-author - disease managementskydiseasemanagement.com/.../2015/10/sky-dm-10.19.2… · web viewthe...
TRANSCRIPT

IntroductionIn 1996 at the City of Asheville in Asheville, North Carolina, a ’new model’ of healthcare was emerging which involved identifying high-risk health plan members and conducting one-on-one meetings with healthcare personnel. The goal was to get the high risk medical plan members to become compliant with the medical norms of their specific health condition or disease. These efforts ultimately received national notoriety and became known as the Asheville Project and later through national grants as Ten City Challenge.
In the years that followed, over $2,000,000 was spent studying the effectiveness of the program. In the end, the program is the most independently researched, peer reviewed, and published disease management program in existence! Simply put, the results speak for themselves.
Financial ResultsA recent study of the total medical claims of our employer clients versus that of a major, national insurance carrier revealed our claims were 19% less than their norms. These results were achieved through our nurses meeting one-on-one with high risk participants, every month.
Sky Disease Management delivers highly measurable and identifiable data showing actual claims savings to our clients, and due to this success we have built great stop loss relationships with preferred pricing and plan provisions. Through coupling our medical management with the procurement of reinsurance, you can now capture full credit for your health management efforts.
1 | P a g e

Our HistoryThe Asheville Project
Nearly 20 years ago, a group of researchers at the University of North Carolina School of Pharmacy had a theory for an improved model of healthcare delivery. Specifically, they were interested in studying the financial impact to employer medical plan costs which could be obtained if medical plan participants would remain compliant with their prescribed medications. With their premise in hand, the next step was to find an employer partner who would be willing to experiment with them. This partnership was eventually forged with the City of Asheville in Asheville, North Carolina.
The Asheville Project, as it was later named, began with a narrow focus on their diabetic population of employees. Diabetic patients were chosen specifically due to the comorbidities (multiple other chronic health conditions) that are generally present in diabetics. Numerous studies have documented the following in diabetic patients::
2 to 4 times greater risk of heart disease 60% to 65% have hypertension 2 to 4 times greater risk of stroke 60% to 70% have some degree of nervous system damage Leading cause of adult blindness Leading cause of end-stage renal disease (ESRD), and accounts for 40% of all new cases Accounts for 50% of lower limb amputations
The program implementation involved a nurse or pharmacist to meeting one-on-one with each identified high risk diabetic on the medical plan. The goal of these ongoing quarterly meetings was to ensure the patients actually complied with the prescribed overall medical standard for their condition. In addition, the copays and other associated costs for diabetic testing were waived, thus removing any financial barrier to compliance.
At the time there existed published research showing that if the hemoglobin A1C (90 day measure of blood sugar) of diabetic patients were to reduce just 1 point, you could expect to see all of the comorbid conditions to reduce by 50%. This meant that even a small improvement in these health plan member’s A1C levels would see all of the associated health conditions cut in half. Obviously achieving this goal was worth the effort, and thus the programs was implemented and communicated to the employees.
2 | P a g e

Our HistoryResults of the Asheville Project
At the program’s implementation, the City of Asheville took a long view regarding results, assuming that they would not be able to see a measurable improvement for between 3 and 5 years. They soon discovered that their expectations were extremely conservative as they began to see the measurable impact of hemoglobin A1C readings of their diabetic population decrease substantially. In only 8 month after program’s implementation, the average A1C reading had decreased from 7.6 to 7.0. After 14 months, the readings had experienced an even further reduction.
Based upon the research, these outcomes suggested an expectation for a 70% reduction in the comorbid conditions for these diabetic members. Below is a graph (left) of the measured readings for all of their population over the first 5 years of the program.
There were also significant changes to other indirect employment costs of these patients in terms of sick-leave usage and disability usage. Below is the graph (right) of measured sick leave over the first 5 years of the program.
3 | P a g e

Our HistoryFinancial Impact to Medical Costs
Obviously the City of Asheville was quite pleased with the initial results of reducing hemoglobin A1C readings of their diabetic patients. Shortly after, they began to experience the financial implications of their efforts as overall medical costs associated with these high risk members reduced by 35% in the first year alone.
Below is a graph of actual published data regarding the medical claims of the City of Asheville for the first 5 years of the programs implementation. These figures were initially published in the Journal of American Pharmacists Association based upon the research performed by Dr. Barry Bunting and Dr. Carole Cranor.
As you will notice, prescription drug expenses actually increased under the program as members were given access to certain free medications to ensure their prescription drug compliance, but as compliance went up, large dollar medical claims began to shrink dramatically.
4 | P a g e

Research and OutcomesNearly $2,000,000 in Grants Awarded to Study the Asheville
Project
As the outcomes of the Asheville Project began to be published, the program received significant national attention and notoriety. The program was particularly interesting to the pharmaceutical industry since the results suggested that more revenue spent on prescription drugs would reduce overall total healthcare costs. Several of the world’s largest pharmaceutical companies gave significant grants for the purpose of more scientifically studying the program. These grants, given by a variety of organizations, totaled over $2,000,000.
As a result, the Asheville Project became the most studied, peer reviewed, and published disease management program ever. You can review these articles on these studies by clicking on this link here.
5 | P a g e
Because of the vast amount of resources dedicated to studying our approach to disease management, we can confidently say that our program is one of the most independently researched and peer reviewed disease management program in existence. - John Miall, co-founder of The Asheville Project

Research and Outcomes5 Year Outcomes | Hypertension, Asthma and Diabetes |
With the initial success regarding diabetes, the program began to quickly extend to other diseases states including the following conditions now currently actively managed under our disease management program which including: hypertension, asthma, diabetes, back pain, hyperlipidemia, neck pain, depression, headache, congestive heart failure, liver disease, atrial fibrillation, osteoporosis, immune disorders, kidney failure and many more.
With the large number of patients studied in the areas of hypertension, diabetes and asthma, the following 3 studies and outcomes are usually of particular interest to employers.
Hypertension. 5 Year, 6200+ Patients. Journal of American Pharmaceuticals Association.
o 53% decrease in risk of cardiovascular event.
o 50%+ reduction in risk of related cardiovascular emergency department visit.
o 31% reduction in medical costs related to cardiovascular patients.
o View External Research Article.
Diabetes Study. 5 Year, 200 Patients, Journal of American Pharmaceuticals Association.
o Total direct medical cost decrease $1,200 to $1,872 per patient per year.
o Estimated productivity increases estimated at $18,000 annually.
o View External Research Article.
Asthma Study. 5 Year, 200+ Patients. Journal of American Pharmaceuticals Association.
o Total direct medical cost decrease $725 per patient per year.
o Indirect cost savings estimation of $1,230 per patient per year.
o View External Research Article.
6 | P a g e

Research and OutcomesThe Asheville Project versus All Fully Insured Medical Plans
Since the initial implementation of the Asheville Project at the City of Asheville, there have been hundreds of program replications at various employers across the country. The results obtained by employers willing to adopt the program continue to be measured and remain impressive.
Each year all commercial fully insured carriers must report their HEDIS clinical results to the National Committee for Quality Assurance (NCQA). These clinical measures show various compliance measures of their health population. In the figure below, you will see the results on average of the NCQA commercial carriers versus those employers who have implemented our approach to disease management. As you would expect, compliance rates for medical plan members under our approach continue to show significantly better outcomes.
7 | P a g e

Sky Disease Management Outcomes-19% Claims versus National Norms
One of the indications of our programs success was when large national insurance carriers began to contract to implement our disease management on their normal fully insured population of health plan members. One of the largest of these national insurance carriers recently conducted a study comparing the results of employer groups with our disease management implemented versus their norms. The study was performed on various disease specific states, as indicated in the figure below.
8 | P a g e
The overall results of the study showed that claims were on average 19% less for employers who had implemented our approach to disease management for at least 12 months.

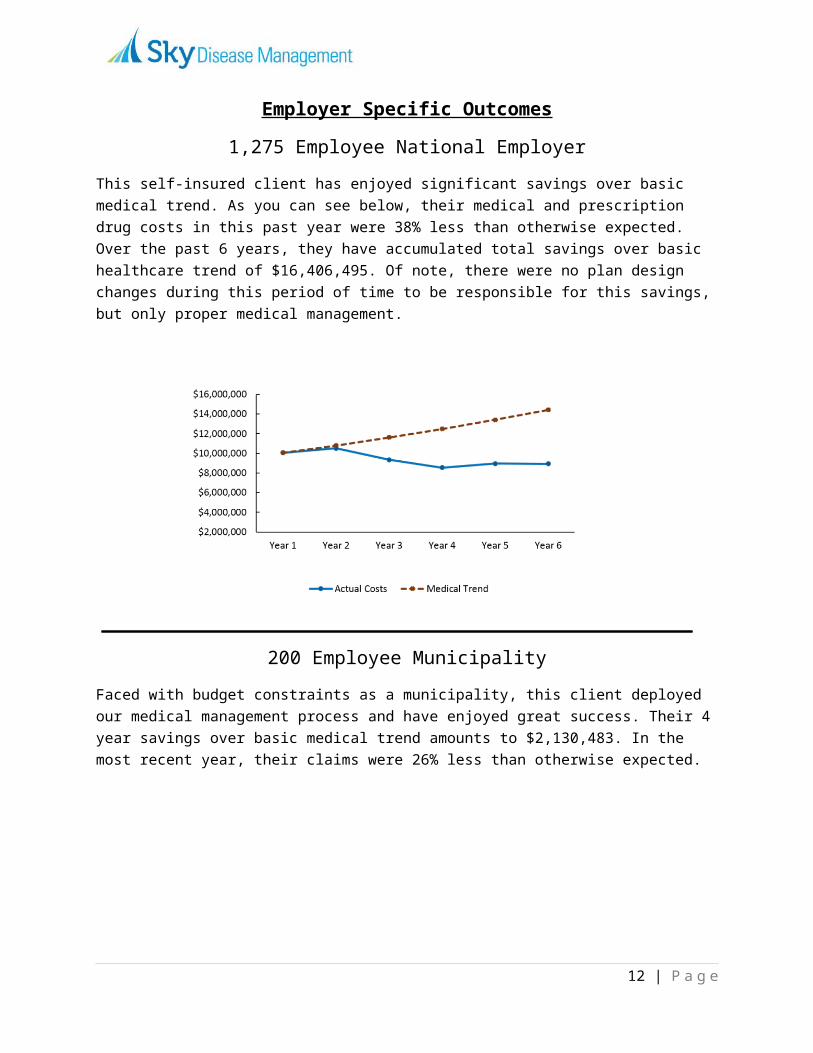
Employer Specific Outcomes1,275 Employee National Employer
This self-insured client has enjoyed significant savings over basic medical trend. As you can see below, their medical and prescription drug costs in this past year were 38% less than otherwise expected. Over the past 6 years, they have accumulated total savings over basic healthcare trend of $16,406,495. Of note, there were no plan design changes during this period of time to be responsible for this savings, but only proper medical management.
200 Employee MunicipalityFaced with budget constraints as a municipality, this client deployed our medical management process and have enjoyed great success. Their 4 year savings over basic medical trend amounts to $2,130,483. In the most recent year, their claims were 26% less than otherwise expected.
9 | P a g e

Employer Specific Outcomes290 Employee Automotive Industry
This multi-state self-funded client has had great success with their claims history since implementing our medical management. Over the past 4 years, they have accumulated savings of $2,015,232 over normal medical trend. In the most recent year, their claims were 23% less than expected trend, resulting a single year savings in excess of $750,000.
125 Employee ClientThe middle market employer space is quite competitive. This client’s healthcare savings has significantly added up to $627,787. In the most recent year, they experienced medical costs 22.5% less than expected based upon normal healthcare trend.
10 | P a g e

Sky Disease ManagementEvidence Based Medical Norms and Employee Compliance
Risk Assessment and Stratification
Our proprietary risk reduction process begins by identifying current and potential high risk members within your group. This is typically performed through a health risk assessment distributed to all adult members on the health plan (or only adult employee members, as the client desires). If the employer has access to more robust claims information systems, we would request to have access to this information also.
Once these risk assessments have been returned, our medical staff will begin their review to identify the high risk members whom will be targeted for ongoing monthly meetings. The typical employer will have 90% of the employees considered ‘under control’ after this risk assessment, and nothing will be required further of them for the given calendar year.
The remaining population of approximately 10% will be contacted and encouraged to participate with our nursing staff in the disease management program. Each individual employer can make their own determination regarding incentives they would wish to deliver to employees for their participation, such as reduced copays for certain drugs or other financial incentives.
One-on-One Meetings with High Risk Members
Once the high risk members have been identified, ongoing monthly meetings will begin based upon the disease management selected by the employer. During these meetings, each member will be given an actionable plan to help them become compliant with the evidence based medical norms for their particular conditions.
As an example, a medical plan participant with diabetes would have the following standard of care:
3 primary care office visits per year 2 to 4 hemoglobin A1C test per year Controlled blood pressure if normal is in excess of 140/90 Lipid profile controlled 1 dilated eye exam per year 1 urine screening per year
11 | P a g e
The program implementation involves a nurse to meet one-on-one with each identified high risk member the medical plan, typically 10% of the total adult members. The specific goal of these ongoing meetings is to build relationships and work with the plan participant to help them become compliant with the prescribed overall medical standard for their condition.
Sky Disease ManagementEvidence Based Medical Norms and Employee Compliance
Employee Compliance Reporting
Accountability is an important element of our disease management program, both for employees as well as between Sky and our employer clients. When possible, we recommend the use of claims measurements systems which provide data to assist in measuring the effectiveness of our program. Accountability and measurement are two elements which our make disease management significantly different than traditional wellness programs.
As an example under one particular such claims system, each employee is designated with a risk index (RI) based upon their actual medical claims history, pharmacy history and overall condition, as well as their basic demographics such as gender and age. The RI is a base number to describe the risk of the average person with these same conditions and demographics.
The employee is also given an adjusted risk index (ARI) which takes into account their actual compliance with the evidence based medical norms for their particular conditions. The goal becomes to work with these members to have them become more and more compliant with the recommended evidence based medical norms, thus moving the ARI as close as possible to their basic RI.
12 | P a g e

Sky Disease ManagementEvidence Based Medical Norms and Employee Compliance
The goal of Sky Disease Management nurses is to assist the employee in moving their adjusted risk index (ARI) as close as possible to their base risk index (RI). The manner in which this is achieved is through the employee’s compliance to their particular evidence based medical norms for their particular conditions.
This is accomplished in various ways based upon the information available to the nurse. Our program has been very successful on employer groups which have very little to no data, such as a fully insured plan. However when given the choice, it is our preference to have access to compliance reports such as the example below. In this particular claims system the nurse is given access to excellent data regarding employee compliance. Employee compliance reporting also adds measurement and accountability to the program, which is important for an employer to measure their return on investment.
13 | P a g e

Sky Disease ManagementImplementation Time Line
Week 1
Client enters into contract and signs business associate agreement Health risk assessment begins, and authorization documents are distributed to employees Initiate any desired onsite lab draw, or arrange for alternative method of obtaining
biometric testing Documents are remitted to Sky and risk assessment and stratification begins If necessary, recruiting begins for additional nursing staff that is best suited to the client’s
specific needs
Week 2
Risk assessment and stratification of all participants continues based on the health risk assessments
Receipt and review of client group’s lab results If necessary, vetting of potential nurse candidates
Week 3
If necessary, begin interview process for registered nurse Risk assessment and stratification is concluded
Week 4
If necessary, conclude interview process, select new hired nurse candidate
Week 5-7
If necessary, implement nurse training program Introduce selected registered nurse to client Provide client with information necessary to begin scheduling initial employee appointments
Week 8
Begin scheduled high risk member employee appointments Schedule return dates and follow-up appointments for worksite.
14 | P a g e