of our ten team leaders have been with us for 25years or more: Dan Pluta, Dennis Seguin,Bob Ferranti, Rick Mazurek, BrendaSleasman, and Terri Lorandeau. Theremaining team leaders—Jessica Rider,Heidi Nystrom, Jerry Seamans—havesomewhat less tenure in their positionsbut no less expertise.
Clinical Operations Manager for DX,Mammo and Ultrasound since 2008,Karen Burgess, has spent over 18 years atDHMC, starting as an RT in RoutineX-ray and Mammography. She left usfor a time to pursue interests that includeddeveloping a public health program for
the city of Manchester, leading a nationalmammography study at DMS, and servingas Director of the Radiologic Technologyprogram at Lebanon College. ChrissKvinlaug, our newly-appointed ClinicalOperations Manager for CT, MRI, VIR,and Nuclear Imaging, moves into thisrole following many years as the highlyeffective director of the RadiologicNursing staff.
Administrative Director Jim Roberts served the department for many years as Clinical Operations Manager beforestepping into the role of ActingAdministrative Director in June of 2008;he was offered the permanent positionin September of that year. Versatile andexperienced in all imaging modalities,Roberts is a New Hampshire nativewho joined DHMC in 1975 and laterearned a BS degree at the NewHampshire Technical Institute.
DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
DX team leaders, Jessica Rider RT and Heidi Nystrom RT
Ultrasound team leader Dennis Seguin RT

NURSES IN RADIOLOGY
36
In 1994, Radiology hired its first nurse tomonitor patients during angiographies.Today, there are eighteen registered nurses—an increase driven mainly by fifteen years of steady growth in both thevolume and varieties of interventionalradiology. The nursing staff is involved in meeting patient needs throughout the department, but is essential for vascular and interventional radiology(VIR), where nurses are responsible forpatient care from planning to discharge.Facilities for image-guided interventionsinclude four dedicated angiography interventional suites and a 10-bed recovery room. In addition to their workin the angiography suites, nurses provide sedation, pain management, catheterizationand other services for patients undergoingCT-guided interventional proceduressuch as biopsies and drain placements;and, to a lesser extent, assist in image-guided procedures performed by the cardiothoracic imaging division and byneurointerventional radiologists. Nursesalso support patient csre in MR imagingwhrn sedation or pain management isneeded. The registered nursing staff issupported by licensed practical nurseswho provide a key role in managingpaperwork, maintaining recovery roomreadiness, assisting in patient care, andplenty of “behind-the-scenes” work tokeep the service running smoothly.
The nursing staff plays an active role inquality improvement initiatives. Lastyear, nurses developed a contrast-reactionsimulation exercise as part of a push to
improve the recognition and response topatients experiencing an adverse reactionto imaging contrast. In January of 2010, the nursing service achieved a 98% compliance rate in the institution’s handwashing audit—an important infection-fighting initiative. Other recentor ongoing QI projects in which thenursing staff has participated includeaudits for pain assessment, and “scrub-the-hub,” a DMHC campaign to reduce IVaccess infection rate by more effectivecleaning techniques. Nursing ManagerChriss Kvinlaug is a member of thedepartment’s QI Steering Committee andspearheaded, with Dr. Dann, last year’saudit of contrast extravasation events.
Chriss Kvinlaug, RNRadiology Nursing Manager

RIS/PACS
Our recently upgraded picture archivingand communications system (PACS) is atthe heart of the radiology informationsystem (RIS) which has been developedover the past several decades to supportthe department’s clinical mission. JohnSundnas, RIS/PACS Administrator,heads a team responsible for maintainingall aspects of imaging informationacquisition, processing, utilization andstorage, and for anticipating future information systems needs in an environment of increasingly compleximaging systems.
Recent accomplishments include:extending our RIS and PACS to theHitchcock Clinic facilities in southernNew Hampshire; the implementation ofa system to effectively upload, store andintegrate patient studies from outsideinstitutions conveyed to us on CD orDVD. Hospitals and Health Networksmagazine ranks us among the nation’s“most wired” hospitals—a recognition ofthe ongoing institutional commitment toinformatics, toward which theRadiology RIS/PACS team remains akey contributor. The department relieson software systems provided by variousdevelopers and systems manufacturers,which include:
• GE Centricity RIS-IC
• Philips iSite PACS
• 3D and post-processing systems including GE Advantage Workstation(AWW), Visage Imaging, VitalImages, and Prism Clinical Imaging(for fMRI)
• AS Software for structured reporting
• SpaceTrax interventional inventory management
RADIOLOGY INFORMATICS
Informatics, as an organizing principleand as adapted to radiology, seeks tomaximize the effectiveness of technologywith integrated information systemscomprising all aspects of data acquisition,distribution, utilization, and storage. The most significant informatics initiativenow underway is the implementation of DHMC’s electronic health record(EHR). Known as “eD-H,” the systemwill work in concert with the depart-ment’s existing RIS and PACS to providecomputerized order entry (CPOE) andimmediate availability of completedimaging studies to clinicians throughoutthe institution.
Enhancements slated to follow the initialeD-H roll-out include an automatedradiologic decision support system.Incorporated into a study request as acomponent of CPOE, decision supportwill provide referring caregivers withinformation on the relative appropriatenessof an imaging request, suggested alternativestudies, and a range of backgroundinformation including relevantmedical/scientific literature references. Anotheranticipated feature is the availability, viaelectronic transmission, of patient studiesfrom outside institutions. At present,such studies are conveyed on disk and
manually entered into RIS. Electronictransmission has special significance forincoming trauma patients, whose outsidestudies will be available for advancereview by radiologists and clinicians.
Department staff has been active in theadvocacy, development and implementationof electronic and online resources toenhance teaching and research. Dr.Siegel serves on the D-H InformationSystems Steering Committee, is chair ofits subcommittee on medical imaging,and is a member of the institution’sClinical Informatics Group. Drs. Lewis,McNulty and Siegel have created web-based learning tools that include applications to facilitate the creation ofteaching files by clinicians at PACS,online anatomy atlases, and a variety ofshared radiology resources for studentsand instructors. In the future, theseresearch and education tools will beincreasingly integrated into the clinicalimaging-data system.
John SundnasPACS/RIS Administrator
Alan Siegel, MDDirector of Radiology Informatics
INFORMATION SYSTEMS
37DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010

The department occupies 80,000 SF atDHMC’s Lebanon campus. Most of ourimaging facilities are located the northwestquadrant of the medical center’s thirdfloor. Additional systems (extremityMRI and one of the mobile MR units)are found on the second floor; in theDoctor’s Office Building (DXA,Mammography screening and tomosyn-thesis clinical trials); and in the EmergencyDepartment. Research facilities arefound at the medical school, and in variouslocations in the medical center.
Upgrading and expanding imagingsystems are an ongoing priority and are essential to all areas of our mission: state-of-the-art equipment improves diagnostic accuracy and procedural outcomes,improves efficiencies, improves patientsafety and comfort, and enhances teachingand research.
DX Core The diagnostic X-ray and fluoroscopy core, a designated PhilipsHealthcare “luminary site,” consists ofeleven exam rooms—among which are three fluoroscopy rooms, a PICCroom, and two rooms with automaticimage-stitching capabilities. Apart from the fluoroscopy rooms—which usePhilips EasyDiagnost Eleva™ systems—the Core utilizes Philips DigitalDiagnost™
systems as standard fixed equipment;eleven older GE portable CR units aredeployed as needed throughout themedical center.
The DX Core team also is responsible for imaging service in the EmergencyDepartment, where it operates aDigitalDiagnost VM unit (whichincludes Philips’ new wireless portabledetector), and the TraumaDiagnost™ CS-4. The CS-4 unit is mounted on anoverhead-rail system designed by formerFacilities Manager Paul Roy, an innovation
permitting the scanner to be easily repositioned for use at any of three ED bays.
DXA Scanning The department operatesa bone densitometry scanning service,utilizing the Hologic Delphi-W DXAsystem.
MRI The department utilizes six clinicalMRI systems: the GE MR750 3T mag-net (installed March 2010), a new GEHDX 1.5T system, an upgraded GESigna Twin Speed 1.5T, two leased 1.5Tsystems on mobile platforms, and theONI Medical Systems’ MSKExtremeTM 1.5T scanner—installedhere in early 2009 as the first clinicalapplication anywhere of this innovativesystem for imaging hands, arms, legs andfeet. In addition, the department main-tains a Philips 3T system used primarilyfor research purposes and housed atDHMC’s Advanced Imaging Center, andseveral small-animal research magnets atthe Vail and Rubin research laboratories.
Ultrasound The Ultrasound ImagingDivision operates six exam rooms, andequipment consisting of five Philips HDIscanners, two Philips iU22 systems, andfour Siemens Antares™ units.
Angiography The four-room angiographysuite for VIR procedures includes twoGE single-plane angiography systems, a GE Advantx™ LCN biplane unit, and a new (Jan. 2009) Siemens AxiomArtis zee™ biplane system that facilitates arange of interventional neuroradiologyprocedures.
Nuclear Imaging The Nuclear ImagingDivision utilizes four scanning systems:the Siemens Symbia T6™ SPECT-CTunit (Feb. 2009); the GE InfiniaHawkeye SPECT/CT; the GE Discovery ST™ PET-CT; and a Marconi IRIX Gamma Camera.
Computed Tomography CT systemsinclude: two GE Lightspeed 16-slicescanners, and a GE Lightspeed VCT 64-slice system. In early 2009 we expandedour capacities in CT-guided interventionswith the Siemens Somatom Definition™
AS system; offering multiplanar fluoro-scopic reconstruction and merged3D/real-time imaging. This versatile 40-slice scanner is used for a range ofimage-guided percutaneous interventions.
Breast Imaging Mammography screening and diagnostic studies are conducted on five Hologic Selenia™
full-field digital mammography systems. Biopsies are performed using a Selenia MultiCare™ Platinumstereotactic biopsy system. Breast-MRexams and interventions utilize aSentinelle™ Breast MR Auxiliary Tablewith 8-channel coil array. A new (2009)Hologic™ tomosynthesis system is usedfor clinical studies.
IMAGING SYSTEMS
38
The ONI extremity 1.5T scanner combines superbpatient comfort with resolutions typically foundonly on larger, fixed magnets.

39DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
The TruamaDiagnost CS-4 System, an in-house design that permits three ED bays to share one scanner.

MEDICAL IMAGING RESEARCH
40
The Department of Radiology and its faculty actively supportclinical and basic science research in medical imaging andimage-guided therapies. Within the department, research isconducted by a full-time, grant-funded research staff, as well asby our DHMC-based clinical faculty. (While many recentstudies by the clinical faculty are not described here—as thefocus of this section are the larger, externally-funded, andcross-disciplinary research programs underway—their work isan essential component of D-H imaging research, and thereader is directed to the list of publications in the appendix tothis report.)
The department’s research is best seen in the context of arobust commitment to medical imaging studies throughout aDartmouth medical and scientific community that includes various departments at DHMC and Dartmouth MedicalSchool, Norris Cotton Cancer Center (NCCC), ThayerSchool of Engineering, and The Dartmouth Institute forHealth Policy and Clinical Practice (TDI).1 Cross-disciplinarycollaboration is a common characteristic of this work, resulting in synergies which have established us as leaders inmultiple areas of medical imaging research.
I. RESEARCH FACILITIES
The principle resource for clinical radiology research consists of the department’s complement of radiographic, MR, CT, and molecular imaging systems. Additional clinical studies, as well as the bulk of the Dartmouth community’s basic-science imaging research, are conducted at several facilities, as described below.
The EPR Center The Electron Paramagnetic Resonance(EPR) Center for the Study of Viable Systems is home to theworld’s first clinical EPR system, has been for over fifteenyears a world leader in the development of biological and clinical applications for EPR spectroscopy, and plays a key role in international EPR research education and resourcesharing. The center operates several laboratories, including an instrument-development facility at the Hanover campus, asmall-animal research area within the NCCC (Rubin 6), and a clinical EPR facility in the Department of RadiationOncology (Rubin 2). Directed since inception in 1992 by Dr. Harold Swartz, the EPR Center staff includes Dr. Nadeem
Khan, Dr. Huagang Hou, Dr. Benjamin Williams, severaladjunct faculty researchers, and a growing number of researchassociates and assistants.
The NMR Center The Biomedical Nuclear MagneticResonance (NMR) Research Center conducts basic researchaimed at the development of MRI and MR spectroscopy(MRS) imaging techniques. A key focus is the use of MRS toidentify and depict concentrations of metabolites which can
be associated with specific tumor varieties. The resulting database of metabolic “fingerprints” may ultimately providesignificant clinical tools for cancer staging and treatment monitoring. The center also provides support for the neuro-science program at Dartmouth College, with ongoing investigations of fMRI techniques based on hemodynamics andoxygenation to probe brain activation, and of MRI and MRS‘biomarkers’ for detection of acute brain injury—researchwhich capitalizes on the neuroimaging background of Dr.Risto Kauppinen, director of the NMR Center since 2007.
1 For brevity, “Dartmouth” or “Dartmouth community” refers here to the academic and medical research community comprised of Dartmouth Medical School, Mary Hitchcock Memorial Hospital, Dartmouth-Hitchcock Clinic, Dartmouth College, the Thayer School of Engineering (“Thayer”), and affiliated institutions such as the Norris Cotton Cancer Center (NCCC) or The Dartmouth Institute for Health Policy and Clinical Practice (TDI).
NMR Center director, Risto Kauppinen, MD, PhD

41
The NMR Center operates a 7T Varian Unity-Inova high-field MRI scanner designed for rodent MRI andMRSpectroscopy. The capacities provided by the 7T unit areexpected to be augmented later this year with the installationof a 9.4T large-bore animal MR scanner. This NIH-fundedmagnet will accommodate larger subjects than the existing 7Tscanner, and offers improved sensitivity in both MRI and MRSmodes, opening new possibilities for NMR imaging researchand for affiliated Dartmouth researchers in neuroscience, cardi-ology and oncology. Dr. Kauppinen and the Department ofRadiology welcome the recent arrival of Dr. Barjor Gimi. Dr. Gimi, from the University of Texas, is a multi-disciplinaryspecialist in molecular microimaging with extensive back-ground in encapsulation nanotechnology.
The Advanced Imaging Center (AIC) The Advanced ImagingCenter at DHMC provides imaging support for NIH-fundedstudies, clinical trials and animal research studies, typicallyinvolving multi-disciplinary programs in cancer, vascular, andneurologic imaging. Specific projects include hybrid imaging(e.g., NIR-MR and MR elastography), novel contrast agentsfor early cancer detection, fMRI brain-activation studies, andaccurate image-based treatment guidance for heart disease andcancer. AIC facilities include a dedicated Philips whole-body3T MRI scanner, hybrid MRI-Near Infrared imaging withmicro-imaging capabilities, micro-PET, small-animal CT, and amicroCT specimen scanner.
The AIC includes the Neuroimaging Research Center, and theAlternative Breast Cancer Imaging Center (ABCIC), whichsupports research programs for the development of alternativebreast-cancer imaging modalities, and serves as an imaging clinicfor associated patient trials. With support from the NationalInstitutes of Health, the AIC was opened in 2006 as a jointventure by Mary Hitchcock Memorial Hospital, the DartmouthMedical School, the Thayer School of Engineering, and a number of clinical departments at DHMC. John Peiffer is the AIC Managing Director; Dr. Keith Paulsen Professor ofEngineering and of Radiology, is Scientific Director.
Cancer Imaging at NCCC The goal of the Cancer Imagingand Radiobiology (CIR) Research Program at the NorrisCotton Cancer Center is to foster a collaborative environmentthat promotes the incorporation of imaging, radiobiology, bio-physics, and engineering approaches into the development andevaluation of new cancer diagnostic and treatment strategies.The CIR program is co-directed by Thayer’s Dr. Keith Paulsenand Dr. Harold Swartz, Radiology’s Scientific ResearchDirector. The program utilizes the research labs at NCCC’sRubin and Borwell facilities, which include a variety of spectrographic and other imaging equipment, as well as theBrain Imaging Laboratory, where the Radiology faculty hasparticipated in fMRI neuroimaging research.
Thayer School of Engineering One of the key areas of research at Dartmouth’s Thayer School is medical imaging,especially in the development of new techniques for cancerdetection and staging. The alternative breast-cancer imaging(ABCI) program has been a central element in this work forover a decade. Related projects aim at developing “hybrid”platforms in which established modalities (e.g., MRI, CT and ultrasound) are combined with functional-imaging techniques such as near-infrared or microwave spectroscopy,electrical impedance tomography, or modified MR systemsdesigned to measure tissue elasticity. Additional hybrid imagingstudies underway include the use of fluorescence imaging coupled to MR and CT. Drs. Poplack, Weaver, Cheung andothers from the Department of Radiology participate in Thayer imaging research as consultants, clinical directors, or co-principal investigators.
DISCOVERY The Dartmouth Initiative for SuperComputingVentures in Education and Research (or “DISCOVERY”) is a supercomputing server cluster available to the Dartmouthresearch community. It consists (as of January 2010) of an 888-CPU Beowulf/Linux cluster with 3 Tb of memory, more than35 TB of disk space, and high-speed Infiniband interconnects.Much of the radiology research at Dartmouth—including mostof Thayer’s medical imaging work, and the alternative breast-imaging modalities program in particular—involves complexnon-linear image reconstruction which would not be possiblewithout DISCOVERY’s computational power.
II. RESEARCH PROGRAMS AND MAJOR PROJECTS
In the past five years, medical imaging research in the Dartmouth community has been supported by external grantstotaling nearly $40 million. The synergies, flexibility, and culture of teamwork associated with these multi-disciplinarycollaborations have energized imaging research and stand asone of this institution’s most distinguishing characteristics. Thefollowing summary includes medical imaging research from allfaculties and disciplines of the Dartmouth community.
Alternative Breast-Cancer Imaging Program Now in itseleventh year, the $15 million, NCI-funded Alternative BreastCancer Imaging Modalities (ABCI) program involves over 40 investigators throughout the Dartmouth community. The program seeks adjunct or alternative techniques to mammography and other existing modalities of breast cancerimaging. Keith D. Paulsen, PhD, Professor of Engineering and of Radiology, is PI for the program overall. Radiology’sDr. Poplack is PI for the clinical core component, with additional clinical leadership provided by surgical oncologistRichard Barth, medical oncologist Peter Kaufman, and pathologist Wendy Wells.
DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010

42
The investigational modalities of the ABCI, unlike mammography,differentiate tissue on the basis of metabolic and electromagneticproperties such as oxygenation, hemoglobin concentration, elasticity, and electrical conductivity. In addition to anticipatedimprovements in diagnostic efficacy, the new techniques do notsubject patients to ionizing radiation or compression of thebreast. Described below are the four principal modalities underinvestigation.
Magnetic resonance elastography (MRE) is based on the association of tissue stiffness and cancer—which is why a clinical breast exam involves physical manipulation to feel for hardness or lumps. MRE uses a modified MRI scannerto create images based on variation in breast-tissue elasticity.Project leader: John Weaver, PhD, Radiology Departmentphysicist.
Electrical impedance spectroscopy (EIS) uses a painless low-voltage electrode system to create a “tissue map” of the breastbased on variations in how cells conduct and store electricity. These characteristics (conductivity and permittivity) are usedto reconstruct images differentiating healthy from canceroustissue. Project leader: Alexander Hartov, PhD, Thayer Schoolof Engineering.
Microwave imaging spectroscopy (MIS) uses microwave deflection patterns to differentiate cell types on the basis ofwater content. Resultant high-contrast images can be usedfor diagnosing cancer and treatment monitoring. Projectleader: Paul Meaney, PhD, Thayer.
Near-Infrared Spectral Tomography (NIRST) utilizes the blood sensitivity and tissue-penetrating properties of near-infrared light to locate and quantify regions of hemoglobin, a key indicator of the microvascularity characteristic of cancerous tissue. The program is usingNIRST in two different configurations: as a stand-alone system designed to monitor tumors being shrunk withchemotherapy, and as a hybrid with MRI in which MR provides precise tumor location and NIR categorizes its vascular makeup. Project leader: Brian Pogue, PhD, Thayer.
Digital Breast Tomosynthesis (DBT) Recent controversy on the role of mammography screening in younger womenhighlights the need for further data and for improvedscreening technologies. Digital breast tomosynthesis (“DBT” or “BTS”) is a tomographic application of mammographywhich may lead to improved cancer-screening sensitivity, and reductions in unnecessary recalls and breast biopsies, particularly in younger women with denser breast tissue. DBT involves multiple low-dose X-ray exposures across an arcof motion, creating 3D views which can reduce the incidenceof false positives and false negatives found in conventionalmammography.
Drs. Steven Poplack and Keith Paulsen have helped establish Dartmouth as aleader in breast-cancer imaging research.
Breast Imaging technician, Joyce Wagner, with the Hologic SileniaDimensions DBT scanner.

DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010 43
Dr. Poplack and colleagues have been active in DBT researchsince its introduction, having conducted a groundbreaking earlyclinical trial comparing diagnostic tomosynthesis with that ofconventional film-screen mammography. Study results stronglysupport a clinical role for diagnostic DBT and suggested the likelihood of reduced unnecessary recalls when used inconjunction with digital screening mammography (AJR, 2007).Subsequently, we participated in a larger study, as one of fiveinstitutions in the nation’s first multi-center DBT clinical trial.
With research capabilities enhanced by the 2009 installation of a next-generation DBT scanner, several DBT studies are nowunderway. The first, a clinical trial sponsored by Hologic, Inc.,compares DBT and MRI for diagnostic accuracy in preoperativebreast cancer staging. The second is the R01 program, OpticalImaging Fused with Tomosynthesis for Improved Breast CancerDetection. This five-year program seeks to develop a clinicalexam platform combining the functional imaging of near-infraredspectral tomography (NIRST) with the detailed spatial resolutionof DBT—a hybrid device which may yield improved sensitivity,specificity, and a reduction in unnecessary patient call-backs.The program is led by Drs. Paulsen and Poplack, with theUniversity of Massachusetts, and DBT industry leader, Hologic,Inc.
Other Breast-Cancer Imaging Studies Breast-cancer imaging isthe clinical focal point of several additional projects. FrequencyDomain Optical Imaging of Breast Cancer looks at the diagnosticpotential of a single platform combining the functional-imagingadvantages of NIR with the spatial resolution of MR. MRMicrowave Absorption and Tomography Imaging, another NCI-funded project, seeks the development of two hybrid modalities(possibly in a single combined platform): magnetic resonancemicrowave absorption (MRMA) imaging, and MR-compatiblemicrowave tomography (MRMT.) Both studies are collaborativeefforts led by Thayer’s Dr. Paulsen and Radiology Departmentphysicist Dr. Weaver.
The routine use of preoperative breast MRI is recognized as a potentially powerful, if still controversial, diagnostic adjunct to breast mammography. In 2009, AJR published the results of a significant recent study on the procedure, directed byRadiology’s Dr. Petra Lewis. The role of breast MRI in the preoperative evaluation of patients with newly diagnosed breast cancer considered 199 patients with newly diagnosed cancerwho underwent breast MRI; for nearly 20 percent of thesepatients, additional malignant tumors were found by MRIwhich had not previously been discovered.
In Vivo EPR Programs Electron Paramagnetic Resonance(EPR) spectroscopy is a technique for studying chemical speciesthat have one or more unpaired electrons, such as organic andinorganic free radicals or inorganic complexes possessing a transition metal ion. The basic physical concepts of EPR are
analogous to those of nuclear magnetic resonance (NMR) andMRI, but it is electron spins that are excited instead of spins ofatomic nuclei. A number of unique capabilities for the measure-ment of physiologic parameters are available using EPR, includ-ing direct measurement of tissue pO2 through a repeatablenon-invasive measurement procedure and the measurement of endogenous free-radical species. In vivo EPR oximetry, thecentral research activity of Dr. Swartz’s EPR lab since inceptionin 1992, has a number of potentially valuable clinical applications.By means of accurate pO2 detection, EPR can be used tomonitor oxygen level in a variety of tissue types. In tumors,hypoxia is associated with angiogenesis as well as with resistanceto radiotherapy and chemotherapy; accurate assessment ofchanges in tumor pO2 can be used in cancer detection andstaging, and in monitoring of therapeutic efficacy. Other typesof vascular pathology are also associated with decreased tissue-oxygen levels, such as the ischemia caused by peripheral vasculardisease in diabetic patients and wound healing following radiationdamage to normal tissues. EPR oximetry could provide information critical for effective clinical management of theseand other oxygen-dependent pathologies and for the assessmentof novel therapeutic measures.
Recently, the center has focused on the development of radiation biodosimetry techniques and devices. In a disasterscenario involving the accidental or hostile release of significantlevels of ionizing radiation, public health officials remain without effective portable means of determining exposure levelsin affected individuals, jeopardizing the ability to carry outappropriate triage strategies. During irradiation, free radicalsare created in biologic tissues in proportion to the absorbed dose. In certain tissues, such as tooth enamel, bone, and nails,
EPR Center faculty researchers Drs. Huagang Hou, Ben Williams, and Nadeem Khanat a Rubin laboratory.

44
these radicals remain in a stable state following irradiation andtheir concentration can be quantitatively measured using EPRto estimate the dose. The center has received major fundingfrom a number of NIH and DoD sources, including the NIHCenters for Medical Countermeasures Against Radiation(CMCR) program and the Defense Advanced Research ProjectsAgency (DARPA). As this report goes to press, the EPR Centerawaits confirmation of an expected new $16.6 million five-yearNIH grant for dosimetry research.
In Vivo Optical Spectroscopy Associated with the EPRCenter, Dr. Roger Springett’s Redox Laboratory conductsindependent research on the uses of visible light spectroscopyfor imaging neural processes in the mammalian neocortexthrough the measurement of changes to mitochondrial oxygenation. Specifically, the current five-year NIH-fundedprogram, Imaging the Mitochondrial Response to Neural Activity,seeks to develop and validate spectral domain imaging technologyto collect and reconstruct images of the oxidation state of mitochondrial cytochrome, and of hemoglobin and extrinsicchromophore concentrations. Spectral domain imaging ofmitochondrial oxygenation, presently unique to Dr. Springett’slab, has the potential to add significant understanding of themanner in which the cortex process information, and alsooffers the possibility of precise, non-invasive location of tumors and other metabolically significant structures during certaintypes of neurosurgery.
Neuroimaging Research Dr. Weaver, Dr. Eskey, and the neuroradiology faculty continue collaborations—with theDartmouth Brain Imaging Laboratory, the Advanced ImagingCenter in projects including innovation in advanced 3T imagingin glioblastoma recurrence, fMRI imaging, MRI in pediatrichead trauma, CTA in intracerebral hemorrhage and aneurysmevaluation, imaging of pharyngeal carcinoma, vertebroplasty, and synovial cyst rupture. In addition, the Thayer School, independently and in collaboration with DHMC departmentssuch as Radiology and Psychiatry, has been active in a range ofneuroimaging research, including: the development of dynamicmultimodal imaging; fluorescence signatures for image-guidedneurosurgery; and molecular imaging for the detection ofglioma brain tumors.
Department-funded Research The Radiology ResearchCommittee, chaired by Dr. Belden (following several years ofcapable leadership by Dr. Harris), assists faculty, residents and fellows with clinical research guidance and seed grants madepossible by the Radiology Chair. In the past 3 years, the committee (also including Drs. Eskey, Weaver, Swartz, andBlack) has funded studies on: hemodialysis access outcomes and complications in the elderly; interventional radiology procedure in patients with abnormal coagulation parameters;thyroid nodule ultrasound characterization and differentiation of benign vs. malignant nodules (part of a multi-center trial);and interobserver variability of CTA aneurysm perception.
III. OUTCOMES RESEARCH
The Dartmouth Institute for Health Policy and Clinical Practice (TDI)—formerly known as the CECS—originated thepivotal Dartmouth Atlas and has taken a leading role in advancingoutcomes-based medicine. Nearly 20 years ago the RadiologyDepartment signaled its embrace of the principles of outcomesresearch by recruiting radiologist William C. Black, MD, to ajoint appointment with TDI. Dr. Black has developed andteaches a core curriculum on technology assessment, and isnationally recognized as an authority on the evaluation ofscreening and diagnostic testing. The department’s associationwith the institute has strengthened in recent years as five additional faculty members have earned MS or MPH degrees atTDI. In late 2008, we established the Radiology OutcomesGroup (DHROG) in order to identify opportunities to apply outcomes-based medical practice to clinical imaging, cost-effectiveness, physician education, and shared decision-making with patients.
The National Lung Screening Trial The National LungScreening Trial (NLST) is a randomized, multi-center studydesigned to compare the efficacy of two different techniques to screen for lung cancer: low-dose helical computerizedtomography (LDCT) versus chest radiography (“plain film” X-ray). With a budget of over $200 million and enrollment of over 53,000 current or former smokers with three annualscreenings for each, NLST is the largest randomized study of lung cancer screening in a high-risk population ever conducted, and represents a major milestone in the applicationof outcomes-research principles to a major public health concern.The NLST has generated widespread interest and considerablecontroversy, and will almost certainly impact future policy-making for lung cancer screening. Publication of study resultsand analysis is expected in 2011.
Dr. William C. Black
DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010 45
Radiology’s Dr. Black was instrumental in the design of thestudy, directs its cost-effectiveness component, is PI for theDHMC site, serves on numerous national committees for theNLST, and is slated to present study results at the 2010 RSNAAnnual Meeting. Dr. Black, in addition to clinical duties as achest imaging specialist, serves on the TDI faculty, and as Chairof the Outcomes and Economics Core Laboratory at theAmerican College of Radiology Imaging Network (ACRIN).
CER Center for Cancer Imaging In late 2009 a multi-institutional Dartmouth-initiated consortium was awarded a 2-year, $4 million NIH Recovery Act “Grand Opportunities”
grant for Comparative Effectiveness of Advanced Imaging in Cancer.Funding is provided for establishing a research center as a component in a national infrastructure for comparative effectiveness of cancer imaging research. The project, led byNCCC’s Dr. Anna Tosteson and Radiology’s Dr. Black, includesseveral Dartmouth community disciplines and faculties, as wellas the American College of Radiology Imaging Network(ACRIN), Brown University, and Tufts University’s Evidence-Based Practice Center.
The newest addition to our CT capabilities: the Siemens Somatom Definition AS

46
Judith Austin-Strohbehn, MDAssistant Professor of Radiologybreast imaging, gastrointestinal
Clifford J. Belden, MDAssociate Professor of Radiologyneuroradiology
William C. Black, MDProfessor of Radiology and Community
& Family MedicineDirector, Radiology Outcomes Researchcardiothoracic radiology
Jocelyn D. Chertoff, MD, MSProfessor of Radiology and OB/GYNVice Chair, Department of RadiologyDirector, Gastrointestinal Radiology
Yvonne Y. Cheung, MDAssociate Professor of Radiologymusculoskeletal, abdominal
Laurence D. Cromwell, MDProfessor of Radiology & Surgeryneuroradiology
Harte C. Crow, MDProfessor of Radiology and OB/GYN, Emeritusultrasound, cross-sectional
Julianna Czum, MDAssistant Professor of Radiology and MedicineDirector, Cardiothoracic Radiology
Roberta diFlorio, MD, MSAssistant Professor of Radiologybreast imaging, ultrasound
Elizabeth W. Dann, MDAssistant Professor of RadiologyDirector, Breast MRI
David A. Desrochers, MDInstructor of Radiology
Clifford J. Eskey, MD, PhDAssociate Professor of Radiology and of SurgeryDirector, NeuroradiologyDirector, Neuroradiology Fellowship
Andrew R. Forauer, MDAssociate Professor of Radiologyvascular and interventional
John M. Gemery, MDAssistant Professor of Radiology vascular and interventional
Douglas W. Goodwin, MDAssociate Professor of Radiology and SurgeryDirector, Musculoskeletal Radiology
Robert D. Harris, MD, MPHProfessor of Radiology and OB/GYNDirector, Ultrasound Education and Research
Eric K. Hoffer, MDAssociate Professor of RadiologyDirector, Vascular and Interventional RadiologyDirector, VIR Fellowship Program
Petra J. Lewis, MDAssociate Professor of Radiology and OB/GYNDirector, Radiology Medical Student Educationbreast imaging, ultrasound, nuclear imaging
David B. Haseman, MDAdjunct Associate Professor of Radiology
John J. McIntyre, MDAssistant Professor of RadiologyDirector, Spine Radiology Serviceneuroradiology, musculoskeletal radiology
Nancy J. McNulty, MDAssistant Professor of RadiologyCo-Director, Body Cross-Sectional Imagingneuroradiology, VIR
Anthony L. Merlis, MDAssistant Professor of RadiologyAssistant Director, Radiology Residency Programneuroradiology
Helene M. Nagy, MDAssistant Professor of RadiologyCo-Director, Breast Imaging breast imaging, nuclear imaging
David A. Pastel, MDAssistant Professor of Radiology neuroradiology
Steven P. Poplack, MDAssociate Professor of Radiology and OB/GYNCo-Director, Breast Imaging breast imaging, ultrasound
Steven K. Sargent, MDAssociate Professor of Radiology, ofPediatrics, and of OB/GYNDirector, Pediatric Radiology Director, Ultrasound Clinical Operationsgastrointestinal, pediatric, ultrasound
Dagmar Hoegemann Savellano, MDInstructor in Radiologygastrointestinal, cardiothoracic
Marc A. Seltzer, MD Associate Professor of RadiologyDirector, PET-CT Servicenuclear imaging
Alan H. Siegel, MDAssociate Professor of RadiologyDirector, Nuclear Imaging
Anne M. Silas, MDAssociate Professor of RadiologyDirector, Radiology Residency Programultrasound, vascular and interventional, uroradiology
Albert J. Song, MDAssistant Professor of Radiologymusculoskeletal
Peter K. Spiegel, MD, FACRProfessor of Radiology Chair, Department of Radiology
William S. Trought, MDAssistant Professor of RadiologyDirector, Speare Memorial Radiology
Michael J. Tsapakos, MD PhD Assistant Professor of RadiologyCo-Director, Body Cross-Sectional ImagingFellowship Director, Body Cross-Sectional
Therese J. Vaccaro, MDAssistant Professor of Radiology and Pediatricsbreast imaging, pediatric, ultrasound
Stephanie P. Yen, MDAssistant Professor of Radiologynuclear imaging, ultrasound
John B. Weaver, PhDProfessor of Radiologydiagnostic physics
CLINICAL FACULTY

DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010 47
Oleg Y. Grinberg, PhD Adjunct Associate Professor of Radiology
Hiroshi Hirata, PhD Adjunct Assistant Professor of Radiology
Ke Jian Liu, PhD Adjunct Assistant Professor of Radiology
Bernard Gallez, PhD Adjunct Assistant Professor of Radiology
Minoru Miyake, PhD Adjunct Assistant Professor of Radiology
Tien Burns, MDAssistant Professor of Radiology
Susan N. Harper, MD Assistant Professor of RadiologyDirector, VA Radiology Residency Program
James E. Lenz, MD Assistant Professor of Radiology
Richard A. Morse, MD Assistant Professor of RadiologyActing Director, VA Hospital Radiology
Edward Smith, MDInstructor in Radiology
Emily R. Baker, MDProfessor of OB/GYN and of Radiology
Robert S. Foote, MDAssistant Professor of Medicine and
of RadiologyDirector, Nuclear Cardiology Stress Lab
Charles Herr, MDAssociate Professor of Medicine and
of Radiology
Michele R. Lauria, MDProfessor of OB/GYN and of Radiology
Judith H. McBean, MD Assistant Professor of OB/GYN and
of Radiology
Misty Blanchette Porter, MDAssociate Professor of OB/GYN and
of RadiologyDirector, Assisted Reproductive Technologies
E. Rebecca Pschirrer, MD, MPHAssistant Professor of OB/GYN and
of RadiologyDirector, OB/GYN Ultrasound
Alexei Viazmensk, MD 2010-2011 MRI Travis Mastroianni, DO 2010-2011 Cross Sectional Imaging Stephen J. Guerin, MD 2010-2011 Neuroradiology Lawrence J. Briggs, MD 2010-2011 VIR
GL 5
Morgan Althoen, MD Benjamin Gilloon, MDJ. Allen Graham, MDBryan Navarette, MDVinay Ravi, MD
GL 4
Daniel Gibson, MDHazem Hawasli, MD Marc R. Jordaan, MBChB
GL 3
Christyna Faulkner, MDNicole N. Lee, MDJustin R. Lewis, MDRebecca J. Mueller, MDBenjamin Salter, MDJ. Derek Stensby, MD
GL 2
Hima Bindu Avutu, MDSword Cambron, MDKimberly Jenson, MDRobert Percarpio, MDArash Saemi, MD
Barjor Gimi, PhDAssistant Professor of Radiology and ofBioengineering
Huagang Hou, MD Research Assistant Professor of Radiology
Risto Kauppinen, MD, PhDProfessor of Radiology Director, Biomedical NMR Research Center
Nadeem Khan, PhD Research Associate Professor of Radiology
Keith D. Paulsen, PhDProfessor of Engineering and of Radiology
Roger J. Springett, PhDResearch Assistant Professor of Radiology
Harold M. Swartz, MD, PhD, MSPHDirector, EPR Center Professor of Radiology, Physiology, and ofCommunity and Family Medicine; AdjunctProfessor of Engineering and of Chemistry
Benjamin B. Williams, PhD Research Assistant Professor of Radiology
Ruhong Dong, MD
Maciej M. Kmiec, M.Sc.
Venkata Krishnamurthy Nemani, PhD
Piotr Lesniewski, M.Sc.
Sriram Mupparaju, MS
Namjoon Kim, PhD
Maureen O. Ripple, PhD
Yasuko S. Sakata, MD, Ph
CLINICAL FACULTY ( VA Hospital ) CLINICAL FACULTY ( Secondary Appointments in Radiology )
RADIOLOGY FELLOWS
2010-2011 RESIDENTS
RESEARCH FACULTY
ADJUNCT RESEARCH FACULTY RESEARCH ASSOCIATES
Jennifer Krawitt, MD 2009-2010 MRI Todd Noce, DO 2009-2010 Cross Sectional Imaging Scott D. Smith, MD 2009-2010 Neuroradiology

48
FACULTY PUBLICATIONS
Includes journal articles and book chapters by theclinical radiology faculty published since January2006. Research faculty publications are since January2007. Not included are publicationsby clinical facultywith secondary appointments in radiology, nor by theradiology staff of the VA Hospital. Residents are indicat-edby asterisks.
Ledet EH, Jeshuran W, Glennon JC, Shaffrey C, De Deyne P, Belden C, Kallakury B, Carl AL.Small Intestinal Submucosa for Anular DefectClosure: Long Term Response In An In Vivo SheepModel. Spine. 2009;34(14): 1457-1463.
Barry G, Khachikian S, Beck A, Belden C, PearceJ, Simon J. Optic Canal Diameter in InfantileOsteopetrosis. J Ped Ophthalmol and Strabismus.J Ped Ophthalmol Strab. 2009;46(2):112-114.
Cooper JS, Mukherji SK, Toledano AY, Belden C,Schmalfuss IM, et al. An Evaluation of theVariability of Tumor-Shape Definition Derived byExperienced Observers from CT-Images ofSupraglottic Carcinomas (ACRIN protocol 6658).Int J Radiat Oncol Biol Phys. 2007 Mar; 67 (4) 972-975.
Schenck JF, Zimmerman EA, et al. (Belden C).High-field Magnetic Resonance Imaging of BrainIron in Alzheimer Disease. Topics in Mag ResImaging. 2006 Feb;17(1):41-50.
Mills DM, Tsai S, Meyer DR, Belden C. Pediatricophthalmic Computed Tomography and associatedcancer risk. American Journal of Ophthalmology.2006;142 (6):1046 —1053.
Black WC, Krupinski EA, Relyea-Chew A, ChewFS. Methodology and application of clinical trialsin radiology: self-assessment module. AJR Am JRoentgenol. 2008 Mar;190(3 Suppl):S23-8.
Black WC, Aberle DR, Berg CD. Large field trialfor lung cancer screening: putting the wrong cartbefore the horse? Radiology. 2007 May; 243(2):314-316; discussion 317-318.
Black WC, Baron JA. CT screening for lung cancer:spiraling into confusion? JAMA. 2007 Mar;297(9): 995-997.
Black WC. Computed tomography screening forlung cancer: review of screening principles andupdate on current status. Cancer. 2007 Dec;110(11): 2370-84. Review.
Black WC, Czum JM. Screening coronary CTangiography: no time soon. J Am Coll Radiol.2007 May; 4(5): 295-299. Review.
Black WC. Randomized clinical trials for cancerscreening: rationale and design considerationsfor imaging tests. J Clin Oncol 2006;24(20):3252-3260. Review.
Lacy BE, Weiser K, Chertoff J, et al. TheDiagnosis of Gastroesophageal Reflux Disease.Am J Med. 2010 May 19. [Epub ahead of print]
Mainiero MB, Davis LP, Chertoff J. Resident dutyhour limits: recommendations by the IOM andthe response from the radiology community. JAm Coll Radiol. 2010 Jan;7(1): 56-60.
Chertoff J. Imaging of the abdomen. SeminRoentgenol. 2009 Oct;44(4):217.
Chertoff J. Leadership Lesson: The Art ofSuccessful Nominations. Faculty Vitae onAdvancing Women's Leadership. Acad Med. April2009.
Chertoff J, Pisano E, Gert B. Core curriculum:research ethics for radiology residents. AcadRadiol. 2009 Jan;16(1):108-16.
Chertoff J. Competency assessment in resident education. Acad Radiol 2008 Oct;15(10):1215-1216.
Gardner TB, Olenec CA, Chertoff J, et al.Hemoconcentration and pancreatic necrosis: further defining the relationship. Pancreas 2006;33(2):169-173.
Cheung Y, Perrich KD*, Gui J, Koval KJ,Goodwin DW. MRI of isolated distal fibular fractures with widened medial clear space onstressed radiographs: which ligaments are interrupted? AJR Am J Roentgenol. 2009Jan;192(1):W7-12.
Koval KJ, Egol KA, Cheung Y, Goodwin DW,Spratt KF. Does a positive ankle stress test indicate the need for operative treatment afterlateral malleolus fracture? A preliminary report. J Orthop Trauma. 2007; 2(7): 449-455.
Mancuso MA*, Cheung Y, Silas AM, Chertoff JD,Dickey KW. Case 120: ischemic colitis limited tothe cecum. Radiology. 2007; 244(3): 919-1022.
Cheung Y, Doyley M, et al. (Paulsen KD,Weaver JB). Magnetic resonance elastographyof the plantar fat pads: preliminary study in diabetic patients and asymptomatic volunteers. J Comput Assist Tomogr. 2006;30(2):321-326.
Cheung Y, Naspinsky SR*, Goodwin DW, et al.Increased radiodensity of the proximal pole ofthe scaphoid: a common finding in computedtomography imaging of the wrist. J ComputAssist Tomogr. 2006; 30(5):850-857.
Cheung Y, Rosenberg ZS. Soft tissue injury tothe ankle: ligaments. In: Pope T, Bloem H, et al,eds. Imaging of the Musculoskeletal System.Elsevier, 2008. (book chapter)
Zarovnaya EL, Ball PA, Cromwell LD, et al.Atypical Teratoid Rhabdoid Tumor of the Spine inan Adult: Case Report and Review of the Literature.Journal of Neuro-Oncology. 2007 Aug; 84 (1): 49-55.
Czum JM. Evidence-based methodology forevaluation of coronary computed tomographicangiography: reflecting on a self-directed learningexperience. Semin Roentgenol. 2009Jul;44(3):201-8.
Czum JM. Coronary CT angiography for coronaryartery stenosis: a critically appraised topic. SeminRoentgenol. 2009 Jul;44(3):188-90.
Wu N, Gamsu G, Czum J, et al. Detection of small pulmonary nodules using direct digital radiography and picture archiving and communication systems. J Thorac Imaging. 2006Mar;21(1):27-31.
Maddox PT, Paydarfar JA, Black CC, Eskey CJ.Pathology quiz case 1. Basal cell adenocarcinoma(BCAC) of a minor salivary gland. Arch OtolaryngolHead Neck Surg. 2010 Mar;136(3):310, 312-3.
Stein JM, Eskey CJ, Mamourian AC. Mass Effectin the Thoracic Spine from Remnant Bone Wax:An MR Imaging Pitfall. Am J Neuroradiol. 2009Nov 12. [Epub ahead of print]
Farsad K, Mamourian AC, Eskey CJ, FriedmanJA. Computed tomographic angiography as anadjunct to digital subtraction angiography for thepre-operative assessment of cerebral aneurysms.Open Neurol J. 2009 Jan 28;3:1-7.
Fadul CE, Kingman LS, et al. (Eskey CJ). A phaseII study of thalidomide and irinotecan for treatmentof glioblastoma multiforme. J Neurooncol. 2008;90(2): 229-235.
Missios S, Quebada PB, et al. (Eskey CJ). Quick-brain magnetic resonance imaging fornonhydrocephalus indications. J NeurosurgPediatrics. 2008; 2(6): 438-444.
Nogueira RG, Dabus G, Rabinov JD, Eskey CJ, et al. Preliminary experience with onyxembolization for the treatment of intracranialdural arteriovenous fistulas. Am J Neuroradiol.2008; 29(1): 91-97.
Grosberg BM, Farinhas J, Kazmi M, Cohen JA,Eskey CJ. Teaching case: inflammatoryheadache. Headache. 2007; 47(6): 945-947.
Barrocas AM, Eskey CJ, Hirsch JA. Vertebral augmentation in osteoporotic fractures. Injury.2007; 38 Suppl 3:S88-96. Review.
Reddy NJ, Lewis LD, Gardner TB, Osterling W,Eskey CJ, Nierenberg DW. Two Cases of RapidOnset Parkinson’s Syndrome Following ToxicIngestion of Ethylene Glycol and Methanol. ClinPharmacol Ther. 2007;81: 114-121.
Mamourian AC, Pluta DJ, Eskey CJ, Merlis AL.Optimizing computed tomography to reduce artifacts from titanium aneurysm clips: an in vitrostudy. Technical note. J Neurosurg. 2007; 107(6):1238-1243.
Duhaime AC, Saykin AJ, et al. (Eskey CJ).Functional magnetic resonance imaging of theprimary somatosensory cortex in piglets. JNeurosurg .2006; 104(4 Suppl):259-264.
Tong SC, Eskey CJ, et al. Kyphoplasty: a single institution’s initial experience. J Vasc IntervRadiol. 2006; 17(6):1025-1030.
Fadul CE, Kominsky AL, et al. (Eskey CJ).Simmons NE. Long-term response of pituitarycarcinoma to temozolomide. Report of twocases. J Neurosurg. 2006; 105:621-626.

49DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
Yoo AJ, Eskey CJ, Hirsch JA. Vertebral heightrestoration in image-guided interventions. In: Mauro MA, et al., eds. Image-GuidedIntervention, vol 2. Elsevier, 2008. (book chapter)
Eskey CJ, Hirsch JA. Vertebroplasty and kyphoplasty. In: Manchikanti L, Singh V, eds.Interventional Techniques in Chronic Spinal Pain.ASIPP Publishing, 2007. (book chapter)
Eskey CJ. Vertebroplasty and kyphoplasty. In: Schmidek, HH and Roberts DW, eds. OperativeNeurosurgical Techniques: Indications, Methods, andResults, 5th ed. Elsevier, 2006. (book chapter)
Hardman RL, Forauer AR, et al. Uterine arteryembolization for menorrhagia. J Support Oncol.2009 Jan-Feb;7(1):47-50.
Forauer AR, McNulty NJ, Kaneko TM. Tunneledhemodialysis catheter outcomes in elderlypatients. J Vasc Interv Radiol. 2009 Apr;20(4):467-71.
Forauer AR, Hoffer EK, Homa K. Dialysis access venous stenoses: treatment with balloonangioplasty—1- versus 3-minute inflation times.Radiology. 2008; 249(1): 375-381.
Forauer AR, Kent E, Cwikiel W, Esper P, RedmanB. Selective palliative transcatheter embolizationof bony metastases from renal cell carcinoma.Acta Oncol. 2007; 46(7): 1012-1018.
Forauer AR. Pericardial tamponade in patientswith central venous catheters. J Infus Nurs. 2007;30(3):161-167. Review.
Reilley MJ, Forauer AR. Abnormally superiorcourse of the right subclavian artery. J Vasc IntervRadiol. 2007; 18(12): 1602-1604.
Forauer AR, Theoharis CG, Daskia NL. Jugularvein catheter placement: histologic features anddevelopment of catheter-related (fibrin) sheaths ina swine model. Radiology. 2006; 240(2):427-434.
Hughes M, Forauer AR, Lindh M, Cwikiel W.Conformation of adjacent self-expanding stents: across-sectional in vitro study. Cardiovasc InterventRadiol. 2006; 29(2):255-259.
Benz BK, Gemery JM, McIntyre JJ, Eskey CJ.Value of immediate preprocedure magnetic resonance imaging in patients scheduled toundergo vertebroplasty or kyphoplasty. Spine.2009;34(6):609-12.
Rhodes ES, Pekala JS, Gemery JM, Dickey KW.Case 129: Polyarteritis nodosa. Radiology. 2008;246(1): 322-326.
Gemery JM, Nangia AJ, Mamourian AC, Reid SK.Digital three-dimensional modeling of the malepelvis and bicycle seats: impact of rider positionand seat design on potential penile hypoxia anderectile dysfunction. British Journal of Urology BJUInt. 2007 Jan; 99(1):135-140.
Sedlacek M, Gemery JM, et al. Aspirin treatment is associated with a significantlydecreased risk of Staphylococcus aureus bacteremia in hemodialysis patients with tunneled catheters. Am J Kidney Dis. 2007 Mar;49(3):401-408.
Gemery JM. Why I won’t be getting off the interventional radiology tour [letter]. AJR Am JRoentgenol. 2006 Feb;186(2):584.
Sherif C, Gruber A, Bavinzski G, Standhardt H,Widhalm G, Gibson D*, Richling B, Knosp E.Long-term outcome of a multidisciplinary conceptof spinal dural arteriovenous fistulae treatment.Neuroradiology. 2008 Jan;50(1): 67-74.
Sherif C, Dorfer C, Kalteis K, Thun C, Kaiser I,Gibson D*, Alesch F. Deep brain pulse-generatorand lead-extensions: subjective sensations relatedto measured parameters. Movement Disorders.2008 May 15;23(7):1036-40.
Gimi B, Kwon J, et al. Cell encapsulation and oxygenation in nanoporous microcontainers.Biomed Microdevices. 2009 Dec;11(6):1205-12.
Rollins NK, Vachha B, Srinivasan P, Chia J, PickeringJ, Hughes CW, Gimi B. Simple developmentaldyslexia in children: alterations in diffusion-tensormetrics of white matter tracts at 3 T. Radiology.2009 Jun;251(3):882-91.
Gimi B, Kwon J, et al. A nanoporous, transparentmicrocontainer for encapsulated islet therapy. JDiabetes Sci Technol. 2009;3(2):297-303.
Kwon J, Trivedi K, et al. (Gimi B). SU-8-basedimmunoisolative microcontainer with nanoslotsdefined by nanoimprint lithography. J Vac SciTechnol B Microelectron Nanometer StructProcess Meas Phenom. 2009;27(6):2795-2800.
Song H, Shahverdi K, et al. (Gimi B). An immunotolerant HER-2/neu transgenic mousemodel of metastatic breast cancer. Clin CancerRes. 2008 Oct 1;14(19):6116-24.
Patel B, Gimi B, Vachha B, Agadi S, Koral K. Opticnerve and chiasm enlargement in a case of infantile Krabbe disease: quantitative comparisonwith 26 age-matched controls. Pediatr Radiol.2008 Jun;38(6):697-9.
Mikhaylova M, Mori N, Wildes FB, Walczak P, Gimi B, Bhujwalla ZM. Hypoxia increases breastcancer cell-induced lymphatic endothelial cellmigration. Neoplasia. 2008 Apr;10(4):380-9.
Koral K, Gargan L, Bowers DC, Gimi B, et al.Imaging characteristics of atypical teratoid-rhabdoidtumor in children compared with medulloblastoma.AJR Am J Roentgenol. 2008 Mar;190(3):809-14.
Koral K, Kedzierski RM, Gimi B, Gomez A, RollinsNK. Subependymoma of the cerebellopontineangle and prepontine cistern in a 15-year-old adolescent boy. AJNR Am J Neuroradiol. 2008Jan;29(1):190-1.
Gimi B, Artemov D, et al. MRI of regular-shapedcell-encapsulating polyhedral microcontainers.Magn Reson Med. 2007 Dec;58(6):1283-7. PubMedPMID: 17969063.
Vogel-Claussen J, Gimi B, Artemov D, BhujwallaZM. Diffusion-weighted and macromolecular contrast enhanced MRI of tumor response to antivascular therapy with ZD6126. Cancer BiolTher. 2007 Sep;6(9):1469-75. Epub 2007 Jun 27.
Ackerstaff E, Gimi B, Artemov D, Bhujwalla ZM.Anti-inflammatory agent indomethacin reducesinvasion and alters metabolism in a human breastcancer cell line. Neoplasia. 2007 Mar;9(3):222-35.
Gimi B, Artemov D, et al. Cell viability and noninvasive in vivo MRI tracking of 3D cell encapsulatingself-assembled microcontainers.Cell Transplant. 2007;16(4):403-8.
Perrich K*, Goodwin D, Hecht P, Cheung Y. AnkleLigaments on MRI: Appearance of Normal andInjured Ligaments. Am. J. Roentgenol. 2009Sep;193: 687 - 695.
Grinberg OY, Williams BB, et al. (Swartz HM).Oxygen effects on the EPR signals from woodcharcoals: experimental results and the development of a model. J Phys Chem B. 2007Nov;111(46):13316-24.
Grinberg OY, Hou H, Roche MA, et al (Swartz HM, Dunn JF). Modeling of the responseof ptO2 in rat brain to changes in physiologicalparameters. In: Okunieff P, Williams J, eds. OxygenTransport to Tissue, vol 26 (2006). New York: PlenumPublishers. (book chapter)
Grinberg OY, et al. (Swartz HM). Axial oxygendiffusion in the krogh model: modifications to account for myocardial oxygen tension in isolated perfused rat hearts measured by EPRoximetry. In: Okunieff P, Williams J, eds. OxygenTransport to Tissue, vol 26 (2006). New York: PlenumPublishers. (book chapter)
Harris RD, Marks WM. Compact ultrasound forimproving maternal and perinatal care in low-resource settings: Review of the potential benefits,implementation challenges, and public healthissues. J Ultrasound Med. 2009;28(8):1067-76.
Schwaab T, Schwarzer A, et al. (Harris RD).Clinical and immunologic effects of intranodalautologous tumor lysate-dendritic cell vaccinewith Aldesleukin (Interleukin 2) and IFN-{alpha}2atherapy in metastatic renal cell carcinomapatients. Clin Cancer Res. 2009 Aug 1;15(15):4986-92.
Ernstoff MS, Crocenzi TS, et al. (Harris RD).Developing a rational tumor vaccine therapy forrenal cell carcinoma: immune yin and yang. ClinCancer Res. 2007 Jan 15;13(2 Pt 2):733s-740s.
Popov V, Popov D, Kacar I, Harris RD. The feasibility of real-time transmission of sonographic images from a remote location overlow-bandwidth Internet links: a pilot study. AJR AmJ Roentgenol. 2007 Mar;188(3):W219-22.
Pyke J, Hart M, Popov V, Harris RD, McGrath S. Atele-ultrasound system for real-time medicalimaging in resource-limited settings. Conf ProcIEEE Eng Med Biol Soc. 2007; 3094-309.
Harris RD. Arguments for universal healthaccess in the United States: a radiologist’s perspective. AJR Am J Roentgenol. 2007Mar;188(3):617-618.
Schwaab T, Tretter CP, et al. (Harris RD). Tumor-related immunity in prostate cancer patientstreated with human recombinant granulocytemonocyte-colony stimulating factor (GM-CSF).Prostate. 2006 May 1;66(6):667-74.
Harris RD, Couto C, et al. The chorionic bump: afirst-trimester pregnancy sonographic findingassociated with a guarded prognosis. J UltrasoundMed. 2006; 25(6):757-763.
Hoffer EK, Krohmer SJ, Gemery JM, et al.Endovascular recanalization of symptomatic portomesenteric venous obstruction after pancreaticoduodenectomy and radiation. J VascInterv Radiol. 2009;20(12):1633-7.
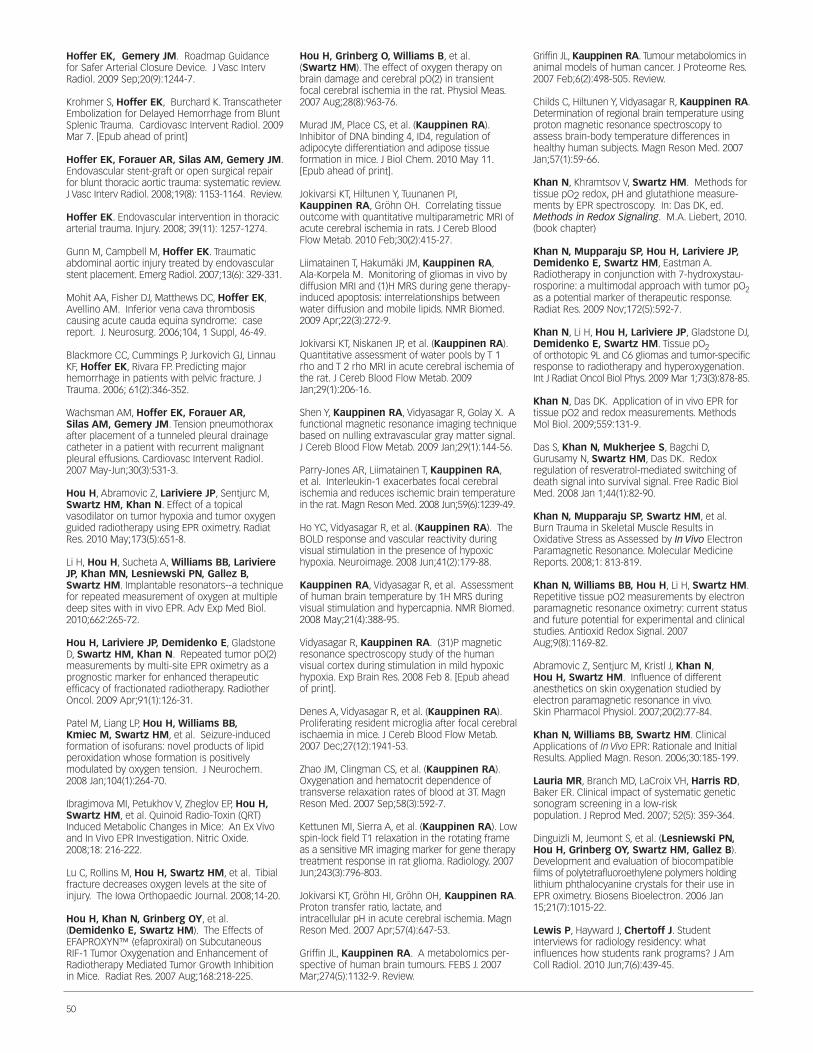
50
Hoffer EK, Gemery JM. Roadmap Guidancefor Safer Arterial Closure Device. J Vasc IntervRadiol. 2009 Sep;20(9):1244-7.
Krohmer S, Hoffer EK, Burchard K. TranscatheterEmbolization for Delayed Hemorrhage from BluntSplenic Trauma. Cardiovasc Intervent Radiol. 2009Mar 7. [Epub ahead of print]
Hoffer EK, Forauer AR, Silas AM, Gemery JM.Endovascular stent-graft or open surgical repairfor blunt thoracic aortic trauma: systematic review.J Vasc Interv Radiol. 2008;19(8): 1153-1164. Review.
Hoffer EK. Endovascular intervention in thoracicarterial trauma. Injury. 2008; 39(11): 1257-1274.
Gunn M, Campbell M, Hoffer EK. Traumaticabdominal aortic injury treated by endovascularstent placement. Emerg Radiol. 2007;13(6): 329-331.
Mohit AA, Fisher DJ, Matthews DC, Hoffer EK,Avellino AM. Inferior vena cava thrombosis causing acute cauda equina syndrome: casereport. J. Neurosurg. 2006;104, 1 Suppl, 46-49.
Blackmore CC, Cummings P, Jurkovich GJ, LinnauKF, Hoffer EK, Rivara FP. Predicting major hemorrhage in patients with pelvic fracture. JTrauma. 2006; 61(2):346-352.
Wachsman AM, Hoffer EK, Forauer AR, Silas AM, Gemery JM. Tension pneumothoraxafter placement of a tunneled pleural drainagecatheter in a patient with recurrent malignantpleural effusions. Cardiovasc Intervent Radiol.2007 May-Jun;30(3):531-3.
Hou H, Abramovic Z, Lariviere JP, Sentjurc M,Swartz HM, Khan N. Effect of a topicalvasodilator on tumor hypoxia and tumor oxygenguided radiotherapy using EPR oximetry. RadiatRes. 2010 May;173(5):651-8.
Li H, Hou H, Sucheta A, Williams BB, LariviereJP, Khan MN, Lesniewski PN, Gallez B,Swartz HM. Implantable resonators--a techniquefor repeated measurement of oxygen at multipledeep sites with in vivo EPR. Adv Exp Med Biol.2010;662:265-72.
Hou H, Lariviere JP, Demidenko E, GladstoneD, Swartz HM, Khan N. Repeated tumor pO(2)measurements by multi-site EPR oximetry as aprognostic marker for enhanced therapeutic efficacy of fractionated radiotherapy. RadiotherOncol. 2009 Apr;91(1):126-31.
Patel M, Liang LP, Hou H, Williams BB, Kmiec M, Swartz HM, et al. Seizure-inducedformation of isofurans: novel products of lipid peroxidation whose formation is positively modulated by oxygen tension. J Neurochem.2008 Jan;104(1):264-70.
Ibragimova MI, Petukhov V, Zheglov EP, Hou H,Swartz HM, et al. Quinoid Radio-Toxin (QRT)Induced Metabolic Changes in Mice: An Ex Vivoand In Vivo EPR Investigation. Nitric Oxide.2008;18: 216-222.
Lu C, Rollins M, Hou H, Swartz HM, et al. Tibialfracture decreases oxygen levels at the site ofinjury. The Iowa Orthopaedic Journal. 2008;14-20.
Hou H, Khan N, Grinberg OY, et al.(Demidenko E, Swartz HM). The Effects ofEFAPROXYN™ (efaproxiral) on Subcutaneous RIF-1 Tumor Oxygenation and Enhancement ofRadiotherapy Mediated Tumor Growth Inhibitionin Mice. Radiat Res. 2007 Aug;168:218-225.
Hou H, Grinberg O, Williams B, et al. (Swartz HM). The effect of oxygen therapy onbrain damage and cerebral pO(2) in transientfocal cerebral ischemia in the rat. Physiol Meas.2007 Aug;28(8):963-76.
Murad JM, Place CS, et al. (Kauppinen RA).Inhibitor of DNA binding 4, ID4, regulation ofadipocyte differentiation and adipose tissue formation in mice. J Biol Chem. 2010 May 11.[Epub ahead of print].
Jokivarsi KT, Hiltunen Y, Tuunanen PI, Kauppinen RA, Gröhn OH. Correlating tissueoutcome with quantitative multiparametric MRI ofacute cerebral ischemia in rats. J Cereb BloodFlow Metab. 2010 Feb;30(2):415-27.
Liimatainen T, Hakumäki JM, Kauppinen RA, Ala-Korpela M. Monitoring of gliomas in vivo bydiffusion MRI and (1)H MRS during gene therapy-induced apoptosis: interrelationships betweenwater diffusion and mobile lipids. NMR Biomed.2009 Apr;22(3):272-9.
Jokivarsi KT, Niskanen JP, et al. (Kauppinen RA).Quantitative assessment of water pools by T 1rho and T 2 rho MRI in acute cerebral ischemia ofthe rat. J Cereb Blood Flow Metab. 2009Jan;29(1):206-16.
Shen Y, Kauppinen RA, Vidyasagar R, Golay X. Afunctional magnetic resonance imaging techniquebased on nulling extravascular gray matter signal.J Cereb Blood Flow Metab. 2009 Jan;29(1):144-56.
Parry-Jones AR, Liimatainen T, Kauppinen RA, et al. Interleukin-1 exacerbates focal cerebralischemia and reduces ischemic brain temperaturein the rat. Magn Reson Med. 2008 Jun;59(6):1239-49.
Ho YC, Vidyasagar R, et al. (Kauppinen RA). TheBOLD response and vascular reactivity duringvisual stimulation in the presence of hypoxichypoxia. Neuroimage. 2008 Jun;41(2):179-88.
Kauppinen RA, Vidyasagar R, et al. Assessmentof human brain temperature by 1H MRS duringvisual stimulation and hypercapnia. NMR Biomed.2008 May;21(4):388-95.
Vidyasagar R, Kauppinen RA. (31)P magneticresonance spectroscopy study of the humanvisual cortex during stimulation in mild hypoxichypoxia. Exp Brain Res. 2008 Feb 8. [Epub aheadof print].
Denes A, Vidyasagar R, et al. (Kauppinen RA).Proliferating resident microglia after focal cerebralischaemia in mice. J Cereb Blood Flow Metab.2007 Dec;27(12):1941-53.
Zhao JM, Clingman CS, et al. (Kauppinen RA).Oxygenation and hematocrit dependence oftransverse relaxation rates of blood at 3T. MagnReson Med. 2007 Sep;58(3):592-7.
Kettunen MI, Sierra A, et al. (Kauppinen RA). Lowspin-lock field T1 relaxation in the rotating frameas a sensitive MR imaging marker for gene therapytreatment response in rat glioma. Radiology. 2007Jun;243(3):796-803.
Jokivarsi KT, Gröhn HI, Gröhn OH, Kauppinen RA.Proton transfer ratio, lactate, and intracellular pH in acute cerebral ischemia. MagnReson Med. 2007 Apr;57(4):647-53.
Griffin JL, Kauppinen RA. A metabolomics per-spective of human brain tumours. FEBS J. 2007Mar;274(5):1132-9. Review.
Griffin JL, Kauppinen RA. Tumour metabolomics inanimal models of human cancer. J Proteome Res.2007 Feb;6(2):498-505. Review.
Childs C, Hiltunen Y, Vidyasagar R, Kauppinen RA.Determination of regional brain temperature usingproton magnetic resonance spectroscopy toassess brain-body temperature differences inhealthy human subjects. Magn Reson Med. 2007Jan;57(1):59-66.
Khan N, Khramtsov V, Swartz HM. Methods fortissue pO2 redox, pH and glutathione measure-ments by EPR spectroscopy. In: Das DK, ed.Methods in Redox Signaling. M.A. Liebert, 2010.(book chapter)
Khan N, Mupparaju SP, Hou H, Lariviere JP,Demidenko E, Swartz HM, Eastman A.Radiotherapy in conjunction with 7-hydroxystau-rosporine: a multimodal approach with tumor pO2as a potential marker of therapeutic response.Radiat Res. 2009 Nov;172(5):592-7.
Khan N, Li H, Hou H, Lariviere JP, Gladstone DJ,Demidenko E, Swartz HM. Tissue pO2of orthotopic 9L and C6 gliomas and tumor-specificresponse to radiotherapy and hyperoxygenation.Int J Radiat Oncol Biol Phys. 2009 Mar 1;73(3):878-85.
Khan N, Das DK. Application of in vivo EPR fortissue pO2 and redox measurements. MethodsMol Biol. 2009;559:131-9.
Das S, Khan N, Mukherjee S, Bagchi D,Gurusamy N, Swartz HM, Das DK. Redox regulation of resveratrol-mediated switching ofdeath signal into survival signal. Free Radic BiolMed. 2008 Jan 1;44(1):82-90.
Khan N, Mupparaju SP, Swartz HM, et al. Burn Trauma in Skeletal Muscle Results inOxidative Stress as Assessed by In Vivo ElectronParamagnetic Resonance. Molecular MedicineReports. 2008;1: 813-819.
Khan N, Williams BB, Hou H, Li H, Swartz HM.Repetitive tissue pO2 measurements by electronparamagnetic resonance oximetry: current statusand future potential for experimental and clinicalstudies. Antioxid Redox Signal. 2007Aug;9(8):1169-82.
Abramovic Z, Sentjurc M, Kristl J, Khan N, Hou H, Swartz HM. Influence of different anesthetics on skin oxygenation studied by electron paramagnetic resonance in vivo. Skin Pharmacol Physiol. 2007;20(2):77-84.
Khan N, Williams BB, Swartz HM. ClinicalApplications of In Vivo EPR: Rationale and InitialResults. Applied Magn. Reson. 2006;30:185-199.
Lauria MR, Branch MD, LaCroix VH, Harris RD,Baker ER. Clinical impact of systematic geneticsonogram screening in a low-risk population. J Reprod Med. 2007; 52(5): 359-364.
Dinguizli M, Jeumont S, et al. (Lesniewski PN,Hou H, Grinberg OY, Swartz HM, Gallez B).Development and evaluation of biocompatiblefilms of polytetrafluoroethylene polymers holdinglithium phthalocyanine crystals for their use inEPR oximetry. Biosens Bioelectron. 2006 Jan15;21(7):1015-22.
Lewis P, Hayward J, Chertoff J. Student interviews for radiology residency: what influences how students rank programs? J AmColl Radiol. 2010 Jun;7(6):439-45.
51DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
Schnell A*, Rosenkranz K, Lewis PJ. The role ofbreast MRI in the preoperative evaluation ofpatients with newly diagnosed breast cancer. AmJ Roentgenol. 2009; 192:1438—1444.
Gorechlad JW, McCabe EB, Higgins JH, Likosky DS,Lewis PJ, Rosenkranz KM, Barth RJ Jr. Screeningfor recurrences in patients treated with breast-conserving surgery: is there a role for MRI? AnnSurg Oncol. 2008; 15(6): 1703-1709.
Koff MD, Cohen JA, McIntyre JJ, Carr CF, SitesBD. Severe Brachial Plexopathy following anUltrasound Guided Single Injection Nerve Blockfor total shoulder arthroplasty in a patient withMultiple Sclerosis. Anesthesiology. 2008;108(2):325—8.
McNulty NJ, Perrich KD, Silas AM, Linville RM,Forauer AR. Implantable Subcutaneous VenousAccess Devices-Is Port Fixation Necessary. Areview of 540 cases. Cardiovasc Intervent Radiol.2009 Dec 3 [Epub ahead of print].
Krohmer S*, McNulty NJ, Schned AR. BestCases from the AFIP: Testicular Seminoma withlymph Node Metastases in a Patient with AdultPolycystic Kidney Disease. RadioGraphics. 2009;29, 2177-2183.
Tyson M, French M, McNulty NJ, Lerner L. Acase of severe bladder wall hypertrophy: bladder cancer or sequela of bladder outletobstruction? Can J Urol. 2009 Feb;16(1):4516-8.
McNulty NJ. Reactivation mycobacterium tuberculosis presenting as empyema necessitans55 years following thoracoplasty. Radiology CaseReports, Vol 3, No 3 (2008).http://radiology.casereports.net.
Nicolalde RJ, Gougelet RM, Rea M, Williams BB,Dong R, Kmiec MM, Lesniewski PN, Swartz HM. The view from the trenches: part 2-technical considerations for EPR screening. HealthPhys. 2010 Feb;98(2):128-35.
Pastel DA, Mamourian AC, Duhaime, AC. InternalStructure in Pineal Cysts on High Resolution MRImaging: Not a sign of malignancy. Journal ofNeurosurgery: Pediatrics. 2009; 4(1):81-84.
Roberts DW, Valdés PA, et al. (Paulsen KD).Coregistered fluorescence-enhanced tumorresection of malignant glioma: relationshipsbetween delta-aminolevulinic acid-induced protoporphyrin IX fluorescence, magnetic resonance imaging enhancement, and neuropathological parameters. J Neurosurg. 2010Apr 9. [Epub ahead of print]
Carpenter CM, Rakow-Penner R, et al. (Paulsen KD). Monitoring of hemodynamicchanges induced in the healthy breast throughinspired gas stimuli with MR-guided diffuse opticalimaging. Med Phys. 2010 Apr;37(4):1638-46.
Davis SC, Samkoe KS, et al. (Paulsen KD, PogueBW). MRI-coupled fluorescence tomographyquantifies EGFR activity in brain tumors. AcadRadiol. 2010 Mar;17(3):271-6.
Valdés PA, Samkoe K, O’Hara JA, Roberts DW,Paulsen KD, Pogue BW. Deferoxamine ironchelation increases delta-aminolevulinic acidinduced protoporphyrin IX in xenograft gliomamodel. Photochem Photobiol. 2010 Mar-Apr;86(2):471-5.
Fang Q, Meaney PM, Paulsen KD. Viable Three-Dimensional Medical Microwave Tomography:Theory and Numerical Experiments. IEEE TransAntennas Propag. 2010 Feb 1;58(2):449-458.
Valdés PA, Fan X, Ji S, Harris BT, Paulsen KD,Roberts DW. Estimation of brain deformation forvolumetric image updating in protoporphyrin IX fluorescence-guided resection. Stereotact FunctNeurosurg. 2010;88(1):1-10.
Skourou C, Hoopes PJ, Paulsen KD. Tissue permittivity: a monitor for progressive tissue fibrosis as observed in bystander tissues followingexperimental high dose rate irradiation. Cancer BiolTher. 2009 Dec;8(23):2223-9.
Halter RJ, Schned A, Heaney J, Hartov A, Paulsen KD. Electrical properties of prostatic tissues: I. Single frequency admittivity properties.J Urol. 2009 Oct;182(4):1600-7.
Halter RJ, Schned A, Heaney J, Hartov A, Paulsen KD. Electrical properties of prostatic tissues: II. Spectral admittivity properties. J Urol.2009 Oct;182(4):1608-13.
Srinivasan S, Carpenter C, Pogue BW, Paulsen KD. Optimization of 3-D image-guidednear infrared spectroscopy using boudary element method. Proc IEEE Int Symp BiomedImaging. 2009 Aug 7;2009:1075-1078.
Wells WA, Wang X, Daghlian CP, Paulsen KD,Pogue BW. Phase contrast microscopy analysis ofbreast tissue: differences in benign vs. malignantepithelium and stroma. Anal Quant Cytol Histol.2009 Aug;31(4):197-207.
Ji S, Roberts DW, Hartov A, Paulsen KD. Brain-skull contact boundary conditions in an inversecomputational deformation model. Med ImageAnal. 2009 Aug;13(4):659-72.
Li Z, Krishnaswamy V, Davis SC, Srinivasan S,Paulsen KD, Pogue BW. Video-rate near infraredtomography to image pulsatile absorption properties in thick tissue. Opt Express. 2009 Jul6;17(14):12043-56.
Borsic A, Halter R, Wan Y, Hartov A, Paulsen KD.Sensitivity study and optimization of a 3D electricimpedance tomography prostate probe. PhysiolMeas. 2009 Jun;30(6):S1-18.
Halter RJ, Zhou T, Meaney PM, et al. (Paulsen KD).The correlation of in vivo and ex vivo tissuedielectric properties to validate electromagneticbreast imaging: initial clinical experience. PhysiolMeas. 2009 Jun;30(6):S121-36.
Davis SC, Pogue BW, Tuttle SB, Dehghani H,Paulsen KD. Spectral distortion in diffuse molecular luminescence tomography in turbidmedia. J Appl Phys. 2009 May 15;105(10):102024.
Davis SC, Pogue BW, Dehghani H, Paulsen KD.Tissue drug concentration determines whetherfluorescence or absorption measurements aremore sensitive in diffuse optical tomography ofexogenous contrast agents. Appl Opt. 2009 Apr1;48(10):D262-72.
Wang J, Jiang S, Paulsen KD, Pogue BW.Broadband frequency-domain near-infrared spec-tral tomography using a mode-locked Ti:sapphirelaser. Appl Opt. 2009 Apr 1;48(10):D198-207.
Jiang S, Pogue BW, Laughney AM, Kogel CA,Paulsen KD. Measurement of pressure-displace-ment kinetics of hemoglobin in normal breast tissue with near-infrared spectral imaging. ApplOpt. 2009 Apr 1;48(10):D130-6
Schegerin M, Tosteson AN, Kaufman PA, Paulsen KD, Pogue BW. Prognostic imaging in neoadjuvant chemotherapy of locally-advancedbreast cancer should be cost-effective. BreastCancer Res Treat. 2009 Apr;114(3):537-47.
Skourou C, Hoopes PJ, Gibbs-Strauss SL,Gladstone DJ, Strawbridge R, Paulsen KD. Highdose rate radiation treatment of experimentalintramuscular prostate carcinoma. Int J Radiat Biol.2009 Apr;85(4):330-7.
Srinivasan S, Carpenter C, Pogue BW, Paulsen KD. Image-guided near infrared spec-troscopy using boundary element method: phan-tom validation. Proc Soc Photo Opt Instrum Eng.2009 Feb 20;7171:717103.
Liu F, Lollis SS, Ji S, Paulsen KD, Hartov A, RobertsDW. Model-based estimation of ventricular deformation in the cat brain. Med Image ComputComput Assist Interv. 2009;12(Pt 2):308-15.
Ji S, Roberts DW, Hartov A, Paulsen KD.Combining multiple true 3D ultrasound image volumes through re-registration and rasterization. Med Image Comput Comput AssistInterv. 2009;12(Pt 1):795-802.
Meaney PM, Zhou T, Fanning MW, Geimer SD,Paulsen KD. Microwave thermal imaging ofscanned focused ultrasound heating: phantomresults. Int J Hyperthermia. 2008 Nov;24(7):523-36.
Carpenter CM, Srinivasan S, Pogue BW, Paulsen KD. Methodology development forthree-dimensional MR-guided near infrared spectroscopy of breast tumors. Opt Express. 2008 Oct 27;16(22):17903-14.
Ji S, Wu Z, Hartov A, Roberts DW, Paulsen KD.Mutual-information-based image to patient re-registration using intraoperative ultrasound inimage-guided neurosurgery. Med Phys. 2008Oct;35(10):4612-24.
Dehghani H, Eames ME, et al. (Paulsen KD).Near infrared optical tomography using NIRFAST:Algorithm for numerical model and image reconstruction. Commun Numer Methods Eng.2008 Aug 15;25(6):711-732.
Wang J, Davis SC, et al. (Paulsen KD). Spectraltomography with diffuse near-infrared light: inclusion of broadband frequency domain spectraldata. J Biomed Opt. 2008 Jul-Aug;13(4):041305
Kepshire D, Davis SC, Dehghani H, Paulsen KD,Pogue BW. Fluorescence tomography characteri-zation for sub-surface imaging with protopor-phyrin IX. Opt Express. 2008 Jun 9;16(12):8581-93.
Tromberg BJ, Pogue BW, Paulsen KD, et al.Assessing the future of diffuse optical imagingtechnologies for breast cancer management. MedPhys. 2008 Jun;35(6):2443-51.
Halter RJ, Hartov A, Paulsen KD, Schned A,Heaney J. Genetic and least squares algorithmsfor estimating spectral EIS parameters of prostatic tissues. Physiol Meas. 2008Jun;29(6):S111-23.

52
Yalavarthy PK, Lynch DR, Pogue BW, Dehghani H,Paulsen KD. Implementation of a computationallyefficient least-squares algorithm for highly under-determined three-dimensional diffuse opticaltomography problems. Med Phys. 2008May;35(5):1682-97.
Halter RJ, Schned A, et al. (Paulsen KD). Electricalimpedance spectroscopy of benign and malignantprostatic tissues. J Urol. 2008 Apr;179(4):1580-6.
Hartov A, Roberts DW, Paulsen KD. A comparative analysis of coregistered ultrasoundand magnetic resonance imaging in neurosurgery.Neurosurgery. 2008 Mar;62(3 Suppl 1):91-9; discussion 99-101.
Halter RJ, Hartov A, Paulsen KD. A broadbandhigh-frequency electrical impedance tomographysystem for breast imaging. IEEE Trans Biomed Eng.2008 Feb;55(2 Pt 1):650-9.
Halter RJ, Hartov A, Paulsen KD. Imaging forearm blood flow with pulse-ox gated electrical impedance tomography. Conf Proc IEEEEng Med Biol Soc. 2008;2008:1192-5.
Borsic A, Hartov A, Paulsen KD, Manwaring P. 3D electric impedance tomography reconstructionon multi-core computing platforms. Conf ProcIEEE Eng Med Biol Soc. 2008;2008:1175-7.
Fox CJ, Meaney PM, et al. (Paulsen KD).Characterization of an Implicitly Resistively-Loaded Monopole Antenna in Lossy Liquid Media.Int J Antennas Propag. 2008;2008:580782.
Song X, Pogue BW, Dehghani H, Jiang S, Paulsen KD, Tosteson TD. Receiver operatingcharacteristic and location analysis of simulatednear-infrared tomography images. J Biomed Opt.2007 Sep-Oct;12(5):054013.
Halter RJ, Hartov A, Heaney JA, Paulsen KD,Schned AR. Electrical impedance spectroscopy ofthe human prostate. IEEE Trans Biomed Eng. 2007Jul;54(7):1321-7.
Halter RJ, Hartov A, Paulsen KD. Experimentaljustification for using 3D conductivity reconstructions in electrical impedance tomography. Physiol Meas. 2007 Jul;28(7):S115-27.
Yalavarthy PK, Pogue BW, et al. (Paulsen KD).Structural information within regularization matrices improves near infrared diffuse opticaltomography. Opt Express. 2007 Jun25;15(13):8043-58.
Meaney PM, Raynolds T, Potwin L, Paulsen KD.3-Point support mechanical steering system for high intensity focused ultrasound.Phys Med Biol. 2007 Jun 7;52(11):3045-56.
Yalavarthy PK, Pogue BW, Dehghani H, Paulsen KD. Weight-matrix structured regularization provides optimal generalized least-squares estimate in diffuse optical tomography. Med Phys. 2007 Jun;34(6):2085-98.
Meaney PM, Fang Q, Rubaek T, Demidenko E,Paulsen KD. Log transformation benefits parameter estimation in microwave tomographicimaging. Med Phys. 2007 Jun;34(6):2014-23.
Carpenter CM, Pogue BW, et al. (Paulsen KD,Weaver JB, Poplack SP, Kaufman PA). Image-guided optical spectroscopy provides molecular-specific information in vivo: MRI-guidedspectroscopy of breast cancer hemoglobin, water,and scatterer size. Opt Lett. 2007 Apr 15;32(8):933-5.
Davis SC, Dehghani H, et al. (Paulsen KD).Image-guided diffuse optical fluorescence tomography implemented with Laplacian-typeregularization. Opt Express. 2007 Apr 2;15(7):4066-82.
Kepshire DS, Davis SC, Dehghani H, Paulsen KD,Pogue BW. Subsurface diffuse optical tomogra-phy can localize absorber and fluorescent objectsbut recovered image sensitivity is nonlinear withdepth. Appl Opt. 2007 Apr 1;46(10):1669-78.
Skourou C, Rohr A, Hoopes PJ, Paulsen KD. In vivo EIS characterization of tumour tissue properties is dominated by excess extracellularfluid. Phys Med Biol. 2007 Jan 21;52(2):347-63.
Jiang S, Pogue BW, Carpenter CM, Poplack SP, etal. (Paulsen KD, Kaufman PA). Evaluation ofbreast tumor response to neoadjuvantchemotherapy with tomographic diffuse opticalspectroscopy: case studies of tumor region-of-interest changes. Radiology. 2009 Aug;252(2):551-60.
Poplack SP, Tosteson TD, et al. (Paulsen KD).Electromagnetic breast imaging: results of a pilot study in women with abnormal mammograms. Radiology. 2007 May;243(2):350-9.
Meaney PM, Fanning MW, Raynolds T, Fox CJ, FangQ, Kogel CA, Poplack SP, Paulsen KD. Initialclinical experience with microwave breast imaging in women with normal mammography.Academic Radiology. 14(2):207-18, 2007 Feb.
Poplack SP, Tosteson TD, Kogel CA, Nagy HM.Digital breast tomosynthesis: initial experience in 98 women with abnormal digital screeningmammography. Am J Roentgenol. 2007; 189(3):616-623.
Srinivasan S, Pogue BW, Carpenter C, Jiang S, WellsWA, Poplack SP, Kaufman PA, Paulsen KD.Developments in quantitative oxygen-saturationimaging of breast tissue in vivo using multispectralnear-infrared tomography. Antioxid Redox Signal.2007 Aug;9(8):1143-56.
Goodrich ME, Greene MA, Eliassen MS, Poplack SP, Wells WA, Carney PA. A Population-based Mammography Registry: How Complete isits Capture? Journal of Registry Management.2006;33(1):3-9.
Srinivasan S, Pogue BW, et al. (Poplack SP,Paulsen KD). In vivo hemoglobin and water concentrations, oxygen saturation, and scatteringestimates from near-infrared breast tomographyusing spectral reconstruction. Acad Radiol. 2006Feb;13(2):195-202.
Ripple MO, Abajian M, Springett R.Cytochrome c is rapidly reduced in the cytosol after mitochondrial outer membrane permeabilization. Apoptosis. 2010 May;15(5):563-73.
Shin HO, Blietz M, Frericks B, Baus S, Savellano D, Galanski M. Insertion of virtual pulmonary nodules in CT data of the chest: development of a software tool. Eur Radiol. 2006Nov;16(11):2567-74.
Schiepers C, Hoh CK, Nuyts J, Seltzer M, Wu C,Huang SC, Dahlbom M. 1-11C-acetate kinetics ofprostate cancer. J Nucl Med. 2008;49(2): 206-15.
Farley EP*, Siegel A, Forauer A, Seltzer M.Subclavian vein stenosis detected with a GI bleeding scan. Clin Nucl Med. 2008; 33:647-648.
Siegel A, Mancuso M, Seltzer M. The spectrum of positive scan patterns in parathyroidscintigraphy. Clin Nucl Med. 2007;32:770-774.
Siegel A, Alvarado M, et al. Parameters in thePrediction of the Sensitivity of ParathyroidScanning. Clin Nucl Med. 2006 Nov;31:679-682.
Siegel A. Nuclear Medicine—Skeletal. In:Approach to Diagnosis: A Case-Based Imaging Review.American Roentgen Ray Society, 2006. (bookchapter)
Ravi V, Silas AM, Siegel A, Seltzer M.Lymphoma of the superior vena cava detectedwith FDG PET/CT. Clin Nucl Med. 2009Dec;34(12):936-8.
Silas AM, Perrich KD, Hoffer EK, McNulty NJ.Complication rates and outcomes of 536 implantedsubcutaneous chest ports: do rates differ basedon the primary operator’s level of training? AcadRadiol. 2010 Apr;17(4):464-7.
Silas AM. Evaluating the urothelium with CTurography: are we there yet? Semin Roentgenol.2009 Oct;44(4):244-54. Review.
Mazurek PM, Silas AM, Gemery JM.Summation of CT scans during radiofrequencyablation for assessing target lesion coverage. AmJ Roentgenol. 2008; 191(3): 790-792.
Silas AM, Forauer AR, Perrich KD*, Gemery JM. Sclerosis of postoperative lymphoceles: avoidance of prolonged catheterdrainage with use of a fibrin sealant. J Vasc IntervRadiol. 2006 Nov;17(11 Pt 1):1791-1795.
Davis SC, Pogue BW, Springett R, et al. (Paulsen KD). Magnetic resonance-coupled fluorescence tomography scanner for molecularimaging of tissue. Rev Sci Instrum. 2008Jun;79(6):064302.
Springett R, Swartz HM, Measurements ofOxygen In Vivo: Overview and Perspectives onMethods to Measure Oxygen within Cells andTissues. Antioxidants & Redox Signaling.2007;9:1295-1301.
Liu B, Zhu X, Chen CL, et al. (Swartz HM).Opening of the mitoKATP channel and decouplingof mitochondrial complex II and III contribute tothe suppression of myocardial reperfusion hyperoxygenation. Mol Cell Biochem. 2010Apr;337(1-2):25-38.
Swartz HM, Flood AB, Gougelet RM, Rea ME,Nicolalde RJ, Williams BB. A critical assessmentof biodosimetry methods for large-scale incidents.Health Phys. 2010 Feb;98(2):95-108.
Rea ME, Gougelet RM, Nicolalde RJ, Geiling JA,Swartz HM. Proposed triage categories forlarge-scale radiation incidents using high-accuracybiodosimetry methods. Health Phys. 2010Feb;98(2):136-44.

53DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
Suzuki H, Tamukai K, et al. (Swartz HM).Development of a compact electron spin resonance system for measuring ESR signals ofirradiated fingernails. Health Phys. 2010Feb;98(2):318-21.
Meenakshisundaram G, Eteshola E, et al. (Swartz HM). Oxygen sensitivity and biocompat-ibility of an implantable paramagnetic probe forrepeated measurements of tissue oxygenation.Biomed Microdevices. 2009 Aug;11(4):817-26.
Fujii H, Sakata K, et al. (Swartz HM). Tissue oxygenation in a murine SCC VII tumor after X-rayirradiation as determined by EPR spectroscopy.Radiother Oncol. 2008 Mar;86(3):354-60.
Reyes RA, Romanyukha A, et al. (Swartz HM).Electron paramagnetic resonance in human fingernails: the sponge model implication. RadiatEnviron Biophys. 2008 Nov;47(4):515-26.
Swartz HM, Burke G, et al. (Dong R, Grinberg O,Lesniewski P, Kmiec M, Nicolalde RJ, SakataY, Williams BB). In vivo EPR for dosimetry. RadiatMeas. 2007 Jul;42(6-7):1075-1084.
Romanyukha A, Trompier F, et al. (Swartz HM).EPR dosimetry in chemically treated fingernails.Radiat Meas. 2007 Aug;42(6-7):1110-1113.
Trompier F, Kornak L, et al. (Swartz HM).Protocol for emergency EPR dosimetry in fingernails. Radiat Meas. 2007 Aug;42(6-7):1085-1088.
Flood AB, Bhattacharyya S, Nicolalde RJ, Swartz HM. Implementing EPR Dosimetry forLife-Threatening Incidents: Factors BeyondTechnical Performance. Radiat Meas. 2007Jul;42(6-7):1099-1109.
Romanyukha A, Mitchell CA, Schauer DA,Romanyukha L, Swartz HM. Q-band EPR biodosimetry in tooth enamel microsamples: feasibility test and comparison with x-band.Health Phys. 2007 Dec;93(6):631-5.
Swartz HM. On tissue oxygen and hypoxia: aneditorial. Antioxidants & Redox Signaling (ForumIssue) 2007; 9:1111-1113.
Alexander GA, Swartz HM, et al. BiodosEPR-2006 Meeting: Acute Dosimetry ConsensusCommittee Recommendations on BiodosimetryApplicants in Events Involving Uses of Radiationby Terrorists and Radiation Accidents. RadiatMeas. 2007;42:972-996.
Schauer DA, Iwasaki A, Romanyukha A, Swartz HM, Onori S. Electron ParamagneticResonance (EPR) in Medical Dosimetry. RadiatMeas. 2007;41:S117-S123.
Swartz HM, Khan N, Khramtsov VV. Use of electron paramagnetic resonance spectroscopyto evaluate the redox state in vivo. Antioxid RedoxSignal. 2007 Oct;9(10):1757-71. Review.
Greer SE, Pipas JM, Sutton JE, Zaki BI, Tsapakos M, et al. Effect of neoadjuvant therapyon local recurrence after resection of pancreatic adenocarcinoma. J Am Coll Surg.2008Mar;206(3):451-7.
Lollis SS, Mamourian AC, Vaccaro TJ, DuhaimeAC. Programmable CSF Shunt Valves:Radiographic Identification and Interpretation. AmJ Neuroradiol. 2010 Feb 11. [Epub ahead of print]
Levin D, Vaccaro TJ. Interpretation of IntensiveCare Nursery Chest Films and Clinical Outcomes,Retrospective review. Journal of Pediatric CriticalCare, 2009 (in press).
Perriñez PR, Kennedy FE, Van Houten EE, Weaver JB, Paulsen KD. Magnetic resonanceporoelastography: an algorithm for estimating themechanical properties of fluid-saturated soft tissues. IEEE Trans Med Imaging. 2010Mar;29(3):746-55.
Xie B, Weaver JB, Meaney PM, Paulsen KD.Magnetic resonance microwave absorption imaging: feasibility of signal detection. Med Phys.2009 Nov;36(11):5190-7.
Rauwerdink AM, Hansen EW, Weaver JB.Nanoparticle temperature estimation in combined ac and dc magnetic fields. Phys MedBiol. 2009 Oct 7;54(19):L51-5.
Weaver JB, Rauwerdink AM, Hansen EW.Magnetic Nanoparticle Temperature Estimation.Medical Physics. 2009; 36(5): 1822-1829.
Perriñez PR, Kennedy FE, Van Houten EE, Weaver JB, Paulsen KD. Modeling of soft poroelastic tissue in time-harmonic MR elastography. IEEE Trans Biomed Eng. 2009Mar;56(3):598-608.
Wang H, Weaver JB, Doyley MM, Kennedy FE,Paulsen KD. Optimized motion estimation forMRE data with reduced motion encodes. PhysMed Biol. 2008 Apr 21;53(8):2181-96.
Weaver JB, Rauwerdink AM, Sullivan CR, Baker I. Frequency distribution of the nanoparticle magnetization in the presence of astatic as well as a harmonic magnetic field. MedPhys. 2008 May;35(5):1988-94.
Carpenter CM, Pogue BW, et al. (Weaver JB,Poplack SB). Image-guided optical spectroscopyprovides molecular-specific information in vivo:MRI-guided spectroscopy of breast cancer hemoglobin, water, and scatterer size. OpticsLetters 2007; 32(8):933-5.
Mamourian AC, Mahadevan N, et al. (Weaver JB).A metal-polymer hybrid cerebral aneurysm clipprototype: in vitro testing for closing force, slippage, and CT artifact. J Neurosurg.2007;107(6):1198-1204.
Zeng Q, Baker I, et al. (Weaver JB). Fe/Fe oxidenanocomposite particles with large specificabsorption rate for hyperthermia. Applied PhysicsLetters, vol 90, 2007.
Doyley M, Feng Q, Weaver JB, Paulsen KD.Performance analysis of steady-state harmonicelastography. Phys Med Biol. 2007 May21;52(10):2657-74.
Madsen EL, Hobson MA, et al. (Weaver JB).Anthropomorphic breast phantoms for testingelastography systems. Ultrasound Med Biol. 2006Jun;32(6):857-74.
Brooksby B, Pogue BW, et al. (Weaver JB,Poplack SP, Paulsen KD). Imaging breast adipose and fibroglandular tissue molecular signatures by using hybrid MRI-guided near-infrared spectral tomography. Proceedings of theNational Academy of Sciences (PNAS) June 6,2006, 103(23):8828—8833.
Williams BB, Khan N, Zaki B, Hartford A, ErnstoffMS, Swartz HM. Clinical electron paramagneticresonance (EPR) oximetry using India ink. AdvExp Med Biol. 2010;662:149-56.
Pollock JD, Williams BB, Sidabras JW, Grinberg O,Salikhov I, Lesniewski P, Kmiec M, Swartz HM.Surface loop resonator design for in vivo EPRtooth dosimetry using finite element analysis.Health Phys. 2010 Feb;98(2):339-44.
Williams BB, Dong R, Kmiec M, Burke G,Demidenko E, Gladstone D, Nicolalde RJ,Sucheta A, Lesniewski P, Swartz HM.Development of in vivo tooth EPR for individualradiation dose estimation and screening. HealthPhys. 2010 Feb;98(2):327-38.
Williams BB, Li D, et al. Disease-toxicant screenreveals a neuroprotective interaction betweenHuntington’s disease and manganese exposure. JNeurochem. 2010 Jan;112(1):227-37.
Demidenko E, Williams BB, Swartz HM.Radiation dose prediction using data on time toemesis in the case of nuclear terrorism. RadiatRes. 2009 Mar;171(3):310-9.
Wilcox DE, He X, Gui J, Ruuge AE, Li H, Williams BB, Swartz HM. Dosimetry based onEPR spectral analysis of fingernail clippings.Health Phys. 2010 Feb;98(2):309-17.
Williams BB, Sucheta A, Dong R, Sakata Y,Iwasaki A, Burke G, Grinberg O, Lesniewski P,Kmiec M, Swartz HM. ExperimentalProcedures for Sensitive and Reproducible In Situ EPR Tooth Dosimetry. Radiat Meas. 2007Jul;42(6-7):1094-1098.
Williams BB, Hou H, Grinberg OY, DemidenkoE, Swartz HM. High spatial resolution multisiteEPR oximetry of transient focal cerebral ischemiain the rat. Antioxid Redox Signal. 2007Oct;9(10):1691-8.
Demidenko E, Williams BB, Sucheta A, Dong R,Swartz HM. Radiation dose reconstruction fromL-band in vivo EPR spectroscopy of intact teeth:Comparison of methods. Radiat Meas. 2007Jul;42(6-7):1089-1098.

54
A Century of Medical Imaging Leadership
1920191019001890 1930 1940 1950 1
‘03
‘11
‘14
‘22
‘27
‘30
‘34
‘40
‘42
‘46
‘56
‘
‘96
‘93
A Century of Medical Imaging Leadership
1797Dartmouth Medical School,fourth oldest medical school in the U.S is founded by Dr
A Century of Medical Imaging Leadership
Dartmouth Medical School, the l school in
is founded by Dr
A Century of Medical Imaging Leadership
Kodak’s new mechanical film processor develops and dries film
‘56Kodak’s new mechanical film
processor develops and dries film
the U.S., is founded by DrNathan Smith.
‘93
John Bowler (DMS 1917) founds the Hitchcock Clinic, one of the
country’s early multispeciality
is founded by Dr.
‘27John Bowler (DMS 1917) founds the Hitchcock Clinic, one of the
country’s early multispeciality
‘30Leslie Sycamore, first specialty-trained radiologist in northern New England, becomes chief of radiology after studying under George Holmes at Massachusetts General Hospital.
In this era, staff uses the RCA “Snook
processor develops and dries film in 7 minutes, “practically a
processor develops and dries film in 7 minutes, “practically a
miracle” at the time.
‘96First Clinical X-Ray in performed at and Gilman FMcCarthy of Hanoverwrist after a fall while skatingtakes a 20-minute exposure
Mary Hitchcock Memorial Hospital (MHMH) is built by Hirin memory of his wifeMaynard Hitchcock.
First Clinical X-Ray in America is performed at Dartmouth College by Edwin and Gilman Frost. Patient is young Eddie
r,, of Hanover who fractured his wrist after a fall while skating. (X-ray takes a 20-minute exposure.)
Mary Hitchcock Memorial Hospital (MHMH) is built by Hiram Hitchcock in memory of his wife, Mary Maynard Hitchcock.
country’s early multispeciality group practices.
Interrrupterless” X-ray apparatus, which was noisy, smelled of ozone, and threw sparks.
‘34 3500 X-ray exams are done per year.
1890
First Production X-rapparatus is placed at MHMH.
1900 1910
‘03First Production X-ray
apparatus is placed at MHMH.
1920
‘22Harry T. French (DMS 1915) is appointed “Assistant
1930 1940
Harry T. French (DMS 1915) is appointed “Assistant
1950
‘46Hanover native Edward Wells (DMS 1940) becomes the first to complete the new radiology residency program. (Dr. Wells, our first radiology resident, was born attended by Dr. Gilman
apparatus is placed at MHMH.
Arthur B. Meservey (DC 1906) joins physics department at Dartmouth,
takes over X-ray operation and teaches radiologic physics to medical residents
apparatus is placed at MHMH.
‘11Arthur B. Meservey (DC 1906) joins physics department at Dartmouth,
takes over X-ray operation and teaches radiologic physics to medical residents
through the 1950’s.
‘14
Roentgenologist.” French had no specialist training in radiology.
Roentgenologist.” French had no specialist training in
‘42William C. McCarty, trained at Mayo Clinic, joins Dr. Sycamore as the 2nd Radiologist in the department. 9,933 X-ray studies done.
First myelography, arteriography and ventriculography done, jointly with surgeons.
William C. McCarty, trained at Mayo Clinic, joins Dr. Sycamore as the 2nd Radiologist in the department. 9,933 X-ray studies done.
First myelography, arteriography and ventriculography done, jointly with surgeons.
born attended by Dr. Gilman Frost, who presided over the first clinical X-ray in 1895!)
equipment for $1500. Pictures which formerly took 15 minutes can now be
‘14MHMH buys more powerful X-ray
equipment for $1500. Pictures which formerly took 15 minutes can now be
done in a few seconds.
First GI studies with bismuthcontrast agent, first fluoroscopy.
‘40Dr. Sycamore starts the MHMH Radiology Residency program, with one resident per year. Paul C. Briede is the department’s first resident.
Dr. Sycamore starts the MHMH Radiology Residency program, with one resident per year. Paul C. Briede is the department’s

55DARTMOUTH-HITCHCOCK MEDICAL CENTER DEPARTMENT OF RADIOLOGY 2006-2010
1960 1970 1980 1990 2000
‘
‘62
‘64
‘65
‘66
‘70
‘74
‘76
‘68
‘80
‘84
‘90
‘91
‘92
‘93
‘95
‘99
‘97
‘00
‘03
‘04
‘05
‘09
‘10
‘10
Robert Jeffery performs first selective coronary
angiography.
‘70Robert Jeffery performs first
selective coronary angiography.
‘74
New medical center opens. Radiology Department has two fixed 1.5T MR scanners,
3 CT systems, and 3 angio/ IR suites.
William Black, outcomes scientist, jointly recruited by Radiology and CECS/TDI.
‘91New medical center opens. Radiology
Department has two fixed 1.5T MR scanners, 3 CT systems, and 3 angio/ IR suites.
William Black, outcomes scientist, jointly recruited by Radiology and CECS/TDI.
the department will complete more than 250,000
Dr. Cliff Belden starts first clinical functional MRI service in northern New England.
Department staff numbers 275, with 35 clinical radiologists and 8 research radiologists; this year the department will complete more than 250,000
exams and procedures.
‘09
‘10Dr. Cliff Belden starts first clinical
functional MRI service in northern New England.
Department staff numbers 275, with 35 clinical radiologists and 8 research radiologists; this year the department will complete more than 250,000
exams and procedures.
‘66Radiology split into separate sections:
‘68Dr. Sycamore retires. Peter
Spiegel is recruited from Harvard. Percutaneous
angiography initiated in angio lab in OR by Dr. Spiegel.
‘74First ultrasound unit installed, a Picker Gray Scale Scanner, under Harte Crow.
‘76Dr. Spiegel named Radiology Section Chairman. Seven radiologists now on staff.
Radiology installs first whole body CT scanner, gift of the Hubbard family: 1.5 minutes for 2 slices, 6-8 minutes for head,
‘68Dr. Sycamore retires. Peter
Spiegel is recruited from Harvard. Percutaneous
angiography initiated in angio lab in OR by Dr. Spiegel.
First ultrasound unit installed, a Picker Gray Scale Scanner, under
Dr. Spiegel named Radiology Section Chairman. Seven radiologists now on staff.
Radiology installs first whole body CT scanner, gift of the Hubbard family: 1.5 minutes for 2 slices, 6-8 minutes for head,
‘92The department’s first basic science laboratory created—the Electron Paramagnetic
‘92The department’s first basic science laboratory created—the Electron Paramagnetic
Residency program expanded to five per year. Radiology departments
in D-H clinics in southern NH integrated into a single RIS/PACS
with DHMC Radiology.
‘09Residency program expanded to
five per year. Radiology departments in D-H clinics in southern NH
integrated into a single RIS/PACS with DHMC Radiology.
‘64Residency program
expands to two residents per year.
Radiation Oncology, under Frank Lane, MD, and
Diagnostic Radiology, under William McCarty.
2 slices, 6-8 minutes for head, 15-20 minutes for a body.
Residency program expands to three residents per year. 122,885
exams and procedures done.
Begin Cross-Sectional Radiology
2 slices, 6-8 minutes for head, 15-20 minutes for a body.
‘90Radiology becomes a full
DHMC department.
Residency program expands to three residents per year. 122,885
exams and procedures done.
Begin Cross-Sectional Radiology fellowship.
Resonance (EPR) Center, under Harold Swartz.
the Electron Paramagnetic Resonance (EPR) Center, under Harold Swartz.
‘93Biomedical NMR Lab, with 7T small-bore experimental magnet, established by Jeffrey Dunn.
Begin fellowship program in Vascular and Interventional Radiology.
1960
‘65The KelliKet image intensifer introduced. Until now, radiologists using fluoroscopic screens wore red goggles in all normal light even at breakfast at home before work.
1970
‘65The KelliKet image intensifer introduced. Until now, radiologists using fluoroscopic screens wore red goggles in all normal light even at breakfast at home before work.
‘80First balloon angioplasty of leg.
1980 1990
fellowship.
‘95Radiology nursing service
created, driven by rapid expansion of interventional
procedures.
1990 2000
‘95Radiology nursing service
created, driven by rapid expansion of interventional
procedures.
‘97
‘05Cliff Eskey begins interventional neuroradiology service.
‘05Cliff Eskey begins interventional neuroradiology service.
‘62Nuclear imaging initiated by Pathology Department, under Elizabeth French. First cardiac catheterization/ angiography rooom installed in the OR, with modern fluoroscopic intensification, cineflourographic and biplane rapid serial filmchanging equipment. Early procedures were mostly cardiac caths, by cutdown rather than percutaneously.
Nuclear imaging initiated by Pathology Department, under Elizabeth French. First cardiac catheterization/ angiography rooom installed in the OR, with modern fluoroscopic intensification, cineflourographic and biplane rapid serial filmchanging equipment. Early procedures were mostly cardiac caths, by cutdown rather than percutaneously.
First clinical MRI in the department, a 1.0T Siemens
‘84First clinical MRI in the
department, a 1.0T Siemens
Drs. Steven Poplack and Keith Paulsen launch NCI-funded
Alternative Breast Cancer Imaging program: now in its 11th year, the
$15 million study is among the most prominent of its kind anywhere.
Ultrasound becomes totally digital and filmless. DXA bone
mineral screening service
‘99Drs. Steven Poplack and Keith
Paulsen launch NCI-funded Alternative Breast Cancer Imaging program: now in its 11th year, the
$15 million study is among the most prominent of its kind anywhere.
‘97Ultrasound becomes totally
digital and filmless. DXA bone mineral screening service
initiated.
‘03
‘04Neuroradiology fellowship begins.
Acquire experimental tomosynthesis system and begin one of the nation’s first clinical trials comparing DBT with conventional mammography.
Neuroradiology fellowship begins.
Acquire experimental tomosynthesis system and begin one of the nation’s first clinical trials comparing DBT with conventional mammography.
selfshielding unit installed in a prefabricated building adjacent
to Radiology.
selfshielding unit installed in a prefabricated building adjacent
to Radiology.
prominent of its kind anywhere.
Residency program expands to 4 per year.Neurointerventional room with biplane
16/12 intensifier installed.
prominent of its kind anywhere.
‘00Residency program expands to 4 per year.
Neurointerventional room with biplane 16/12 intensifier installed.
‘03Transition to filmless workplace completed as CT and MR are integrated into PACS.
Begin joint program with Lebanon College for training radiographic technologists.
Transition to filmless workplace completed as CT and MR are integrated into PACS.
Begin joint program with Lebanon College for training radiographic technologists.

56
The principal facilities of the DHMC Department of Radiology are located on the third (main) floor of the DHMC Lebanon campus,
as shown above. In addition, the department conducts clinical imaging in the Emergency Department, a DXA suite in the
outpatient wing, and mobile MRI units and an extremity MRI scanner on the second floor. Imaging research labs are located at
Dartmouth Medical School and The Thayer School of Engineering in Hanover, and at several DHMC locations including the
Advanced Imaging Center, the Rubin building and the Borwell Research wing.
DHMC RADIOLOGY FACILITIES
Res
id.
Ad
min
.
CT 4 CT 5
3D
Body RR VIR RR
Angio 4
Angio 3Angio 2
Angio 1
AngioRecovery
ResidentsRoom
RR RR
Rm. 9Rm. 10Chest Rm. 11
PICC
Rm. 8Fluoro Fluoro RR
Rm. 7Fluoro
Rm. 6 Rm. 5Fluoro
Rm. 4Chest
Rm. 3 Rm. 2Stitching
Rm. 1Stitching
PT Holding
RRRICS/PACS
RR
RR
Imaging Center(Film Library)
Student Rm.
Admin. Asst’s
Nuc RR
CT 2
3W(Nuc, CT, MRI)
Nuc 3 StressLab
Nuc 1
Nuc 2
Conference Room
U/S 5 U/S 6
U/S 3 U/S 2 U/S 1
3S(U/S, Mammo)
3T(X-ray, Flouro)
U/S RRU/S 4
Mam
mo
RR
Mam
mo
RR
DX 3
Stereotactic
DX 2 U/S 1 U/S 2
Gla
ss W
all
ED and East Entrance
Food Court
North Mall
MR 1
MR 2
MR 3
Neuro RR
Stairs
Elevators
Mammography
DX Core
Ultrasound
EEG Lab
3V
Vascular Services
LeadershipPreventiveMedicine
PET/CT
Palliative Care
Stairs
Stairs
W
E
N S
Main Entrance
MR 1
3D
CT 4MR 1
Neuro RR
MRI)
CT 2
CT 5 ,TT, C,c,(Nu3W
Nuc 1Lab
Nuc 2
Nuc 3 Stress
ED and East Ent
3V
ance rED and East Ent
MR 2
Angio 4
Body RR
MR 3
Recovery
Angio 4
VIR RRBody RR
Angio
Nuc RR
PET/CT
ascular ServicesVVa
ascular Services
E
Angio 3Stairs
Admin
Angio 3Angio 2
Angio 1
RR
Admin
RR
RR ACS
Room
RR
PRICS/
Residents alliative CareP
9PT Holding
Chest
ACS
Medicine
RICS/
10.Rm.Rm
PreventiveLeadership
PICC 11.Rm
N
E
W
all
all
WWG
lass
Gla
ss
S
Ad
min
.Conference Room
Asst’s
U/S 6U/S 5 Student Rm.
Res
id.
Admin
Mammography
R
Asst’s RR
ary)
Ro
amm
M
RR
oam
mM
.Admin
rrary)(Film LibImaging Center
DX Core
6
Fluoro
Fluoro
Fluoro Chest 3
Fluoro RR
.Rm 4.Rm 5.Rm.Rm
7.Rm
8.Rm
PICC
Stitching Stitching
EEG Lab
1.Rm 2.Rm
s
Elevators
Stairs
srrStaiStai
Ultrasound
U/S 1U/S 2U/S 3
U/S RRU/S 4
DX 2 1
DX 3
(U/S, Mammo) U/S
3S
lal MorthNood CourtF
U/S 2
Stereotactic
Flouro),yy,arra(X-3T
ance rM i E tMain Ent

Dartmouth College, February 3, 1896. Less than a year after German scientist Wilhelm Roentgen describes the penetrating properties of his“mysterious light,” Dartmouth physics assistant Frank Austin builds an X-ray apparatus based on Roentgen’s model. His senior colleague,physics professor Edwin Frost, proposes a medical use for the device,and speaks of it to his brother, Dr. Gilman Frost, Mary Hitchcock HospitalPhysician-in-Chief. Frost’s patient, Eddie McCarthy, is a local fourteen-yearold who has broken his wrist ice-skating. The 20-minute exposure ofEddie’s left wrist made at Dartmouth College this day was the first clinicaluse of X-ray imaging in the U.S.—and possibly the first in the world.
Left to right: physicist Edwin Frost, patient Eddie McCarthy, Dr. Gilman Frost, and Gilman’s wife, Margaret Mead Frost.Photo by H.H. Langill and Henry H. Barrett.Courtesy of Dartmouth College Archives.

ONE MEDICAL CENTER DRIVE, LEBANON, NH 03756 www.DHMC.ORG©2010 Dartmouth-Hitchcock Medical Center