© continuing medical implementation …...bridging the care gap target organ damage joel niznick md...
TRANSCRIPT
© Continuing Medical Implementation …...bridging the care gap
Target Organ DamageTarget Organ Damage
Joel Niznick MD FRCPC
© Continuing Medical Implementation …...bridging the care gap
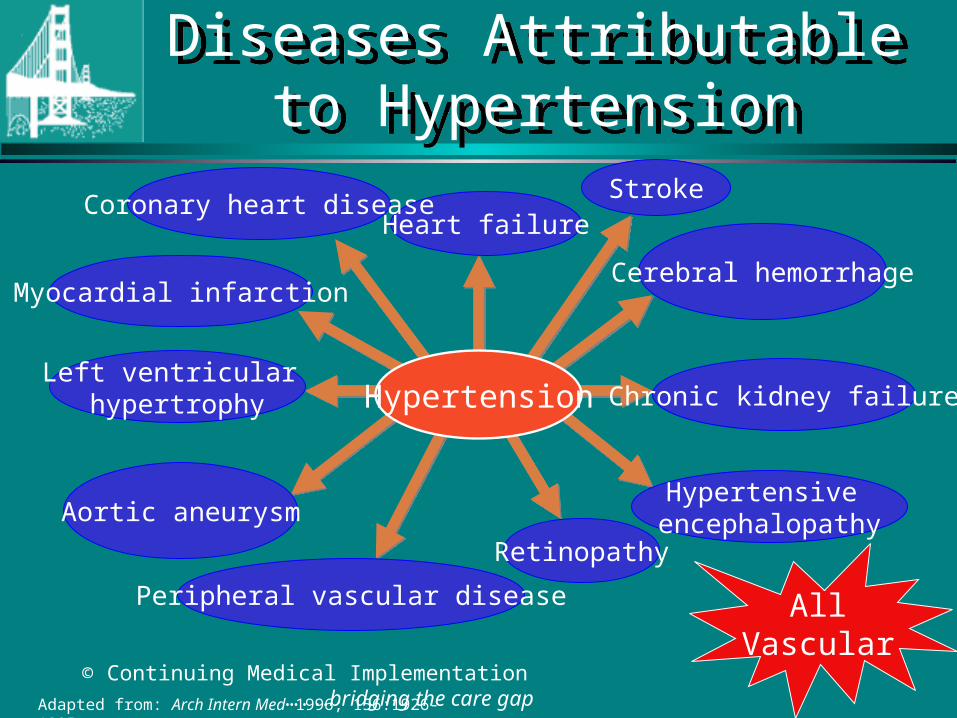
Diseases Attributable to Hypertension
Diseases Attributable to Hypertension
Hypertension
Heart failureStroke
Coronary heart disease
Myocardial infarction
Left ventricular hypertrophy
Aortic aneurysm
Retinopathy
Peripheral vascular disease
Hypertensive encephalopathy
Chronic kidney failure
Cerebral hemorrhage
Adapted from: Arch Intern Med 1996; 156:1926-1935.
AllVascular
© Continuing Medical Implementation …...bridging the care gap
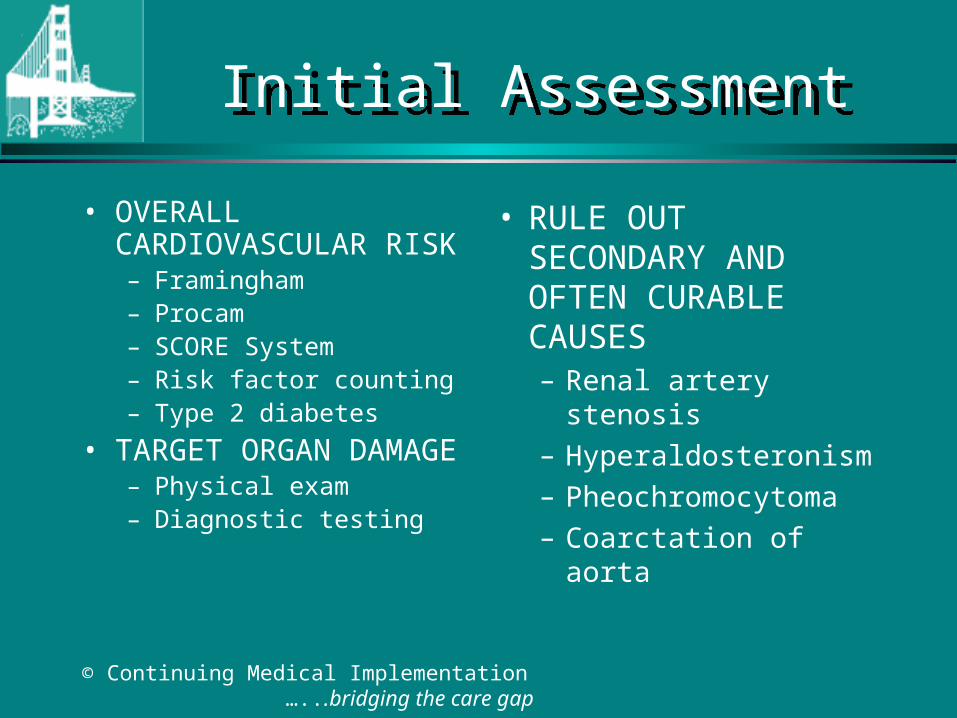
Initial AssessmentInitial Assessment
• OVERALL CARDIOVASCULAR RISK– Framingham– Procam– SCORE System– Risk factor counting– Type 2 diabetes
• TARGET ORGAN DAMAGE– Physical exam– Diagnostic testing
• RULE OUT SECONDARY AND OFTEN CURABLE CAUSES– Renal artery stenosis
– Hyperaldosteronism
– Pheochromocytoma
– Coarctation of aorta
© Continuing Medical Implementation …...bridging the care gap
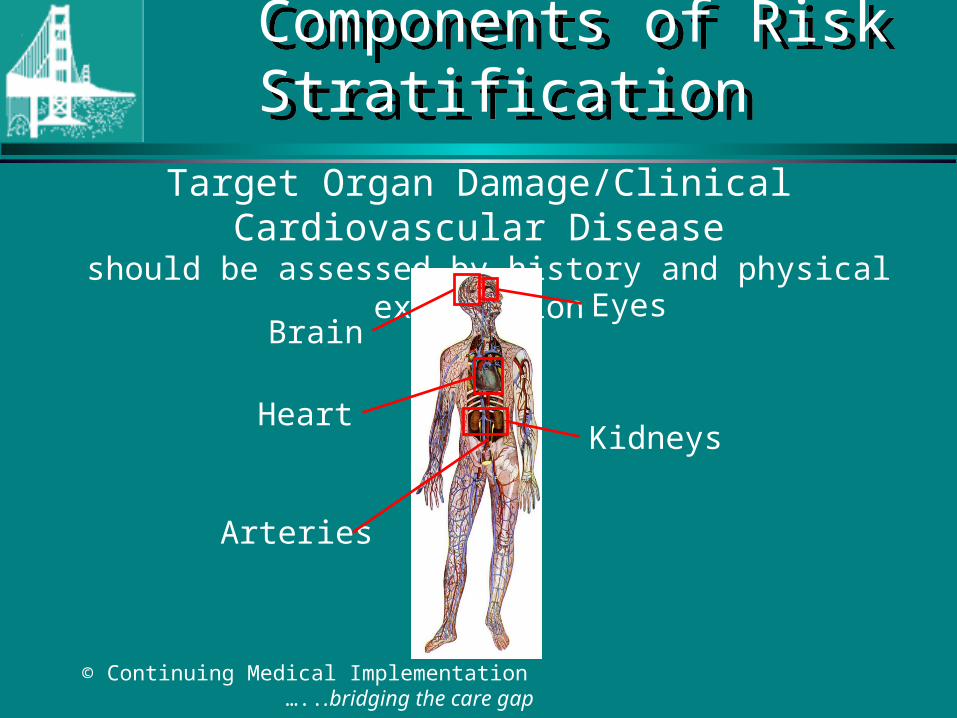
Target Organ Damage/Clinical Cardiovascular Disease should be assessed by history and physical examination
Components of Risk Stratification
Components of Risk Stratification
Brain
HeartKidneys
Eyes
Arteries
© Continuing Medical Implementation …...bridging the care gap
Important Aspects of the Physical Examination in the Hypertensive PatientImportant Aspects of the Physical Examination in the Hypertensive Patient
• Accurate measurement of blood pressure• General appearance: distribution of body fat, skin lesions,
muscle strength, alertness• Fundoscopy• Neck: palpation and auscultation of carotids, thyroid• Heart: size, rhythm, sounds• Lungs: rhonchi, rales• Abdomen: renal masses, bruits over aorta or renal arteries,
femoral pulses• Extremities: peripheral pulses, edema• Neurologic assessment
© Continuing Medical Implementation …...bridging the care gap
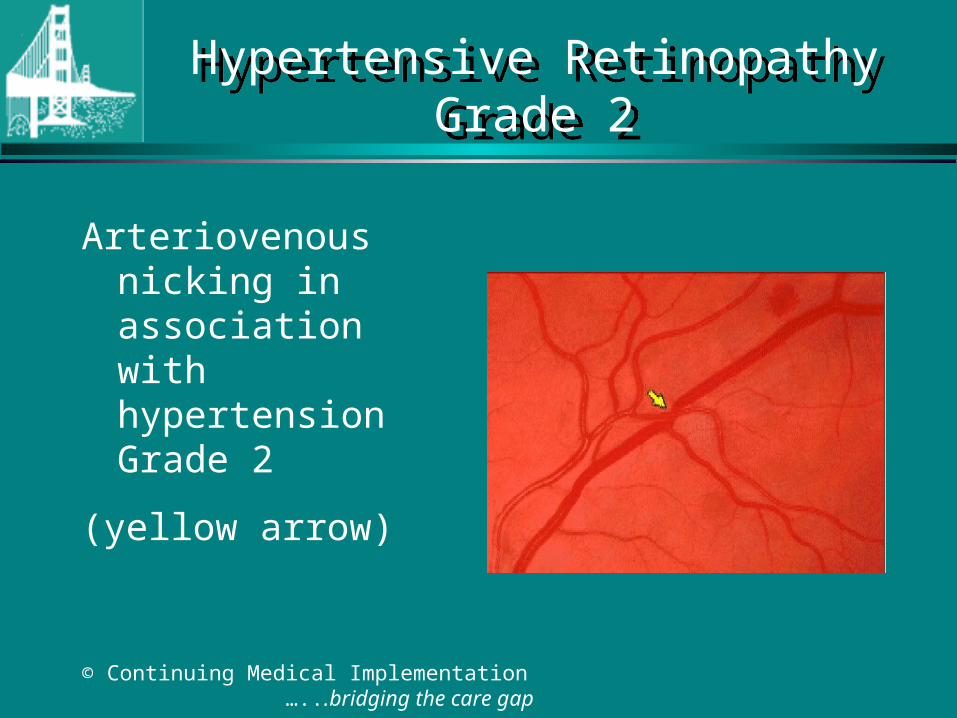
Hypertensive RetinopathyGrade 2
Hypertensive RetinopathyGrade 2
Arteriovenous nicking in association with hypertension Grade 2
(yellow arrow)
© Continuing Medical Implementation …...bridging the care gap
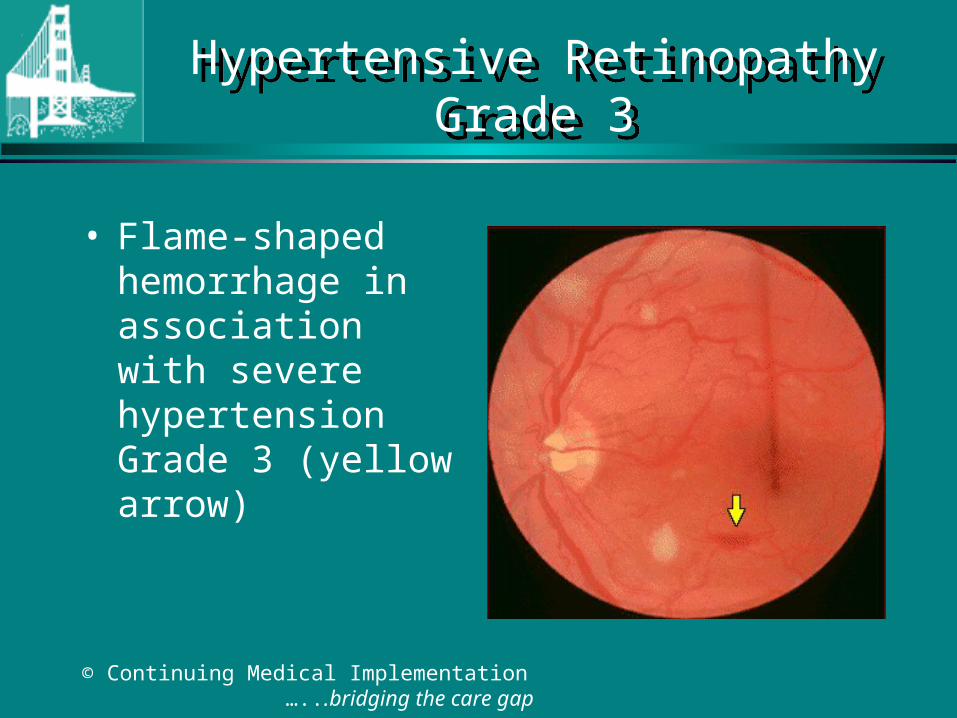
Hypertensive RetinopathyGrade 3
Hypertensive RetinopathyGrade 3
• Flame-shaped hemorrhage in association with severe hypertension Grade 3 (yellow arrow)
© Continuing Medical Implementation …...bridging the care gap
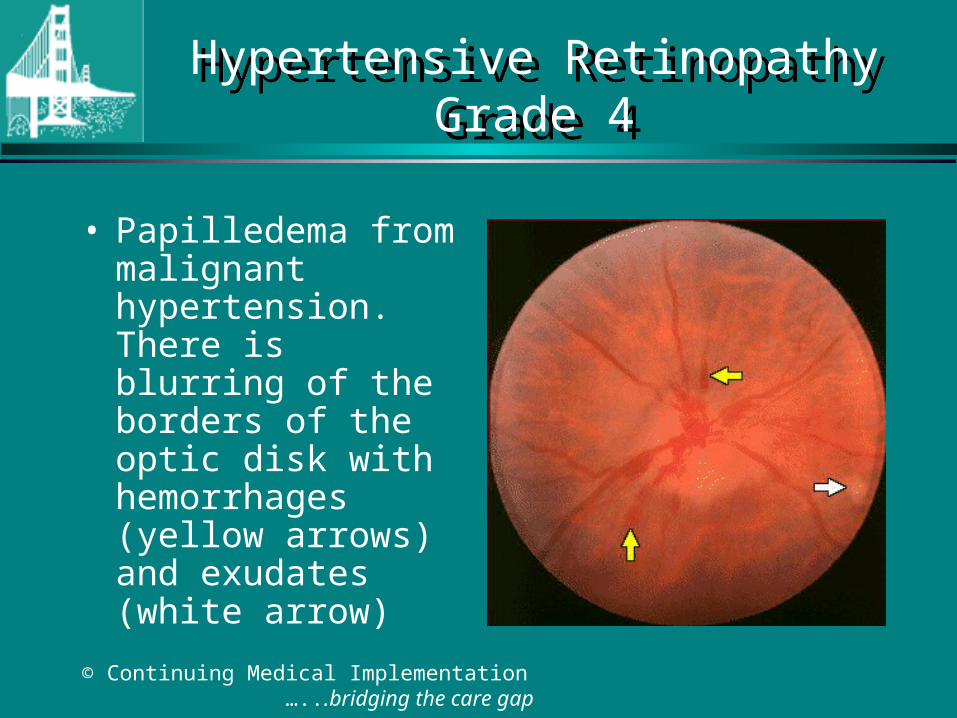
Hypertensive RetinopathyGrade 4
Hypertensive RetinopathyGrade 4
• Papilledema from malignant hypertension. There is blurring of the borders of the optic disk with hemorrhages (yellow arrows) and exudates (white arrow)
© Continuing Medical Implementation …...bridging the care gap
Clinical Signs of LV Dysfunction
Clinical Signs of LV Dysfunction
• Hypotension• Pulsus alternans• Reduced volume
carotid• LV apical
enlargement/displacement
• Sustained apex - to S2
• Soft S1• Paradoxically split S2• S3 gallop
(not S4 = impaired LV compliance)
• Mitral regurgitation• Pulmonary congestion
– rales
© Continuing Medical Implementation …...bridging the care gap
Routine laboratory tests for the investigation of all patients with hypertension:
1. Urinalysis 2. Complete blood cell count 3. Blood chemistry (potassium, sodium and
creatinine) 4. Fasting glucose 5. Fasting total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, triglycerides 6. Standard 12 ECG
CHS RecommendationsRoutine Laboratory Investigations
CHS RecommendationsRoutine Laboratory Investigations
© Continuing Medical Implementation …...bridging the care gap
What are the indications for checking the BP in both arms?
What are the indications for checking the BP in both arms?
• The presence of both arms– R/O
• Atherosclerotic obstruction
• Scalenus anticus syndrome/cervical rib
• Aortic coarctation above left subclavian
• Anomalous origin right subclavian artery in aortic coarctation
© Continuing Medical Implementation …...bridging the care gap
What are the indications for checking BP in the lower extremities?
What are the indications for checking BP in the lower extremities?
– Hypertensive patient under 40 years of age.– Elderly patient with suspected PVD
How do you do it?– Thigh cuff-auscultate over popliteal artery– Large arm cuff around calf (bladder posterior)
-palpate PT or DP
Which is normally higher- arm or leg BP?
© Continuing Medical Implementation …...bridging the care gap
Ankle-brachial indexAnkle-brachial index
• Resting and post exercise SBP in ankle and arm.– Normal ABI > 1– ABI < .9 has 95% sensitivity for
angiographic PVD– ABI 0.5- 0.84 correlates with claudication– ABI < 0.5 indicates advanced ischaemia
© Continuing Medical Implementation …...bridging the care gap
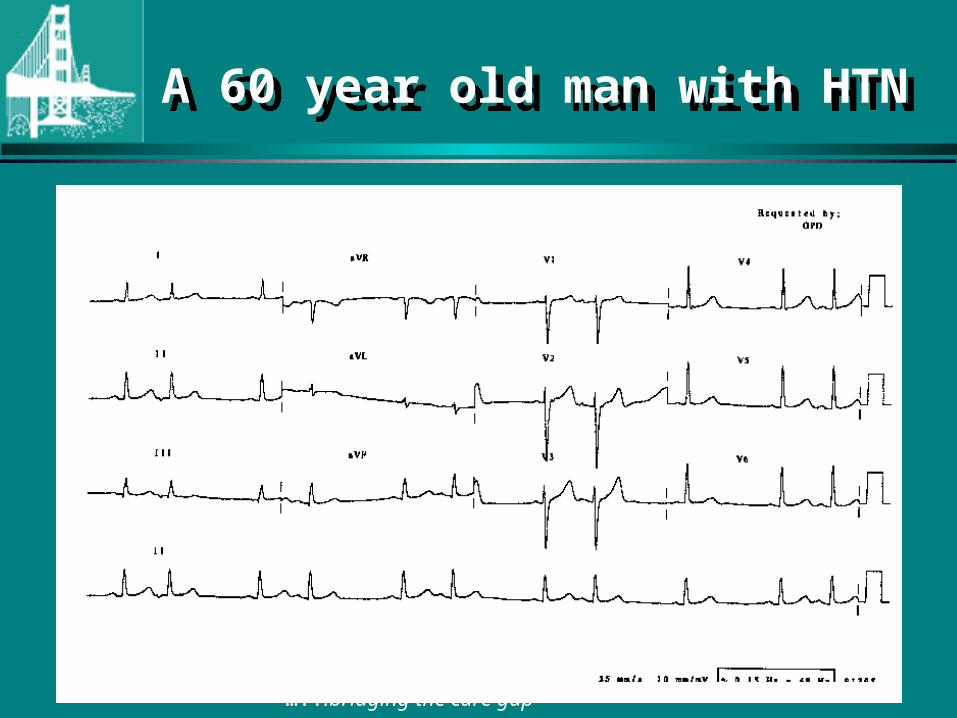
A 60 year old man with HTNA 60 year old man with HTN
© Continuing Medical Implementation …...bridging the care gap
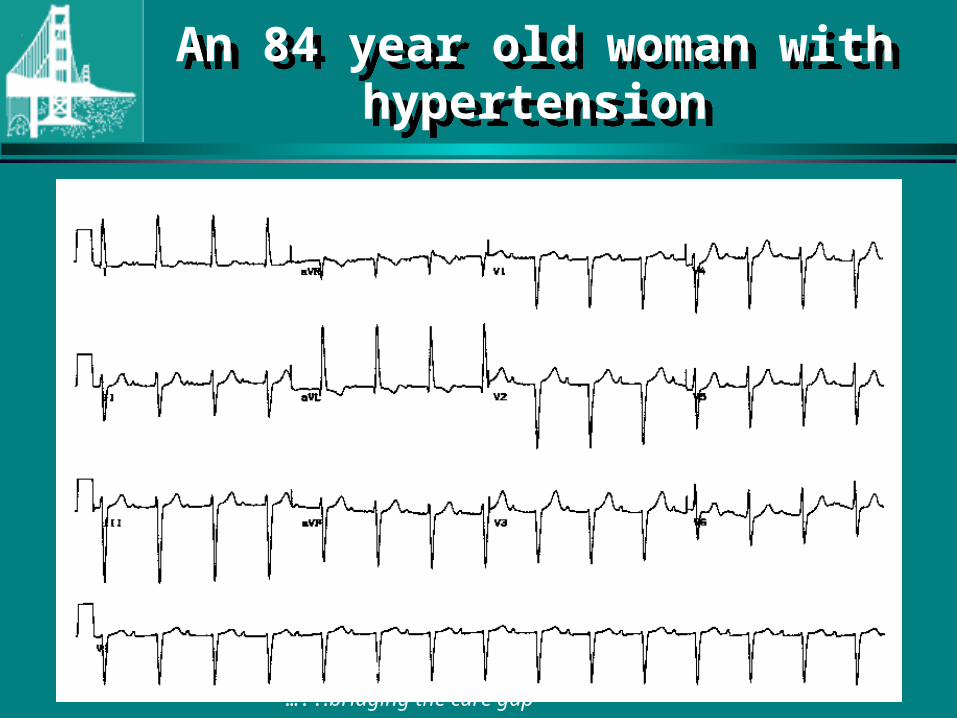
An 84 year old woman with hypertension
An 84 year old woman with hypertension
© Continuing Medical Implementation …...bridging the care gap
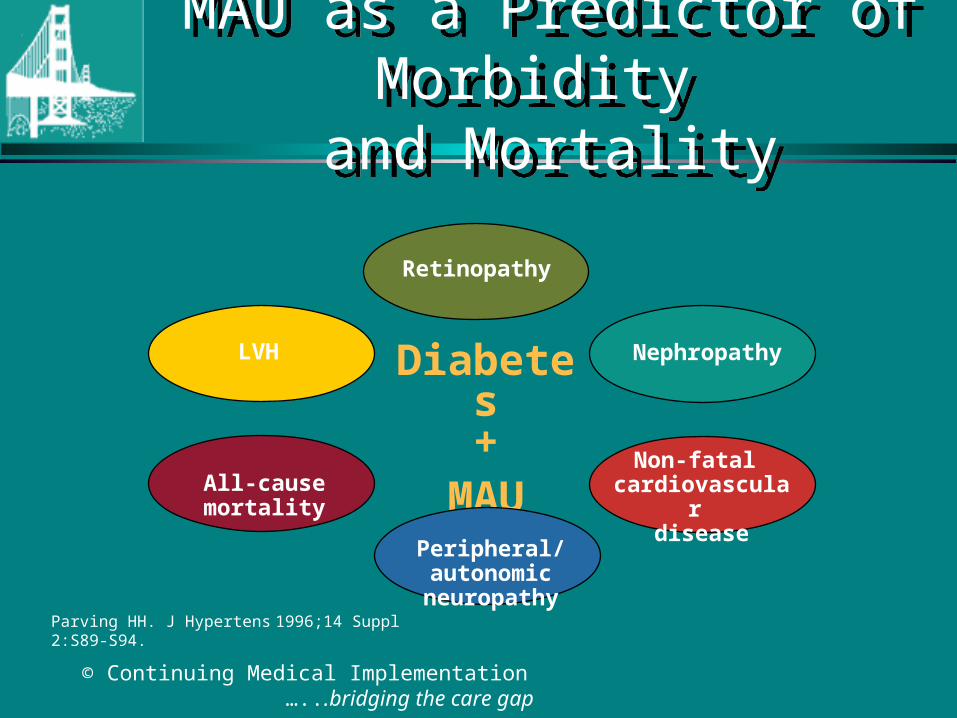
MAU as a Predictor of Morbidity
and Mortality
MAU as a Predictor of Morbidity
and Mortality
Retinopathy
Diabetes+
MAU
LVH
Non-fatal cardiovascular
diseaseAll-cause mortality
Nephropathy
Peripheral/autonomic neuropathy
Parving HH. J Hypertens 1996;14 Suppl 2:S89-S94.
© Continuing Medical Implementation …...bridging the care gap
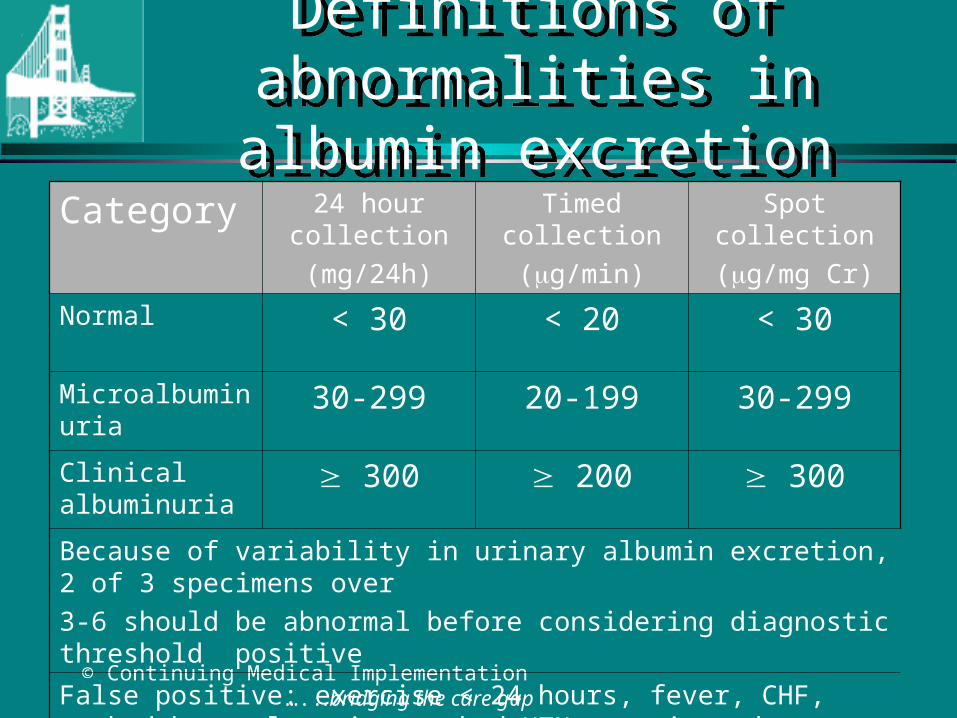
Definitions of abnormalities in albumin excretion
Definitions of abnormalities in albumin excretion
Category 24 hour collection
(mg/24h)
Timed collection
(g/min)
Spot collection
(g/mg Cr)
Normal < 30 < 20 < 30Microalbuminuria
30-299 20-199 30-299
Clinical albuminuria
300 200 300
Because of variability in urinary albumin excretion, 2 of 3 specimens over
3-6 should be abnormal before considering diagnostic threshold positive
False positive: exercise < 24 hours, fever, CHF, marked hyperglycemia, marked HTN, pyuria and hematuria.
© Continuing Medical Implementation …...bridging the care gap
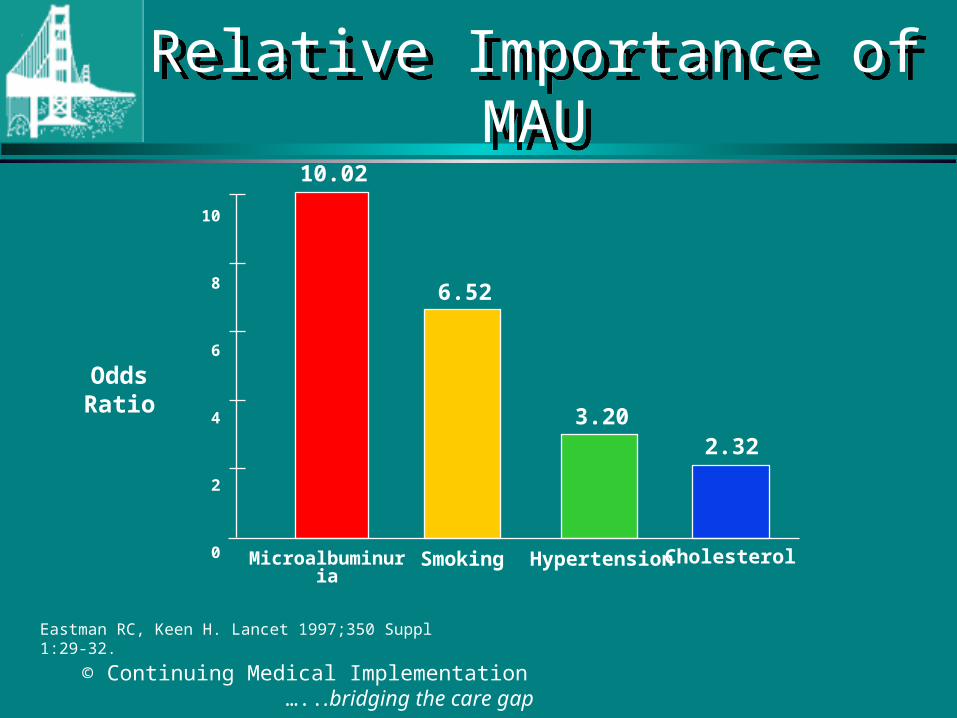
Eastman RC, Keen H. Lancet 1997;350 Suppl 1:29-32.
Microalbuminuria
10
8
6
4
2
0
10.02
Smoking Hypertension
Odds Ratio
6.52
Cholesterol
2.323.20
Relative Importance of MAURelative Importance of MAU
© Continuing Medical Implementation …...bridging the care gap
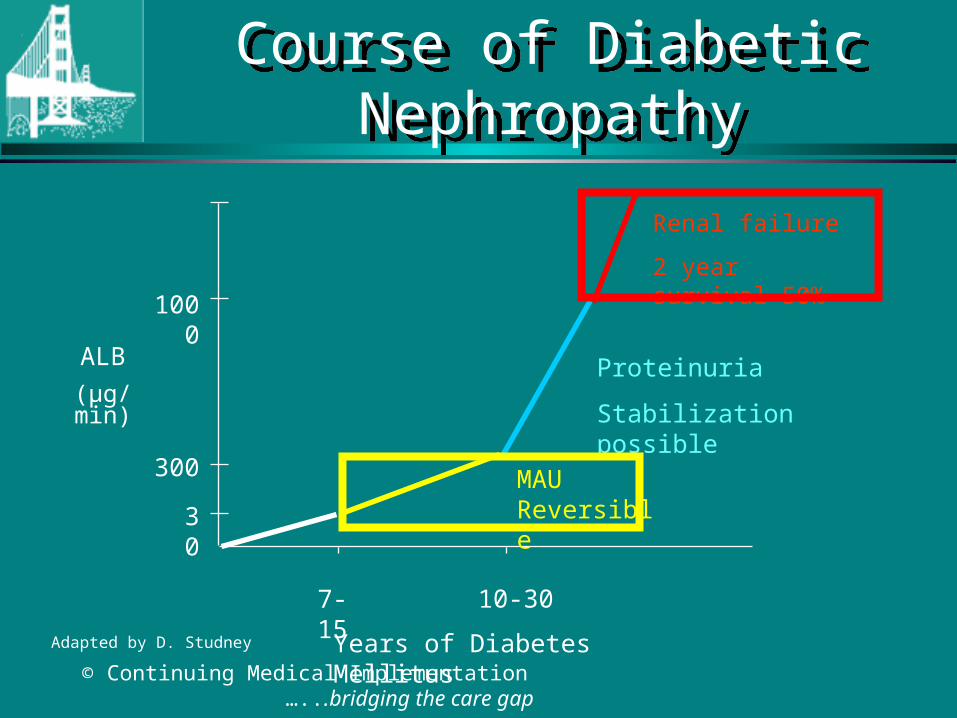
ALB
(µg/min)
1000
300
30
Years of Diabetes Mellitus
7-15 10-30
Proteinuria
Stabilization possible
Renal failure
2 year survival 50%
MAU Reversible
Adapted by D. Studney
Course of Diabetic NephropathyCourse of Diabetic Nephropathy