© copyright, the joint commission joint commission center for transforming healthcare (cth)...
TRANSCRIPT

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Joint Commission Center for Transforming Healthcare (CTH)
Partnering for Success in Reducing Surgical Site Infections
Cynosure Health Summit21st May 2012

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Siew Lee Grand-Clément RN, MSN, CPHQ Center Project Leader: Surgical Site Infections CollaborativeJoint Commission Center for Transforming Healthcare (CTH)
2

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Objectives1. To explain the collaborative working model of the Joint
Commission Center for Transforming Healthcare.
2. To describe the problem solving methodology used in reducing Surgical Site Infections.
3. To identify the key stakeholders involved and describe the process of forming an effective multi-disciplinary team.
4. To demonstrate the use of infection control and prevention practices in driving improvements.
5. To illustrate the roles of nursing in process improvement initiative.
3

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
4

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Introduction to CTH-Vision
All people always experience the safest, highest quality, best-value health care across all settings.
One Vision
5

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Why the CTH was Created
Our Mission - Transform health care into a high reliability industry and to ensure patients receive the safest, highest quality care they expect and deserve.
Presents a new approach to address critical safety and quality problems sought by The Joint Commission, health care organizations, patients and their families, physicians and other clinicians, and other public and private stakeholders
6

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
What’s Different About the Center?Unique approach to improvement: Center for Transforming Healthcare (CTH)
collaborating with HCOs and hospital leaders where lean, six sigma are already working
Powerful process improvement tools (RPI) – Underlying causes, targeted solutions
– Integrated change management for acceptance and accountability
Engaging industry coupled with reach of TJC– Leadership Advisory Council Members & Sponsors
– Ability to spread solutions to 19,000+ accredited health care organizations in US
7

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Introduction to CTH-Targeting Root Causes
8

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Introduction to CTH-Projects Project 1 – Hand Hygiene Compliance Project 2 – Wrong Site Surgery Project 3 – Hand Off Communication Project 4 – Surgical Site Infections
– With American College of Surgeons Project 5 – Preventing Avoidable Heart Failure Hospitalizations
– With American College of Physicians Project 6 – Safety Culture Project 7 – Preventing Falls with Injury Project 8 – Reducing Sepsis Mortality Project 9 – Medication Safety
9

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
PROJECT #4: SURGICAL SITE INFECTIONS
Collaborate with American College of Surgeons & NSQIP measurement system leveraged.
Seven participating hospitals:1.Mayo Clinic, MN2.Cleveland Clinic, OH3.Stanford Hospital & Clinics, CA 4.OSF Saint Francis, IL5.Northwestern Memorial Hospital, IL6.North Shore LIJ, NY7.Cedars-Sinai Medical Center, CA
10

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Systematic Approach to Problem Solving
– Surgical Site Infections (1)
11
The Center worked with the American College of Surgeons to determine the scope of the SSI project, since there is a wide range of surgeries and procedures that can develop SSIs – each with its own unique set of complications and challenges.
To help narrow the scope of the project, the following criteria were used to identify a specific procedure that:
Is common across different types of hospitalsHas significant complications with an adverse clinical impactHospitals have significant opportunities to improve performanceHas high variability in performance across hospitals

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Systematic Approach to Problem Solving
– Surgical Site Infections (2)
12
Scope: All patients undergoing colorectal surgery (emergency and elective) regardless of who (i.e., which clinical discipline) performs the surgery. NSQIP CPT codes for colorectal surgery. All types of Surgical Site Infections (Superficial Incisional, Deep Incisional, and Organ/Space). Exclude: Trauma and Transplant patients. Patients under 18 years of age.Process starts: Pre-admission Process ends: 30 days post surgery
Metrics to improve:Defects: Colorectal Surgical Site Infections (SSIs)Goal: Reduce colorectal surgical site infections by 50%.Primary: Observed Rate of Patients with Colorectal SSIs (within 30 days of the procedure)Secondary: Observed over Expected (O/E) Ratio for Colorectal SSIs

Dominique LaRochelle, MHA Project Manager Cleveland Clinic Quality & Patient Safety Institute
13

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Quality and Patient Safety Institute * 14
Cleveland ClinicCleveland Clinic
14

Quality and Patient Safety Institute * 15
Developing Effective Teams…
Who is going to solve this important problem?
15

Patient
Quality and Patient Safety Institute * 16
Complex Environment
Physicians
Unit Secretaries Coders
Case Managers Patient Access
OperationsAdministration
Nurses
How to Align?
16

Quality and Patient Safety Institute * 17
Identifying a Project Team - RACIR A C I
Quality Improvement
Quality Management
Colorectal Services
Perioperative Services
Inpatient Colorectal Services
Pharmacy
Infection Control / Infectious Disease
Environmental Services
Safety / Clinical Risk / Accreditation
Sterile Processing
Data
17

Quality and Patient Safety Institute * 18
Project Team
Who is going to solve this important problem?Sponsor Chief Quality Officer
Champion Surgeon Leader
Process Owner Colorectal Surgery
Black Belt Director of Quality Improvement
Core Team Quality Improvement Project Manager
Quality Management
Peri-operative Services Nurse Managers (Admission & PACU)
Nurse Manager Colorectal Services
OR Nurse Manager Colorectal Services
Wound Care specialist
Infection Prevention
18

Quality and Patient Safety Institute * 19
Project Team Subject Matter Experts:
Stakeholder Represented Area
Quality and Patient Safety Institute
Quality ImprovementQuality ManagementSafetyAccreditation
Clinical Risk ManagementInfection Control / Infectious DiseaseData Resource Management
Colorectal Services Digestive Disease Institute – Administration & Physician LeadershipQuality Review OfficersPre-op: Nursing, Education, Staff, Management, Anesthesia, DietaryPost-op: Nursing, Education, Staff, Management, Wound Care, Dietary
Surgical Operations Administration / Physician LeadershipPACE, PACU, IMPACT clinicsNursing, Staff, Anesthesia
Pharmacy Pharmacists
Environmental Services OR & Inpatient management
Sterile Processing Surgical Tech Management / EducationEquipment Vendors
Data NSQIPARKSNursing Informatics
Medical Records Data / Health Data ServicesBusiness Intelligence (EBI)
19

Quality and Patient Safety Institute * 20
Analysis Strategy
Cause/Effect Analysis
Multi-Vari Analysis
Benchmarking & SMEs
Impact/Effort Analysis
Improvements Validation
20

Quality and Patient Safety Institute * 21
SIPOC Analysis
Met with 3 teams of core team members to map peri-operative process: Pre-, Intra-, Post- Op
Expanded upon SIPOC to explore cause & effect relationships Fishbone Diagram Cause & Effect scale: Numerical score, 1-5, based on process
variable and its relationship to our output; SSI– Subjective findings using area experts– Narrowed the scope to help us focus on a few key processes – Key processes can then be further explored using objective
data
21

SIPOC
22

Quality and Patient Safety Institute * 23
Cause & Effect Analysis
SSI
Patient Health
Materials / Equipment
Environment
Clinical Decision Making
Technique
Pre-op Medications
Pre-Op Pain Mgmt
Central Line
Pre-op Abx
Repeat Abx
Abx Selection
Post-op Abx
Post-op Glucose
Post-op Pain Mgmt
Dressing Change
Post-op Pt Diet/Hydration
Post D/C Follow-up
Post-op Medications
Wound Care Specialist
RN Hours/Patient DayPost-op LOS
Geographic Location (Pt.)
Socio-economic Status
Surgery Location (OR)
OR Humidity
OR Temperature
Surgical Team Consistency
Shift Changes During Surgery
OR traffic
OR Air Filter Maintenance
OR Cleaning Crew
Surgical Fellowship Turnover
Staff Change(s)
PACU Traffic
Post-op Recovery Location
Private v. Semi-Private Recovery Rm
Inpt Unit
EVS
Discharge Location
Inpt Room Traffic
Surgical Equipment
Wound Dressing Material
OR Cleaning Solutions
Wound Care Materials / Equipment
Bed Linen Type
Bed Type
Inpt Rm Cleaning Solutions
Diagnosis / Disease
Comorbidities
Platelet Count
Isolation PatientGlucose levels
Anemia
Diet/Nutrition
BMI
Ethnicity/Culture
Age
Antiseptic Shower/Bath
Pre-op Pt Edu
OR dress code compliance
Surgeon Scrub Technique (HH) Hair Removal
Aseptic Practice / Sterile TechniqueEquip. Sterilization
Intra / Post-op Pt Temp.
Warming Device
Procedure Type – Minor v. Major
Wound Dressing TechniqueOR Cleaning Process
1 Surgeon: Multiple OR’sCombo Surgical Case
Patient hand-off Communication
Post-op Education
Wound Care Technique (HH)
Freq. Bed Linen Change
Inpt. Rm Cleaning
D/C Instructions
23

Cause & Effect Analysis Met with SIPOC teams (area experts) to review recorded processes
and narrow our focus using a rating scale 1-5 (Subjective findings)
24

Quality and Patient Safety Institute * 25
Cause & Effect Analysis Priority processes were identified to help focus the team’s interventions
Processes Identified as Having the Greatest Impact on Risk of SSIProcesses Identified as Having the Greatest Impact on Risk of SSI
Pre- Op Diagnosis / Disease Focus on chronic inflammation
Isolation Patient, Pre-op infectious agent
Glucose Levels
Diet / Nutrition
Antiseptic Shower or Bath
Patient Demographics BMI specifically
Intra- Op Surgeon Scrub Technique (HH)
Aseptic Practice / Sterile technique
Equipment Sterilization Technique
Air Filter Maintenance
Post- Op RN Hours per Patient Day
Wound Care Technique and Materials (Including HH)
OR PACU/ICU, Patient Hand-off Communication
Post-op Glucose Levels
Patient Diet / Nutrition
Post- Op Medications
Wound Care Specialist, CWOCN
25

Quality and Patient Safety Institute * 26
Analysis Strategy
Cause/Effect Analysis
Multi-Vari Analysis
Benchmarking & SMEs
Impact/Effort Analysis
Improvements Validation
26

Quality and Patient Safety Institute * 27
Validating Progress: OR Audits
Detail observations (April – May 2011) Multidisciplinary team Broad scope, low n
Circulating nurse checklist (May – October 2011) Led by circulating nurse Narrow scope – bundle focus High n – intent to capture all eligible cases
27

Quality and Patient Safety Institute * 28
Challenges Encountered
Impacting how surgeons practice
Data are imperfect – Sampling Incomplete process data are available
Resources are limited Data needed to support improvements Improvements need to be made
28

Sasha Madison, MPH, CIC. Sasha Madison, MPH, CIC. ManagerManagerInfection Prevention and Control Department Infection Prevention and Control Department
29
30

Confidential- Protected by California Evidence Code Section 1157
Infection Prevention & ControlInfection Prevention & Control
Role in this Project:
−Subject Matter Expert (SME)
−Core team member
−Prior to this project the role of the Infection Preventionist was focused on surveillance.
Defining cases, abstracting data, calculating rates
Interventions to decrease SSIs were often individual – not system based
31

Confidential- Protected by California Evidence Code Section 1157
Infection Prevention & ControlInfection Prevention & Control
Role in this Project: (during project)
−Core team member: “ team participant”
Involved in project in all phases: from Define to Control
−Subject Matter Expert (SME)
Defining different data sources with team and reviewing them, along with the definitions, with the team
NSQIP vs NHSN
− Interventions to decrease SSIs were system based
32
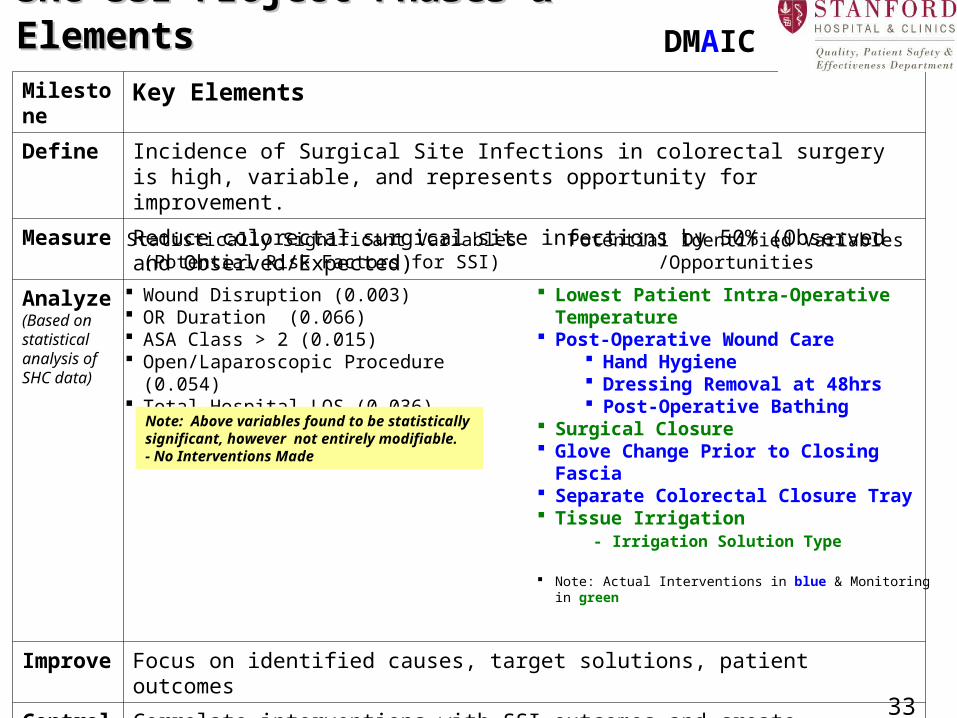
SHC SSI Project Phases & ElementsSHC SSI Project Phases & ElementsMilestone
Key Elements
Define Incidence of Surgical Site Infections in colorectal surgery is high, variable, and represents opportunity for improvement.
Measure
Reduce colorectal surgical site infections by 50% (Observed and Observed/Expected)
Analyze(Based on statistical analysis of SHC data)
Improve
Focus on identified causes, target solutions, patient outcomes
Control Correlate interventions with SSI outcomes and create sustainability plans for any intervention that successfully decreased SSIs
Statistically Significant Variables(Potential Risk Factors for SSI)
Potential Identified Variables /Opportunities
Wound Disruption (0.003) OR Duration (0.066) ASA Class > 2 (0.015) Open/Laparoscopic Procedure (0.054) Total Hospital LOS (0.036)
Lowest Patient Intra-Operative Temperature
Post-Operative Wound Care Hand Hygiene Dressing Removal at 48hrs Post-Operative Bathing
Surgical Closure Glove Change Prior to Closing
Fascia Separate Colorectal Closure Tray Tissue Irrigation - Irrigation Solution Type
Note: Actual Interventions in blue & Monitoring in green
Note: Above variables found to be statistically significant, however not entirely modifiable.- No Interventions Made
33
DMAIC

Confidential- Protected by California Evidence Code Section 1157 34
NHSN Publicly Reported Cases- MIDAS Focus StudyNHSN Publicly Reported Cases- MIDAS Focus Study
MIDAS Focus Objectives:
• Detailed abstraction of elements with identified areas of opportunity
• Data will be analyzed for any potential trends and to serve as a guide for further interventions
• Surgeon specific SSI rates
• Surgical Quality Council Dashboard will include SSI outcomes
Confidential- Protected by California Evidence Code Section 1157
Next Steps & OpportunitiesNext Steps & Opportunities
MIDAS Focus Study on Publicly Reported Cases− Infection Control SSI surveillance in July/Aug 2011 identified an
opportunity in colorectal surgery
− Data collection focused on elements which are not captured elsewhere
− Need for individual physician communication of infections identified
Antibiotic Stewardship− Instituted February 2012
− Review of current prophylaxis guidelines and empiric therapy
Based on best practice learning through collaborative, continue glove changes & separate/clean closing instruments
35

Elisa Nguyen, RN, MS, CMSRN. Elisa Nguyen, RN, MS, CMSRN. Patient Care Manager Patient Care Manager
36

Confidential- Protected by California Evidence Code Section 1157
Role of Nursing
Wound Management
Postoperative Phase
37
Confidential- Protected by California Evidence Code Section 1157
Key stakeholder
− In all processes that involves caring for patients
Nursing involvement from different levels collaborating with the Core Team
− staff nurses
− Unit Educators
− managers
Process improvement
− We own majority of the process
− What are gaps in the process that could be improved
Education and training
− Lead the education and training the frontline nurses 38
Role of NursingRole of Nursing

Confidential- Protected by California Evidence Code Section 1157
Existing Policy and Procedure (P&P)
−No existing one for post-op wound care management
−Utilized another service’s P&P as a model to create one for colorectal
Shared governance approval
−Drafted P&P went to one of the physician lead for review
−Hospital nursing council for final review and approval
39
MD/RN CollaborationMD/RN Collaboration

Confidential- Protected by California Evidence Code Section 1157 40
Post-Operative Wound Management & Post-Operative Wound Management & Surgical Brochure Surgical Brochure DMAIC
Utilizing Surgical Brochure to Reinforce critical need of Post Operative Wound ManagementProtocol

Confidential- Protected by California Evidence Code Section 1157
Unit level staff identified process of implementation
− Unit Clerk – added the audit tool to admission packet, color coded the patient’s name of locator board
− Primary Nurse – completed the audit
− Resource Nurse – double checked that audit was completed
Data collector
− Quality manager in charge of data processing
41
Tracking the ProcessTracking the ProcessNursing Action Focus: Conducted to better understand hand hygiene at each phase of post-op care and to assure that we keep the incisional wound and drain insertion sites free from contamination in the early post-operative period
41

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
What is next?
How can you participate in this effort?
42

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
CTH Operating Model
Project Selection
Create Solutions, Pilot Test, Build Spread
Determine TopicSolve with Participating
Organizations
Pilot Test
Integrate Solutions w/ TST Launch TST
18 to 24 months
43

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Introduction to CTH-Spread
Improvement spread through Targeted Solutions Tool™
– Web-based tool free to Joint Commission accredited organizations
– No knowledge of RPI methodology needed
– Data analysis conducted by the tool, not the user
– Tool walks user through process of:
– Measuring current state
– Determining root causes
– Selecting targeted solutions
– Control of process after implementation
44

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Benefits of becoming a pilot siteAssisting the Center in its aim to transform
health care into a high-reliability industry by solving health care’s most critical safety and quality problems
Access to the Center solutions prior to national release
Access to the tools developed and used by the participating hospitals in the Surgical Site Infections Project
45

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Pilot participant expectations
Webex conference calls occur approximately every 2 weeks throughout pilot
46

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
Feel Free to Contact Us
Any information related to the Joint Commission Center for Transforming Healthcare, the SSI Collaborative Project and Pilot Participation, – Please contact Siew Lee Grand-Clément at
[email protected] – Website:
www.centerfortransforminghealthcare.org
47

© C
opyr
ight
, The
Joi
nt C
omm
issi
on
QUESTIONS OR COMMENTS?
48