· ana carla pereira de araujo, bruno f. de oliveira santos, flavia ricci calasans, ibraim m....
TRANSCRIPT

www.arquivosonline.com.br Sociedade Brasileira de Cardiologia • ISSN-0066-782X • Volume 103, Nº 5, November 2014
EditorialCardiovascular Computed Tomography and Magnetic Resonance:
History and Growing Impact in Brazil and in the World
Original ArticlesSleep Apnea and Nocturnal Cardiac Arrhythmia: A Populational Study
Applicability of the Appropriate use Criteria for Myocardial Perfusion
Scintigraphy
Congenital Heart Disease as a Warning Sign for the Diagnosis of the
22q11.2 Deletion
Impact of Intensive Physiotherapy on Cognitive Function after
Coronary Artery Bypass Graft Surgery
Association of Aortic Valve Sclerosis with Previous Coronary Artery
Disease and Risk Factors
Prevention of Pazopanib-Induced Prolonged Cardiac Repolarization
and Proarrhythmic Effects
Hemodynamic Effects of Noninvasive Ventilation in Patients with
Venocapillary Pulmonary Hypertension
Physical Stress Echocardiography: Prediction of Mortality and Cardiac
Events in Patients with Exercise Test showing Ischemia
Determinants of Functional and Structural Properties of Large Arteries
in Healthy Individuals
Review ArticleEffects of Yoga in Patients with Chronic Heart Failure: A Meta-Analysis
Letter to the EditorACE I/D Gene Polymorphism in Children with Family History of
Premature Coronary Disease
Erratum
Eletronic Pages
Anatomopathological SessionCase 5/2014 - 41-Year-Old Woman with Rheumatic Disease
and Previous Mitral Valve Repair with Pulmonary Embolism and
Cardiogenic and Septic Shock
Case ReportMultiple Benefits of Rehabilitation in a Patient with Heart and Renal Failure
ImageLeft Internal Mammary Artery Graft-to-Pulmonary Artery Fistula
Graph 1 – Main heart diseases affecting 47 patients with the 22q11.2 deletion syndrome. Page 385
Otherheart diseases
(27.7%)
Tetralogy ofFallot
(38.3%)
Ventricularseptal defect
(21.3%)
Pulmonaryatresia(12.7%)
Tetralogy of Fallot
Ventricular Septal Defect
Pulmonary AtresiaOther Heart Diseases
38.3%
12.7%
21.3%
27.7%

Arquivos Brasileiros de Cardiologia - Volume 103, Nº 5, November 2014
A JOURNAL OF SOCIEDADE BRASILEIRA DE CARDIOLOGIA - Published since 1948
Contents
Editorial
Cardiovascular Computed Tomography and Magnetic Resonance: History and Growing Impact in Brazil and in the WorldMarcelo Souto Nacif e Carlos Eduardo Rochitte.....................................................................................................................................................................page 362
Original Articles
Clinical Arrhythmia
Sleep Apnea and Nocturnal Cardiac Arrhythmia: A Populational StudyFatima Dumas Cintra, Renata Pimentel Leite, Luciana Julio Storti, Lia Azeredo Bittencourt, Dalva Poyares, Laura de Siqueira Castro, Sergio Tufik, Angelo de Paola.....................................................................................................................................................................page 368
Nuclear Cardiology and PET
Applicability of the Appropriate use Criteria for Myocardial Perfusion ScintigraphyAnderson de Oliveira, Maria Fernanda Rezende, Renato Corrêa, Rodrigo Mousinho, Jader Cunha Azevedo, Sandra Marina Miranda, Aline Ribeiro Oliveira1, Ricardo Fraga Gutterres, Evandro Tinoco Mesquita, Cláudio Tinoco Mesquita.....................................................................................................................................................................page 375
Pediatric Cardiology
Congenital Heart Disease as a Warning Sign for the Diagnosis of the 22q11.2 DeletionMarcília S. Grassi, Cristina M. A. Jacob, Leslie D. Kulikowski, Antonio C. Pastorino, Roberta L. Dutra, Nana Miura, Marcelo B. Jatene, Stephanie P. Pegler, Chong A. Kim, Magda Carneiro-Sampaio.....................................................................................................................................................................page 382
Heart Surgery - Adults
Impact of Intensive Physiotherapy on Cognitive Function after Coronary Artery Bypass Graft SurgeryElder dos Santos Cavalcante, Rosmeiri Magario, César Augusto Conforti, Gerson Cipriano Júnior, Ross Arena, Antonio Carlos C. Carvalho, Enio Buffolo, Bráulio Luna Filho.....................................................................................................................................................................page 391
Echocardiography (Adults)
Association of Aortic Valve Sclerosis with Previous Coronary Artery Disease and Risk FactorsFilipe Carvalho Marmelo, Sónia Matilde Fonseca Mateus, Alexandre José Marques Pereira.....................................................................................................................................................................page 398

Arquivos Brasileiros de Cardiologia - Volume 103, Nº 5, November 2014
Electrophysiology/Arrhythmias
Prevention of Pazopanib-Induced Prolonged Cardiac Repolarization and Proarrhythmic EffectsTulay Akman, Oytun Erbas, Levent Akman, Ahmet U. Yilmaz.....................................................................................................................................................................page 403
Hemodynamics - Adults
Hemodynamic Effects of Noninvasive Ventilation in Patients with Venocapillary Pulmonary HypertensionAndré Moreira Bento, Luiz Francisco Cardoso, Flávio Tarasoutchi, Roney Orismar Sampaio, Luiz Junya Kajita, Pedro Alves Lemos Neto.....................................................................................................................................................................page 410
Other Cardiovascular Imaging Techniques
Physical Stress Echocardiography: Prediction of Mortality and Cardiac Events in Patients with Exercise Test showing IschemiaAna Carla Pereira de Araujo, Bruno F. de Oliveira Santos, Flavia Ricci Calasans, Ibraim M. Francisco Pinto, Daniel Pio de Oliveira, Luiza Dantas Melo, Stephanie Macedo Andrade, Irlaneide da Silva Tavares, Antonio Carlos Sobral Sousa, Joselina Luzia Menezes Oliveira.....................................................................................................................................................................page 418
Other Diagnostic Tests (not involving imaging)
Determinants of Functional and Structural Properties of Large Arteries in Healthy IndividualsElaine Cristina Tolezani, Valéria Costa-Hong, Gustavo Correia, Alfredo José Mansur, Luciano Ferreira Drager, Luiz Aparecido Bortolotto.....................................................................................................................................................................page 426
Review Article
Effects of Yoga in Patients with Chronic Heart Failure: A Meta-AnalysisMansueto Gomes-Neto, Erenaldo Sousa Rodrigues-Jr, Walderi Monteiro Silva-Jr, Vitor Oliveira Carvalho.....................................................................................................................................................................page 433
Letter to the Editor
ACE I/D Gene Polymorphism in Children with Family History of Premature Coronary DiseaseDilek Yý lmaz Çiftdoð an.....................................................................................................................................................................page 440
Erratum
.....................................................................................................................................................................page 443

Arquivos Brasileiros de Cardiologia - Volume 103, Nº 5, November 2014
Arquivos Brasileiros de Cardiologia - Eletronic Pages
Anatomopathological Session
Case 5/2014 - 41-Year-Old Woman with Rheumatic Disease and Previous Mitral Valve Repair with Pulmonary Embolism and Cardiogenic and Septic ShockEduardo Gomes Lima, Ricardo D’Oliveira Vieira, Paula Bombonati, Jussara Bianchi Castelli..................................................................................................................................................................page e57
Case Report
Multiple Benefits of Rehabilitation in a Patient with Heart and Renal FailureCarlos Alberto Cordeiro Hossri, Fernando José Pinho Queiroga Júnior, Vitor Oliveira Carvalho, Carlos Roberto Ribeiro Carvalho, Andre Luis Pereira Albuquerque..................................................................................................................................................................page e68
Image
Left Internal Mammary Artery Graft-to-Pulmonary Artery FistulaEmmanouil Petrou and Ioannis Iakovou..................................................................................................................................................................page e72
* Indicate manuscripts only in the electronic version. To view them, visit: http://www.arquivosonline.com.br/2014/english/10305/edicaoatual.asp
Editorial BoardBrazilAguinaldo Figueiredo de Freitas Junior (GO)Alfredo José Mansur (SP)Aloir Queiroz de Araújo Sobrinho (ES)Amanda G. M. R. Sousa (SP)Ana Clara Tude Rodrigues (SP)André Labrunie (PR)Andrei Sposito (SP)Angelo A. V. de Paola (SP)Antonio Augusto Barbosa Lopes (SP) Antonio Carlos C. Carvalho (SP) Antonio Carlos Palandri Chagas (SP) Antonio Carlos Pereira Barretto (SP) Antonio Cláudio L. Nóbrega (RJ) Antonio de Padua Mansur (SP)Ari Timerman (SP)Armênio Costa Guimaraes (BA)Ayrton Pires Brandao (RJ)Beatriz Matsubara (SP)Brivaldo Markman Filho (PE)Bruno Caramelli (SP)Carisi A. Polanczyk (RS)Carlos Eduardo Rochitte (SP)Carlos Eduardo Suaide Silva (SP) Carlos Vicente Serrano Júnior (SP) Celso Amodeo (SP)Charles Mady (SP)Claudio Gil Soares de Araujo (RJ) Cláudio Tinoco Mesquita (RJ)Cleonice Carvalho C. Mota (MG)Clerio Francisco de Azevedo Filho (RJ)Dalton Bertolim Précoma (PR)Dário C. Sobral Filho (PE)Décio Mion Junior (SP)Denilson Campos de Albuquerque (RJ) Djair Brindeiro Filho (PE)Domingo M. Braile (SP)Edmar Atik (SP)Emilio Hideyuki Moriguchi (RS)
Enio Buffolo (SP)Eulógio E. Martinez Filho (SP) Evandro Tinoco Mesquita (RJ) Expedito E. Ribeiro da Silva (SP)Fábio Vilas-Boas (BA)Fernando Bacal (SP)Flávio D. Fuchs (RS) Francisco Antonio Helfenstein Fonseca (SP)Gilson Soares Feitosa (BA)Glaucia Maria M. de Oliveira (RJ)Hans Fernando R. Dohmann (RJ)Humberto Villacorta Junior (RJ)Ines Lessa (BA)Iran Castro (RS)Jarbas Jakson Dinkhuysen (SP)Joao Pimenta (SP)Jorge Ilha Guimaraes (RS)José Antonio Franchini Ramires (SP)José Augusto Soares Barreto Filho (SE)José Carlos Nicolau (SP)José Lázaro de Andrade (SP)José Péricles Esteves (BA)Leonardo A. M. Zornoff (SP)Leopoldo Soares Piegas (SP)Lucia Campos Pellanda (RS)Luís Eduardo Rohde (RS)Luís Cláudio Lemos Correia (BA)Luiz A. Machado César (SP)Luiz Alberto Piva e Mattos (SP)Marcia Melo Barbosa (MG)Maria da Consolaçao Moreira (MG)Mario S. S. de Azeredo Coutinho (SC)Maurício I. Scanavacca (SP)Max Grinberg (SP)Michel Batlouni (SP)Murilo Foppa (RS)Nadine O. Clausell (RS)Orlando Campos Filho (SP)Otávio Rizzi Coelho (SP)
Otoni Moreira Gomes (MG)Paulo Andrade Lotufo (SP)Paulo Cesar B. V. Jardim (GO)Paulo J. F. Tucci (SP)Paulo R. A. Caramori (RS)Paulo Roberto B. Évora (SP)Paulo Roberto S. Brofman (PR)Pedro A. Lemos (SP)Protásio Lemos da Luz (SP)Reinaldo B. Bestetti (SP)Renato A. K. Kalil (RS)Ricardo Stein (RS)Salvador Rassi (GO)Sandra da Silva Mattos (PE)Sandra Fuchs (RS)Sergio Timerman (SP)Silvio Henrique Barberato (PR)Tales de Carvalho (SC)Vera D. Aiello (SP)Walter José Gomes (SP)Weimar K. S. B. de Souza (GO)William Azem Chalela (SP)Wilson Mathias Junior (SP)
ExteriorAdelino F. Leite-Moreira (Portugal)Alan Maisel (Estados Unidos)Aldo P. Maggioni (Itália)Cândida Fonseca (Portugal)Fausto Pinto (Portugal)Hugo Grancelli (Argentina)James de Lemos (Estados Unidos)Joao A. Lima (Estados Unidos)John G. F. Cleland (Inglaterra)Maria Pilar Tornos (Espanha)Pedro Brugada (Bélgica)Peter A. McCullough (Estados Unidos)Peter Libby (Estados Unidos)Piero Anversa (Itália)
Scientific Director Maria da Consolaçao Vieira Moreira
Chief Editor Luiz Felipe P. Moreira
Associated Editors
Clinical Cardiology José Augusto Barreto-Filho
Surgical Cardiology Paulo Roberto B. Evora
Interventionist Cardiology Pedro A. Lemos
Pediatric/Congenital Cardiology Antonio Augusto Lopes
Arrhythmias/Pacemaker Mauricio Scanavacca
Non-Invasive Diagnostic Methods Carlos E. Rochitte
Basic or Experimental Research Leonardo A. M. Zornoff
Epidemiology/Statistics Lucia Campos Pellanda
Arterial Hypertension Paulo Cesar B. V. Jardim
Ergometrics, Exercise and Cardiac Rehabilitation Ricardo Stein
First Editor (1948-1953) † Jairo Ramos
A JOURNAL OF SOCIEDADE BRASILEIRA DE CARDIOLOGIA - Published since 1948www.arquivosonline.com.br
PresidentAngelo Amato V. de Paola
Vice-PresidentSergio Tavares Montenegro
Financial DirectorJacob Atié
Scientific DirectorMaria da Consolaçao Vieira Moreira
Administrative DirectorEmilio Cesar Zilli
Assistance Quality DirectorPedro Ferreira de Albuquerque
Communication DirectorMaurício Batista Nunes
Information Technology DirectorJosé Carlos Moura Jorge
Government Liaison DirectorLuiz César Nazário Scala
Director of State and Regional AffairsAbrahao Afiune Neto
Cardiovascular Health Promotion Director - SBC/FuncorCarlos Costa Magalhaes
Department DirectorEspecializados - Jorge Eduardo Assef
Research DirectorFernanda Marciano Consolim Colombo
Chief Editor of the Brazilian Archives of CardiologyLuiz Felipe P. Moreira
Special Advisor to the PresidencyFábio Sândoli de Brito
Adjunct Coordination
SBC Newsletter EditorNabil Ghorayeb e Fernando Antonio Lucchese
Continuing Education Coordination Estêvao Lanna Figueiredo
Norms and Guidelines Coordination Luiz Carlos Bodanese
Governmental Integration Coordination Edna Maria Marques de Oliveira
Regional Integration Coordination José Luis Aziz
Presidents of State and Regional Brazilian Societies of Cardiology
SBC/AL - Carlos Alberto Ramos Macias
SBC/AM - Simao Gonçalves Maduro
SBC/BA - Mario de Seixas Rocha
SBC/CE - Ana Lucia de Sá Leitao Ramos
SBC/CO - Frederico Somaio Neto
SBC/DF - Wagner Pires de Oliveira Junior
SBC/ES - Marcio Augusto Silva
SBC/GO - Thiago de Souza Veiga Jardim
SBC/MA - Nilton Santana de Oliveira
SBC/MG - Odilon Gariglio Alvarenga de Freitas
SBC/MS - Mércule Pedro Paulista Cavalcante
SBC/MT - Julio César De Oliveira
SBC/NNE - Jose Itamar Abreu Costa
SBC/PA - Luiz Alberto Rolla Maneschy
SBC/PB - Helman Campos Martins
SBC/PE - Catarina Vasconcelos Cavalcanti
SBC/PI - Joao Francisco de Sousa
SBC/PR - Osni Moreira Filho
SBC/RJ - Olga Ferreira de Souza
SBC/RN - Rui Alberto de Faria Filho
SBC/RS - Carisi Anne Polanczyk
SBC/SC - Marcos Venício Garcia Joaquim
SBC/SE - Fabio Serra Silveira
SBC/SP - Francisco Antonio Helfenstein Fonseca
SBC/TO - Hueverson Junqueira Neves
Sociedade Brasileira de Cardiologia
Presidents of the Specialized Departaments and Study GroupsSBC/DA - José Rocha Faria Neto
SBC/DECAGE - Josmar de Castro Alves
SBC/DCC - José Carlos Nicolau
SBC/DCM - Maria Alayde Mendonça da Silva
SBC/DCC/CP - Isabel Cristina Britto Guimaraes
SBC/DIC - Arnaldo Rabischoffsky
SBC/DERC - Nabil Ghorayeb
SBC/DFCVR - Ricardo Adala Benfati
SBC/DHA - Luiz Aparecido Bortolotto
SOBRAC - Luiz Pereira de Magalhaes
SBCCV - Marcelo Matos Cascado
SBHCI - Helio Roque Figueira
SBC/DEIC - Dirceu Rodrigues Almeida
GERTC - Clerio Francisco de Azevedo Filho
GAPO - Danielle Menosi Gualandro
GEECG - Joel Alves Pinho Filho
GEECABE - Mario Sergio S. de Azeredo Coutinho
GECETI - Gilson Soares Feitosa Filho
GEMCA - Alvaro Avezum Junior
GECC - Mauricio Wanjgarten
GEPREC - Glaucia Maria Moraes de Oliveira
Grupo de Estudos de Cardiologia Hospitalar - Evandro Tinoco Mesquita
Grupo de Estudos de Cardio-Oncologia - Roberto Kalil Filho
GEEC - Cláudio José Fuganti
GECIP - Gisela Martina Bohns Meyer
GECESP - Ricardo Stein
GECN - Ronaldo de Souza Leao Lima
GERCPM - Artur Haddad Herdy

Arquivos Brasileiros de Cardiologia
Affiliated at the Brazilian Medical Association
Volume 103, Nº 5, November 2014Indexing: ISI (Thomson Scientific), Cumulated Index Medicus (NLM), SCOPUS,
MEDLINE, EMBASE, LILACS, SciELO, PubMed
The ads showed in this issue are of the sole responsibility of advertisers, as well as the concepts expressed in signed articles are of the sole responsibility of their
authors and do not necessarily reflect the views of SBC.
This material is for exclusive distribution to the medical profession. The Brazilian Archives of Cardiology are not responsible for unauthorized access to its contents and
that is not in agreement with the determination in compliance with the Collegiate Board Resolution (DRC) N. 96/08 of the National Sanitary Surveillance Agency
(ANVISA), which updates the technical regulation on Drug Publicity, Advertising, Promotion and Information. According to Article 27 of the insignia, "the advertisement or publicity of prescription drugs should be restricted solely and exclusively to health
professionals qualified to prescribe or dispense such products (...)".
To ensure universal access, the scientific content of the journal is still available for full and free access to all interested parties at:
www.arquivosonline.com.br.
SUPPORT
Commercial Department
Phone: (11) 3411-5500
E-mail: [email protected]
Editorial Production
SBC - Internal Publication Department
Graphic Design and DiagrammingSBC - Internal Design Department
PrintIMOS Editora e Gráfica
Circulation1.500 copies
Address: Av. Marechal Câmara, 160 - 3º andar - Sala 330 20020-907 • Centro • Rio de Janeiro, RJ • Brasil
Phone.: (21) 3478-2700
E-mail: [email protected]
www.arquivosonline.com.br
SciELO: www.scielo.br

Editorial
Cardiovascular Computed Tomography and Magnetic Resonance: History and Growing Impact in Brazil and in the WorldMarcelo Souto Nacif1,2 and Carlos Eduardo Rochitte3,4,5
Hospital Universitário Antônio Pedro - HUAP - Setor de Ressonância Magnética e Tomografia Computadorizada Cardiovascular1; Pós-graduação em Ciências Cardiovasculares - Universidade Federal Fluminense - UFF2, Niterói, RJ; Instituto do Coração - InCor - Setor de Ressonância Magnética e Tomografia Computadorizada Cardiovascular3, São Paulo, SP; Hospital do Coração – HCOR - Associação do Sanatório Sírio4, São Paulo, SP; Hospital Pro-cardíaco5 - Rio de Janeiro, RJ - Brazil
Mailing Address: Marcelo Souto Nacif •Av. Sao Joao, 2400 – 232b. Jd Colinas, Postal Code 12242-000, Sao José dos Campos, SP - BrazilE-mail – [email protected]
KeywordsTomography, X-Ray Computed/history; Tomography,X-Ray
Computed/trends; Diagnostic Imaging/trends; Diagnostic Imaging/history; Magnetic Resonance Spectroscopy/history.
DOI: 10.5935/abc.20140186
Growth in Brazil and in the WorldCardiovascular computed tomography and magnetic
resonance are an important topic within the area of cardiovascular imaging in Brazil and in the world. In the Arquivos Brasileiros de Cardiologia this is not different, and despite the increased focus in clinical study, these two topics have grown in impact and scientific publications in recent years.
It is notorious the expansion of the national technological park with entrance of countless devices capable of performing advanced studies using cardiovascular tomography and magnetic resonance with increasing impetus for opening more centers specialized in these methods.
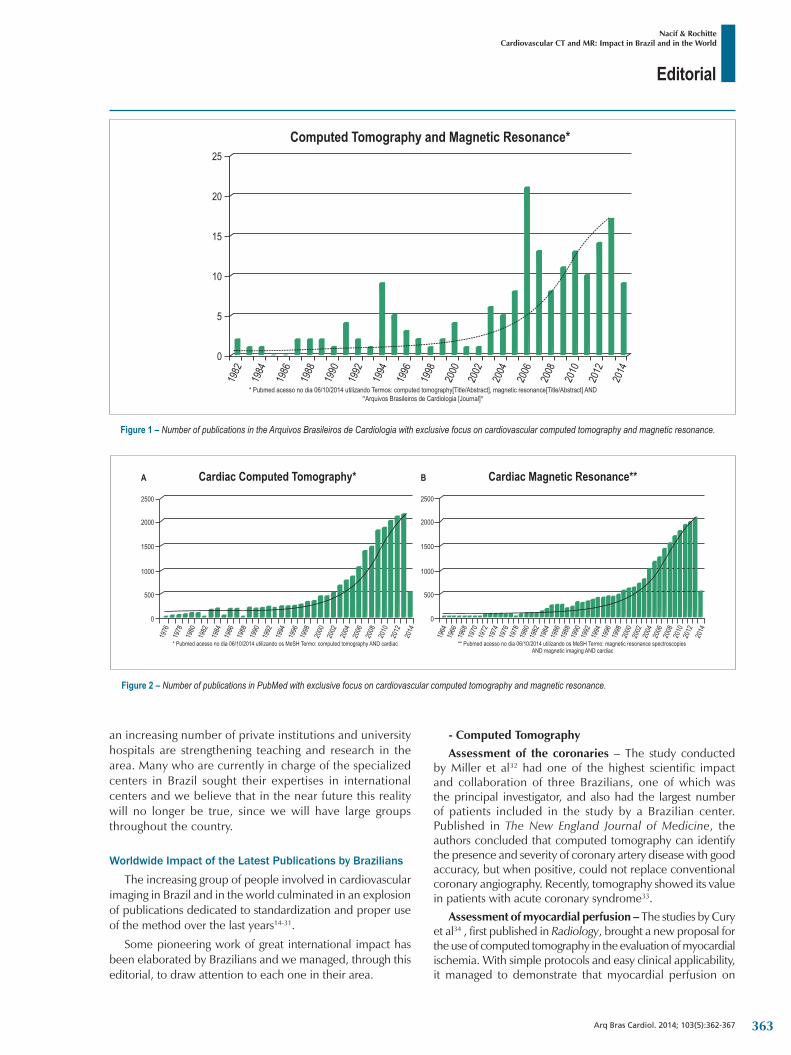
When we perform a systematic review using EndNote as a search tool and select only PubMed as a database with the words "magnetic resonance" and "computed tomography", in the Arquivos Brasileiros de Cardiologia alone we observe a total of 182 studies (Figure 1).
In parallel, when we perform a search on PubMed using the word "cardiac" and the MeSH (Medical Subject Headings) terms "computed tomography" and "magnetic resonance imaging", we find a sum of publications close to 45 thousand articles (44,711 articles) (Figure 2).
These graphics turn out to be merely illustrative, but are without doubt markers of the impact of these methods in Brazil (Figure 1) and in the world (Figure 2). It is easy to identify that after the year 2000 and in the last decade there has been a large insertion of these methods in the scientific scenario and we believe that this reflects also in the clinical scenario.
History in the Arquivos Brasileiros de CardiologiaThe first studies published in the Arquivos Brasileiros de
Cardiologia were basically clinical studies and case reports in which the methods were able to contribute to a better
diagnosis1-4. The first original articles emerged with the use of magnetic resonance imaging in the study by Kalil Filho et al5,6 in the year of 1995. At that same year, guided by Pinto et al7, emerged the first Brazilian consensus for the use of cardiac magnetic resonance imaging in clinical cardiology. Computed tomography had its first original study published in 1997, by Kalil et al8. One of the pioneering studies in the path of the evaluation of the current calcium score was performed by Feldman et al9.
Relationship with International SocietiesWe currently have two international societies dedicated
specifically to these methods. The SCMR (Society for Cardiovascular Magnetic Resonance) was the first society to be founded and by the year 2000, it was already organizing the process of credentialing for those dedicated to cardiovascular magnetic resonance10. The SCCT (Society of Cardiovascular Computed Tomography) was founded shortly after, following the advances of the method, and in 2009, made available its guidelines for better practice of the method11,12. In Brazil, the Arquivos Brasileiros de Cardiologia had a fundamental role in the publication of our first guideline13, which was updated this year (2014) and is currently undergoing editing for future publication.
Scientific and Educational Organization in BrazilIn the early days of the organization in Brazil, a study
group of cardiovascular magnetic resonance and computed tomography called GERT was formed and played a key role in the diffusion of knowledge throughout Brazil. A group of physicians dedicated to cardiovascular computed tomography and magnetic resonance created in Brazil the National Meeting of Cardiac Radiology (Encontro Nacional de Radiologia Cardíaca, ENRC), which will be on its eighth consecutive year in 2015. This group is composed of radiologists and cardiologists supported by SCMR and SCCT, along with national societies, to enhance the methods in Brazil and discuss the experiences in national territory. Similarly, SBC's Department of Cardiovascular Imaging (DIC), bringing together specialists in nuclear medicine, echocardiography, vascular ultrasound, and cardiovascular magnetic resonance and computed tomography, gathers annually in a meeting with almost 2 thousand participants and maintains the role of diffusing knowledge in the areas of cardiovascular magnetic resonance and computed tomography started with GERT.
We still have only a few training centers of experts in the field, mostly in the Rio-Sao Paulo hub, but in the last 5 years
362
Editorial
Nacif & RochitteCardiovascular CT and MR: Impact in Brazil and in the World
Arq Bras Cardiol. 2014; 103(5):362-367
Figure 1 – Number of publications in the Arquivos Brasileiros de Cardiologia with exclusive focus on cardiovascular computed tomography and magnetic resonance.
25
20
15
10
5
0
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
2012
2014
Computed Tomography and Magnetic Resonance*
* Pubmed acesso no dia 06/10/2014 utilizando Termos: computed tomography[Title/Abstract], magnetic resonance[Title/Abstract] ANDArquivos Brasileiros de Cardiologia [Journal]� �
Figure 2 – Number of publications in PubMed with exclusive focus on cardiovascular computed tomography and magnetic resonance.
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
2012
2014
1986
1984
1982
1980
1976
1978
2500
2000
1500
1000
500
0
* Pubmed acesso no dia 06/10/2014 utilizando os MeSH Termo: computed tomography AND cardiac
A Cardiac Computed Tomography*
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
2012
2014
1986
1984
1982
1980
1976
1978
1974
1972
1970
1968
1966
1964
2500
2000
1500
1000
500
0
** Pubmed acesso no dia 06/10/2014 utilizando os MeSH Termo: magnetic resonance spectroscopiesAND magnetic imaging AND cardiac
B Cardiac Magnetic Resonance**
an increasing number of private institutions and university hospitals are strengthening teaching and research in the area. Many who are currently in charge of the specialized centers in Brazil sought their expertises in international centers and we believe that in the near future this reality will no longer be true, since we will have large groups throughout the country.
Worldwide Impact of the Latest Publications by Brazilians
The increasing group of people involved in cardiovascular imaging in Brazil and in the world culminated in an explosion of publications dedicated to standardization and proper use of the method over the last years14-31.
Some pioneering work of great international impact has been elaborated by Brazilians and we managed, through this editorial, to draw attention to each one in their area.
- Computed TomographyAssessment of the coronaries – The study conducted
by Miller et al32 had one of the highest scientific impact and collaboration of three Brazilians, one of which was the principal investigator, and also had the largest number of patients included in the study by a Brazilian center. Published in The New England Journal of Medicine, the authors concluded that computed tomography can identify the presence and severity of coronary artery disease with good accuracy, but when positive, could not replace conventional coronary angiography. Recently, tomography showed its value in patients with acute coronary syndrome33.
Assessment of myocardial perfusion – The studies by Cury et al34 , first published in Radiology, brought a new proposal for the use of computed tomography in the evaluation of myocardial ischemia. With simple protocols and easy clinical applicability, it managed to demonstrate that myocardial perfusion on
363

Editorial
Nacif & RochitteCardiovascular CT and MR: Impact in Brazil and in the World
Arq Bras Cardiol. 2014; 103(5):362-367
computed tomography has good correlation with SPECT and with conventional coronary angiography in identifying stenosis of native vessels35 or with stent36. The first multicenter study validating this new technique to detect myocardial ischemia was recently published by Rochitte et al37. This study reported high accuracy for detecting meaningful stenoses associated with perfusion defects in the same territory evaluated by tomography when compared with the combination of invasive catheterization with SPECT scintigraphy, and with a lower cost of radiation dose. Thus, this new method is able to diagnose hemodynamically meaningful stenoses or those associate with a reduction of myocardial blood flow.
Evaluation of volumes and function – The quantification of ventricular volumes and function has been validated against other methods of great clinical applicability38,39, but recently the use of these measurements demonstrated a great potential for detection of cardiovascular risk and mortality40.
Evaluation of focal fibrosis – In studies by Shiozaki et al41,42 we can observe that, in addition to the ability to detect focal fibrosis, tomography can be used to predict ventricular arrhythmias. This field is of great importance because some patients are unable to undergo magnetic resonance and can benefit with this new technique.
Evaluation of interstitial fibrosis – In quantifying interstitial fibrosis by computed tomography, the studies by Nacif et al43,44 were pioneers and open a potential for evaluating subclinical myocardial damage not previously possible in the context of cardiomyopathies.
Epidemiological impact – The studies by Bittencourt et al45,46 demonstrated the prognostic potential of computed tomography in symptomatic patients with nonobstructive and obstructive coronary disease. However, Prazeres et al47 were able to summarize in an unique way the potential of the technique for use in the emergency room, with potential of cost reduction for low-probability patients.
- Magnetic ResonanceAssessment of the coronaries –Evaluation of the coronary
arteries by magnetic resonance is currently limited to the characterization of the origin or evaluation of the proximal thirds of the main vessels. Recently, new techniques and use of specific vascular contrast created a new horizon for implementation of this method which is free of ionizing radiation. Nacif et al48 demonstrated that the intravenous contrast medium Gadofosveset trisodium had a slightly better performance than the contrast media routinely used.
Assessment of myocardial perfusion – Since the initial studies on the characterization of microvascular obstruction by Rochitte et al49 in 1998, until the clinical applicability of the evaluation of myocardial ischemia by Cury et al50 in 2006, and the use of multimodal (combined) resonance techniques for characterization of coronary artery disease by de Mello et al51 in 2012, we are able to observe the current maturity of the method in the country.
Evaluation of volumes and function – After years using indexing and morphological, volumetric and functional values of international studies, we can say that in a pioneer way, Macedo et al52 were able to demonstrate in a Brazilian population different morphological and volumetric standards for men and women. Nacif et al53 demonstrated that there are several ways to quantify atrial volume and that all correlate with one another.
Evaluation of iron deposits – The studies by Fernandes et al54-56 are of great importance for standardization and evaluation of patients with hepatic and myocardial iron storage.
Evaluation of focal fibrosis – In this topic of publications, there are countless contributions by Brazilians in the impact of the method worldwide, but without a doubt one of the most discussed was the study by Azevedo et al57 who were able to demonstrate the importance of detection and quantification of delayed myocardial enhancement in patients who underwent aortic valve replacement with great implication in left ventricular functional improvement and evaluation of mortality.
Evaluation of interstitial fibrosis – The studies by Mongeon et al58, Coelho-Filho et al59, Nacif et al44, Sibley et al60 and Liu et al61 were pioneers in the evaluation of interstitial fibrosis by techniques of T1 map and quantification of extracellular volume.
Epidemiological impact – Without a doubt, magnetic resonance is one of the best methods for quantification of myocardial fibrosis. When present, myocardial fibrosis is associated with increased mortality and worse prognosis62. In Brazil, in addition to the diseases commonly evaluated in the world, we have Chagas disease that was very well studied by Rochitte et al63,64. Now, one of the studies with a major impact on clinical decision using the method was in the risk reclassification using stressor agents65.
Impact of the Latest Publications in the Arquivos Brasileiros de Cardiologia
The Arquivos Brasileiros de Cardiologia function as a national thermometer and a main scientific channel reflecting this explosion of publications. The article by Duarte66, published in 2010, clearly demonstrates the growth of computed tomography and its impact on the detection of coronary artery disease. Over the past decade, we observed an increasing number of review articles67-75 and original articles47,52,76-90, which reinforces the impact of tomography and magnetic resonance in current cardiovascular imaging.
Finally, it is not possible to include all studies by Brazilian authors due to the increasing number of publications in the area, but we are sure that we are entering a new era of cardiovascular imaging. The great development of technology applied to medicine causes computed tomography and magnetic resonance to grow increasingly, changing day-to-day the impact on clinical practice.
364

Editorial
Nacif & RochitteCardiovascular CT and MR: Impact in Brazil and in the World
Arq Bras Cardiol. 2014; 103(5):362-367
1. Stolf NA, Moreira FA, Beyruti R. [Myxoma of the left atrium: the value of computerized tomography in its diagnosis]. Arq Bras Cardiol. 1982;38(2):125-9.
2. de Medeiros Sobrinho JH, Luiz C, Santos DL, da Silva MV, Fontes VF. [Radiological archway sign in the scimitar syndrome and its importance in surgery. Report of 3 cases]. Arq Bras Cardiol. 1983;41(2):125-30.
3. Brito JC, Ribeiro AC, Carvalho HG, Tadeu E, Nery AC, Eloy R, Ribeiro NA. [The scimitar syndrome. Report of 7 cases]. Arq Bras Cardiol. 1984;42(2):139-43.
4. Araujo JA, Torres JM, de Souza Neto JD, Barros RB, da Rocha FA, de Almeida AP. [Difficulties of angiography in the diagnosis of acute aortic dissection. A case report]. Arq Bras Cardiol. 1987;49(1):51-5.
5. Kalil Filho R, Chacra AP, de Albuquerque CP, Soares PR, Antelmi I, Rosemberg L, et al. [Significance of the nuclear magnetic resonance in the detection of coronary artery patency after thrombolysis]. Arq Bras Cardiol. 1995;64(3):221-4.
6. Kalil R, Bocchi EA, Ferreira BM, de Lourdes Higuchi M, Lopes NH, Magalhaes AC, et al. [Magnetic resonance imaging in chronic Chagas cardiopathy. Correlation with endomyocardial biopsy findings]. Arq Bras Cardiol. 1995;65(5):413-6.
7. Pinto IM, da Luz PL, Magalhaes HM, Pavanello R, Abizaid A, Kambara AM, et al. [Consensus SOCESP-SBC on magnetic resonance imaging in cardiology]. Arq Bras Cardiol. 1995;65(5):451-7.
8. Kalil RA, Feldman CJ, Ludwig FW, da Silva AD, Prates PR, Sant’Anna JR, et al. [Late evaluation with spiral computed tomography of smooth bovine pericardium grafts]. Arq Bras Cardiol. 1997;69(2):111-5.
9. Feldman C, Vitola D, Schiavo N. Detection of coronary artery disease based on the calcification index obtained by helical computed tomography. Arq Bras Cardiol. 2000;75(6):471-80.
10. Guidelines for credentialing in cardiovascular magnetic resonance (CMR). Society for Cardiovascular Magnetic Resonance (SCMR) Clinical Practice Committee. J Cardiovasc Magn Reson. 2000;2(3):233-4.
11. Abbara S, Arbab-Zadeh A, Callister TQ, Desai MY, Mamuya W, Thomson L, et al. SCCT guidelines for performance of coronary computed tomographic angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr. 2009;3(3):190-204.
12. Raff GL, Abidov A, Achenbach S, Berman DS, Boxt LM, Budoff MJ, et al; Society of Cardiovascular Computed Tomography. SCCT guidelines for the interpretation and reporting of coronary computed tomographic angiography. J Cardiovasc Comput Tomogr. 2009;3(2):122-36.
13. Sociedade Brasileira de Cardiologia. Departamento de Cardiologia Clínica. Grupo de Estudos de Ressonância e Tomografia Cardiovascular (GERT). [Guideline of Sociedade Brasileira de Cardiologia for Resonance and cardiovascular tomography. Executive Summary]. Arq Bras Cardiol. 2006;87 Suppl 3:e1-12.
14. Hendel RC, Patel MR, Kramer CM, Poon M, Hendel RC, Carr JC, et al; American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group; American College of Radiology;Society of Cardiovascular Computed Tomography; Society for Cardiovascular Magnetic Resonance; American Society of Nuclear Cardiology; North American Society for Cardiac Imaging; Society for Cardiovascular Angiography and Interventions; Society of Interventional Radiology. ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol. 2006;48(7):1475-97.
15. Taylor AJ, Cerqueira M, Hodgson JM, Mark D, Min J, O’Gara P, et al; American College of Cardiology Foundation Appropriate Use Criteria Task Force; Society of Cardiovascular Computed Tomography; American College of Radiology; American Heart Association; American Society of Echocardiography; American Society of Nuclear Cardiology; North American Society for Cardiovascular Imaging; Society for Cardiovascular Angiography and Interventions; Society for Cardiovascular Magnetic Resonance. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 Appropriate Use Criteria for Cardiac Computed Tomography. A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. Circulation. 2010;122(21):e525-55.
16. Patel MR, White RD, Abbara S, Bluemke DA, Herfkens RJ, Picard M, et al; American College of Radiology Appropriateness Criteria Committee; American College of Cardiology Foundation Appropriate Use Criteria Task Force. 2013 ACCF/ACR/ASE/ASNC/SCCT/SCMR appropriate utilization of cardiovascular imaging in heart failure: a joint report of the American College of Radiology Appropriateness Criteria Committee and the American College of Cardiology Foundation Appropriate Use Criteria Task Force. J Am Coll Cardiol. 2013;61(21):2207-31.
17. Russo AM, Stainback RF, Bailey SR, Epstein AE, Heidenreich PA, Jessup M, et al. ACCF/HRS/AHA/ASE/HFSA/SCAI/SCCT/SCMR 2013 appropriate use criteria for implantable cardioverter-defibrillators and cardiac resynchronization therapy: a report of the American College of Cardiology Foundation appropriate use criteria task force, Heart Rhythm Society, American Heart Association, American Society of Echocardiography, Heart Failure Society of America, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance. Heart Rhythm. 2013;10(4):e11-58.
18. White RD, Patel MR, Abbara S, Bluemke DA, Herfkens RJ, Picard M, et al; American College of Radiology; American College of Cardiology Foundation. 2013 ACCF/ACR/ASE/ASNC/SCCT/SCMR appropriate utilization of cardiovascular imaging in heart failure: an executive summary: a joint report of the ACR Appropriateness Criteria (R) Committee and the ACCF Appropriate Use Criteria Task Force. J Am Coll Radiol. 2013;10(7):493-500.
19. Mark DB, Anderson JL, Brinker JA, Brophy JA, Casey DE Jr, Cross RR, et al. ACC/AHA/ASE/ASNC/HRS/IAC/Mended Hearts/NASCI/RSNA/SAIP/SCAI/SCCT/SCMR/SNMMI 2014 health policy statement on use of noninvasive cardiovascular imaging: a report of the American College of Cardiology Clinical Quality Committee. J Am Coll Cardiol. 2014;63(7):698-721.
20. Wolk MJ, Bailey SR, Doherty JU, Douglas PS, Hendel RC, Kramer CM, et al; American College of Cardiology Foundation Appropriate Use Criteria Task Force. ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS 2013 multimodality appropriate use criteria for the detection and risk assessment of stable ischemic heart disease: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2014;63(4):380-406.
21. Mark DB, Berman DS, Budoff MJ, Carr JJ, Gerber TC, Hecht HS, et al; American College of Cardiology Foundation Task Force on Expert Consensus Documents. ACCF/ACR/AHA/NASCI/SAIP/SCAI/SCCT 2010 expert consensus document on coronary computed tomographic angiography: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. Catheter Cardiovasc Interv. 2010;76(2):E1-42.
22. Halliburton SS, Abbara S, Chen MY, Gentry R, Mahesh M, Raff GL, et al; Society of Cardiovascular Computed Tomography. SCCT guidelines on radiation dose and dose-optimization strategies in cardiovascular CT. J Cardiovasc Comput Tomogr. 2011;5(4):198-224.
References
365

Editorial
Nacif & RochitteCardiovascular CT and MR: Impact in Brazil and in the World
Arq Bras Cardiol. 2014; 103(5):362-367
23. Achenbach S, Delgado V, Hausleiter J, Schoenhagen P, Min JK, Leipsic JA. SCCT expert consensus document on computed tomography imaging before transcatheter aortic valve implantation (TAVI)/transcatheter aortic valve replacement (TAVR). J Cardiovasc Comput Tomogr. 2012;6(6):366-80.
24. Patel MR, Dehmer GJ, Hirshfeld JW, Smith PK, Spertus JA. ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT 2012 Appropriate use criteria for coronary revascularization focused update: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. 2012;59(9):857-81. Erratum in: J Am Coll Cardiol. 2012;59(14):1336.
25. Lesser JR. SCCT International Regional Committees: the best future option for appropriate CT utilization. J Cardiovasc Comput Tomogr. 2013;7(2):145-6.
26. Leipsic J, Abbara S, Achenbach S, Cury R, Earls JP, Mancini GJ, et al. SCCT guidelines for the interpretation and reporting of coronary CT angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr. 2014;8(5):342-58.
27. Raff GL, Chinnaiyan KM, Cury RC, Garcia MT, Hecht HS, Hollander JE, et al. SCCT guidelines on the use of coronary computed tomographic angiography for patients presenting with acute chest pain to the emergency department: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr. 2014;8(4):254-71.
28. Hundley WG, Bluemke DA, Finn JP, Flamm SD, Fogel MA, Friedrich MG, et al; American College of Cardiology Foundation Task Force on Expert Consensus Documents. ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents. J Am Coll Cardiol. 2010;55(23):2614-62.
29. Fratz S, Chung T, Greil GF, Samyn MM, Taylor AM, Valsangiacomo Buechel ER, et al. Guidelines and protocols for cardiovascular magnetic resonance in children and adults with congenital heart disease: SCMR expert consensus group on congenital heart disease. J Cardiovasc Magn Reson. 2013;15:51.
30. Moon JC, Messroghli DR, Kellman P, Piechnik SK, Robson MD, Ugander M, et al; Society for Cardiovascular Magnetic Resonance Imaging; Cardiovascular Magnetic Resonance Working Group of the European Society of Cardiology. Myocardial T1 mapping and extracellular volume quantification: a Society for Cardiovascular Magnetic Resonance (SCMR) and CMR Working Group of the European Society of Cardiology consensus statement. J Cardiovasc Magn Reson. 2013;15:92.
31. Schulz-Menger J, Bluemke DA, Bremerich J, Flamm SD, Fogel MA, Friedrich MG, et al. Standardized image interpretation and post processing in cardiovascular magnetic resonance: Society for Cardiovascular Magnetic Resonance (SCMR) board of trustees task force on standardized post processing. J Cardiovasc Magn Reson. 2013;15:35.
32. Miller JM, Rochitte CE, Dewey M, Arbab-Zadeh A, Niinuma H, Gottlieb I, et al. Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med. 2008;359(22):2324-36.
33. Sara L, Rochitte CE, Lemos PA, Niinuma H, Dewey M, Shapiro EP, et al. Accuracy of multidetector computed tomography for detection of coronary artery stenosis in acute coronary syndrome compared with stable coronary disease: a CORE64 multicenter trial substudy. Int J Cardiol. 2014 Aug 27. [Epub ahead of print].
34. Cury RC, Nieman K, Shapiro MD, Butler J, Nomura CH, Ferencik M, et al. Comprehensive assessment of myocardial perfusion defects, regional wall motion, and left ventricular function by using 64-section multidetector CT. Radiology. 2008;248(2):466-75.
35. Cury RC, Magalhaes TA, Paladino AT, Shiozaki AA, Perini M, Senra T, et al. Dipyridamole stress and rest transmural myocardial perfusion ratio evaluation by 64 detector-row computed tomography. J Cardiovasc Comput Tomogr. 2011;5(6):443-8.
36. Magalhaes TA, Cury RC, Pereira AC, Moreira Vde M, Lemos PA, Kalil-Filho R, et al. Additional value of dipyridamole stress myocardial perfusion by 64-row computed tomography in patients with coronary stents. J Cardiovasc Comput Tomogr. 2011;5(6):449-58.
37. Rochitte CE, George RT, Chen MY, Arbab-Zadeh A, Dewey M, Miller JM, et al. Computed tomography angiography and perfusion to assess coronary artery stenosis causing perfusion defects by single photon emission computed tomography: the CORE320 study. Eur Heart J. 2014;35(17):1120-30.
38. Vieira ML, Nomura CH, Tranchesi Junior B, Oliveira WA, Naccarato G, Serpa BS, et al. Left ventricular ejection fraction and volumes as measured by 3d echocardiography and ultrafast computed tomography. Arq Bras Cardiol. 2009;92(4):294-301.
39. Vieira ML, Nomura CH, Tranchesi B Jr, de Oliveira WA, Naccarato G, Serpa BS, et al. Real-time three-dimensional echocardiographic left ventricular systolic assessment: side-by-side comparison with 64-slice multi-detector cardiac computed tomography. Eur J Echocardiogr. 2010;11(3):257-63.
40. Arsanjani R, Berman DS, Gransar H, Cheng VY, Dunning A, Lin FY, et al; CONFIRM Investigators. Left ventricular function and volume with coronary CT angiography improves risk stratification and identification of patients at risk for incident mortality: results from 7758 patients in the prospective multinational CONFIRM observational cohort study. Radiology. 2014;273(1):70-7.
41. Shiozaki AA, Senra T, Arteaga E, Martinelli Filho M, Pita CG, Avila LF, et al. Myocardial fibrosis detected by cardiac CT predicts ventricular fibrillation/ventricular tachycardia events in patients with hypertrophic cardiomyopathy. J Cardiovasc Comput Tomogr. 2013;7(3):173-81.
42. Shiozaki AA, Senra T, Arteaga E, Pita CG, Martinelli Filho M, Avila LF, et al. [Myocardial fibrosis in patients with hypertrophic cardiomyopathy and high risk for sudden death]. Arq Bras Cardiol. 2010;94(4):535-40.
43. Nacif MS, Liu Y, Yao J, Liu S, Sibley CT, Summers RM, et al. 3D left ventricular extracellular volume fraction by low-radiation dose cardiac CT: assessment of interstitial myocardial fibrosis. J Cardiovasc Comput Tomogr. 2013;7(1):51-7.
44. Nacif MS, Kawel N, Lee JJ, Chen X, Yao J, Zavodni A, et al. Interstitial myocardial fibrosis assessed as extracellular volume fraction with low-radiation-dose cardiac CT. Radiology. 2012;264(3):876-83.
45. Bittencourt MS, Hulten E, Ghoshhajra B, O’Leary D, Christman MP, Montana P, et al. Prognostic value of nonobstructive and obstructive coronary artery disease detected by coronary computed tomography angiography to identify cardiovascular events. Circ Cardiovasc Imaging. 2014;7(2):282-91.
46. Hulten E, Bittencourt MS, Ghoshhajra B, O’Leary D, Christman MP, Blaha MJ, et al. Incremental prognostic value of coronary artery calcium score versus CT angiography among symptomatic patients without known coronary artery disease. Atherosclerosis. 2014;233(1):190-5.
47. Prazeres CE, Cury RC, Carneiro AC, Rochitte CE. Coronary computed tomography angiography in the assessment of acute chest pain in the emergency room. Arq Bras Cardiol. 2013;101(6):562-9.
48. Raman FS, Nacif MS, Cater G, Gai N, Jones J, Li D, et al. 3.0-T whole-heart coronary magnetic resonance angiography: comparison of gadobenate dimeglumine and gadofosveset trisodium. Int J Cardiovasc Imaging. 2013;29(5):1085-94.
49. Rochitte CE, Lima JA, Bluemke DA, Reeder SB, McVeigh ER, Furuta T, et al. Magnitude and time course of microvascular obstruction and tissue injury after acute myocardial infarction. Circulation. 1998;98(10):1006-14.
50. Cury RC, Cattani CA, Gabure LA, Racy DJ, de Gois JM, Siebert U, et al. Diagnostic performance of stress perfusion and delayed-enhancement MR imaging in patients with coronary artery disease. Radiology. 2006;240(1):39-45.
51. de Mello RA, Nacif MS, dos Santos AA, Cury RC, Rochitte CE, Marchiori E. Diagnostic performance of combined cardiac MRI for detection of coronary artery disease. Eur J Radiol. 2012;81(8):1782-9.
52. Macedo R, Fernandes JL, Andrade SS, Rochitte CE, Lima KC, Maciel AC, et al. Morphological and functional measurements of the heart obtained by magnetic resonance imaging in Brazilians. Arq Bras Cardiol. 2013;101(1):68-77.
366

Editorial
Nacif & RochitteCardiovascular CT and MR: Impact in Brazil and in the World
Arq Bras Cardiol. 2014; 103(5):362-367
53. Nacif MS, Barranhas AD, Turkbey E, Marchiori E, Kawel N, Mello RA, et al. Left atrial volume quantification using cardiac MRI in atrial fibrillation: comparison of the Simpson’s method with biplane area-length, ellipse, and three-dimensional methods. Diagn Interv Radiol. 2013;19(3):213-20.
54. Fernandes JL, Fabron A Jr, Verissimo M. Early cardiac iron overload in children with transfusion-dependent anemias. Haematologica. 2009;94(12):1776-7.
55. Fernandes JL, Sampaio EF, Fertrin K, Coelho OR, Loggetto S, Piga A, et al. Amlodipine reduces cardiac iron overload in patients with thalassemia major: a pilot trial. Am J Med. 2013;126(9):834-7.
56. Fernandes JL, Sampaio EF, Verissimo M, Pereira FB, da Silva JA, de Figueiredo GS, et al. Heart and liver T2 assessment for iron overload using different software programs. Eur Radiol. 2011;21(12):2503-10.
57. Azevedo CF, Nigri M, Higuchi ML, Pomerantzeff PM, Spina GS, Sampaio RO, et al. Prognostic significance of myocardial fibrosis quantification by histopathology and magnetic resonance imaging in patients with severe aortic valve disease. J Am Coll Cardiol. 2010;56(4):278-87.
58. Mongeon FP, Jerosch-Herold M, Coelho-Filho OR, Blankstein R, Falk RH, Kwong RY. Quantification of extracellular matrix expansion by CMR in infiltrative heart disease. JACC Cardiovasc Imaging. 2012;5(9):897-907.
59. Coelho-Filho OR, Shah RV, Neilan TG, Mitchell R, Moreno H Jr, Kwong R, et al. Cardiac magnetic resonance assessment of interstitial myocardial fibrosis and cardiomyocyte hypertrophy in hypertensive mice treated with spironolactone. J Am Heart Assoc. 2014;3(3):e000790.
60. Sibley CT, Noureldin RA, Gai N, Nacif MS, Liu S, Turkbey EB, et al. T1 Mapping in cardiomyopathy at cardiac MR: comparison with endomyocardial biopsy. Radiology. 2012;265(3):724-32.
61. Liu CY, Liu YC, Wu C, Armstrong A, Volpe GJ, van der Geest RJ, et al. Evaluation of age-related interstitial myocardial fibrosis with cardiac magnetic resonance contrast-enhanced T1 mapping: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol. 2013;62(14):1280-7.
62. Neilan TG, Shah RV, Abbasi SA, Farhad H, Groarke JD, Dodson JA, et al. The incidence, pattern, and prognostic value of left ventricular myocardial scar by late gadolinium enhancement in patients with atrial fibrillation. J Am Coll Cardiol. 2013;62(23):2205-14.
63. Rochitte CE, Oliveira PF, Andrade JM, Ianni BM, Parga JR, Avila LF, et al. Myocardial delayed enhancement by magnetic resonance imaging in patients with Chagas’ disease: a marker of disease severity. J Am Coll Cardiol. 2005;46(8):1553-8.
64. Rochitte CE, Nacif MS, de Oliveira Junior AC, Siqueira-Batista R, Marchiori E, Uellendahl M, et al. Cardiac magnetic resonance in Chagas’ disease. Artif Organs. 2007;31(4):259-67.
65. Shah R, Heydari B, Coelho-Filho O, Murthy VL, Abbasi S, Feng JH, et al. Stress cardiac magnetic resonance imaging provides effective cardiac risk reclassification in patients with known or suspected stable coronary artery disease. Circulation. 2013;128(6):605-14.
66. Duarte PS. Technologies for the investigation of CAD: association between scientific publications and clinical use. Arq Bras Cardiol. 2010;94(3):379-82, 401-5.
67. Bertaso AG, Bertol D, Duncan BB, Foppa M. Epicardial fat: definition, measurements and systematic review of main outcomes. Arq Bras Cardiol. 2013;101(1):e18-28.
68. Rodrigues AR, Barbosa MR, de Brito MS, Silva LC, Machado FS. [Minimally invasive coronary angiography using a multidetector CT]. Arq Bras Cardiol. 2006;86(5):323-30.
69. Piva e Mattos B, Torres MA, Rebelatto TF, Loreto MS, Scolari FL. The diagnosis of left ventricular outflow tract obstruction in hypertrophic cardiomyopathy. Arq Bras Cardiol. 2012;99(1):665-75.
70. Rosa LV, Salemi VM, Alexandre LM, Mady C. Noncompaction cardiomyopathy: a current view. Arq Bras Cardiol. 2011;97(1):e13-9.
71. Nacif MS, Oliveira Junior AC, Carvalho AC, Rochitte CE. Cardiac magnetic resonance and its anatomical planes: how do I do it? Arq Bras Cardiol. 2010;95(6):756-63.
72. Mattos BP, Torres MA, Freitas VC. Diagnostic evaluation of hypertrophic cardiomyopathy in its clinical and preclinical phases. Arq Bras Cardiol. 2008;91(1):51-62.
73. Nigri M, Rochitte CE, Tarasoutchi F, Grinberg M. Magnetic resonance imaging is image diagnosis in heart valve disease. Arq Bras Cardiol. 2006;87(4):534-7.
74. Dias RR, Fernandes F, Ramires FJ, Mady C, Albuquerque CP, Jatene FB. Mortality and embolic potential of cardiac tumors. Arq Bras Cardiol. 2014;103(1):13-8.
75. Rajani R, Khattar R, Chiribiri A, Victor K, Chambers J. Multimodality imaging of heart valve disease. Arq Bras Cardiol. 2014;103(3):251-63.
76. Tassi EM, Continentino MA, Nascimento EM, Pereira Bde B, Pedrosa RC. Relationship between fibrosis and ventricular arrhythmias in Chagas heart disease without ventricular dysfunction. Arq Bras Cardiol. 2014;102(5):456-64.
77. Rochitte CE, Hoette S, Souza R. Myocardial delayed enhancement by cardiac magnetic resonance imaging in Pulmonary Arterial Hypertension: a marker of disease severity. Arq Bras Cardiol. 2013;101(5):377-8.
78. Bessa LG, Junqueira FP, Bandeira ML, Garcia MI, Xavier SS, Lavall G, et al. Pulmonary arterial hypertension: use of delayed contrast-enhanced cardiovascular magnetic resonance in risk assessment. Arq Bras Cardiol. 2013;101(4):336-43.
79. Fernandes AM, Rathi V, Biederman RW, Doyle M, Yamrozik JA, Willians RB, et al. Cardiovascular magnetic resonance imaging-derived mitral valve geometry in determining mitral regurgitation severity. Arq Bras Cardiol. 2013;100(6):571-8.
80. Villacorta Junior H, Villacorta AS, Amador F, Hadlich M, Albuquerque DC, Azevedo CF. Transthoracic impedance compared to magnetic resonance imaging in the assessment of cardiac output. Arq Bras Cardiol. 2012;99(6):1149-55.
81. Mello RP, Szarf G, Schvartzman PR, Nakano EM, Espinosa MM, Szejnfeld D, et al. Delayed enhancement cardiac magnetic resonance imaging can identify the risk for ventricular tachycardia in chronic Chagas’ heart disease. Arq Bras Cardiol. 2012;98(5):421-30.
82. Moreira Rde C, Haddad AF, Silva SA, Souza AL, Tuche FA, Oliveira MA, et al. Intracoronary stem-cell injection after myocardial infarction: microcirculation sub-study. Arq Bras Cardiol. 2011;97(5):420-6.
83. Efe D, Aygun F. Assessment of the relationship between non-alcoholic fatty liver disease and CAD using MSCT. Arq Bras Cardiol. 2014;102(1):10-8.
84. Staniak HL, Sharovsky R, Pereira AC, Castro CC, Bensenor IM, Lotufo PA, et al. Subcutaneous tissue thickness is an independent predictor of image noise in cardiac CT. Arq Bras Cardiol. 2014;102(1):86-92.
85. Azevedo JC, Ferreira Junior Dde S, Vieira FC, Prezotti LS, Simoes LS, Nacif MS, et al. Correlation between myocardial scintigraphy and CT angiography in the evaluation of coronary disease. Arq Bras Cardiol. 2013;100(3):238-45.
86. Staniak HL, Bittencourt MS, Sharovsky R, Bensenor I, Olmos RD, Lotufo PA. Calcium score to evaluate chest pain in the emergency room. Arq Bras Cardiol. 2013;100(1):90-3.
87. Barros MV, Rabelo DR, Nunes Mdo C, Siqueira MH. Coronary tomography for predicting adverse events in patients with suspected coronary disease. Arq Bras Cardiol. 2012;99(6):1142-8.
88. Hadlich MS, Oliveira GM, Feijoo RA, Azevedo CF, Tura BR, Ziemer PG, et al. Free and open-source software application for the evaluation of coronary computed tomography angiography images. Arq Bras Cardiol. 2012;99(4):944-51.
89. Rochitte CE, Azevedo GS, Shiozaki AA, Azevedo CF, Kalil Filho R. Diltiazem as an alternative to beta-blocker in coronary artery computed tomography angiography. Arq Bras Cardiol. 2012;99(2):706-13.
90. Rabelo DR, Barros MV, Nunes Mdo C, Oliveira CC, Siqueira MH. Multislice coronary angiotomography in the assessment of coronary artery anomalous origin. Arq Bras Cardiol. 2012;98(3):266-72.
367

Original Article
Sleep Apnea and Nocturnal Cardiac Arrhythmia: A Populational StudyFatima Dumas Cintra, Renata Pimentel Leite, Luciana Julio Storti, Lia Azeredo Bittencourt, Dalva Poyares, Laura de Siqueira Castro, Sergio Tufik, Angelo de PaolaUniversidade Federal de São Paulo - Unifesp, São Paulo, SP − Brazil
Mailing Address: Fatima Dumas Cintra •Alameda Taurus, 146, Residencial Genesis I, Alphaville. Postal Code 06543-670. Santana de Parnaíba, SP – BrazilE-mail: [email protected]; [email protected] received December 6, 2013; revised manuscript June 26, 2014; accepted July 4, 2014
DOI: 10.5935/abc.20140142
AbstractBackground: The mechanisms associated with the cardiovascular consequences of obstructive sleep apnea include abrupt changes in autonomic tone, which can trigger cardiac arrhythmias. The authors hypothesized that nocturnal cardiac arrhythmia occurs more frequently in patients with obstructive sleep apnea.
Objective: To analyze the relationship between obstructive sleep apnea and abnormal heart rhythm during sleep in a population sample.
Methods: Cross-sectional study with 1,101 volunteers, who form a representative sample of the city of São Paulo. The overnight polysomnography was performed using an EMBLA® S7000 digital system during the regular sleep schedule of the individual. The electrocardiogram channel was extracted, duplicated, and then analyzed using a Holter (Cardio Smart®) system.
Results: A total of 767 participants (461 men) with a mean age of 42.00 ± 0.53 years, were included in the analysis. At least one type of nocturnal cardiac rhythm disturbance (atrial/ventricular arrhythmia or beat) was observed in 62.7% of the sample. The occurrence of nocturnal cardiac arrhythmias was more frequent with increased disease severity. Rhythm disturbance was observed in 53.3% of the sample without breathing sleep disorders, whereas 92.3% of patients with severe obstructive sleep apnea showed cardiac arrhythmia. Isolated atrial and ventricular ectopy was more frequent in patients with moderate/severe obstructive sleep apnea when compared to controls (p < 0.001). After controlling for potential confounding factors, age, sex and apnea-hypopnea index were associated with nocturnal cardiac arrhythmia.
Conclusion: Nocturnal cardiac arrhythmia occurs more frequently in patients with obstructive sleep apnea and the prevalence increases with disease severity. Age, sex, and the Apnea-hypopnea index were predictors of arrhythmia in this sample. (Arq Bras Cardiol. 2014; 103(5):368-374)
Keywords: Sleep Apnea Syndromes; Arrhythmias, Cardiac; Sleep; Sleep Apnea, Obstructive.
IntroductionObstructive sleep apnea (OSA) is characterized by
sleep fragmentation1 and repetitive hypoxia2 during sleep. OSA is associated with a number of cardiovascular effects, such as hypertension3,4, metabolic syndrome5, and heart failure6. OSA was recently associated with increased cardiovascular mortality7,8; however, the identification of the abnormality and the institution of effective treatment with continuous positive airway pressure (CPAP) reduce the rate of fatal and nonfatal cardiovascular events7.
The mechanisms responsible for cardiovascular damage secondary to the obstructive apnea events are multiple,
but the final common pathway is autonomic involvement9. Intermittent hypoxia10, sleep fragmentation11, and alterations in intrapleural pressure12 directly affect the sympathetic and parasympathetic autonomic nervous system.
Moreover, cardiac arrhythmia may be triggered by changes in the autonomic tone13. The vagal activity may cause bradyarrhythmias, and sympathetic overactivity may favor various rhythm disturbances, including ventricular arrhythmias. The authors of this manuscript hypothesized that nocturnal cardiac arrhythmia occurs more frequently in patients with OSA. Hence, the aim of this study was to analyze the relationship between such arrhythmias and abnormal heart rhythm during sleep in a population sample.
Methods
Study populationCross-sectional study involving 101 volunteers in a single
center was conducted. The sample size was defined to allow prevalence estimates with 3% accuracy14. To obtain a representative sample of the inhabitants of Sao Paulo,
368

Original Article
Cintra et al.Sleep and Cardiac Arrhythmia
Arq Bras Cardiol. 2014; 103(5):368-374
a technique of three-stage cluster sampling was used15. In the first stage, to ensure accurate socioeconomic representation, 96 of the 1,500 districts of the city used by the Brazilian Geography and Statistics Institute (IBGE) were proportionally selected among four homogeneous socioeconomic regions of Sao Paulo. The selected private households were permanently occupied. Thus, clinics, schools, and other commercial and noncommercial establishments were excluded. In the second stage, the families were selected by randomly selecting a household and subsequently skipping a specified number of houses in relation to the total number of selected households and dividing by a fixed number. Eleven families in each sector were selected in this manner. Each apartment, in the building, was considered a household and was counted from the top to the bottom floor. Finally, in the third sampling stage, all eligible residents in each selected household from the youngest to the oldest were listed. Pregnant or lactating women, people with physical or mental disabilities, individuals under 20 or over 80 years of age, and people who worked every night were excluded from the study. Substitutes were selected from the neighboring house, using the same random selection criteria described above. The rational design, sampling, and procedures used in the Epidemiological Study of Sleep of Sao Paulo have been described in a previous publication16.
The study protocol was approved by the Ethics Committee of the Federal University of Sao Paulo (CEP 0593/06) and registered at ClinicalTrials.gov under number NCT00596713. All volunteers read and signed the proposed consent form.
After signing the consent form, the patients were asked to attend the Sleep Laboratory for clinical evaluation and basal overnight polysomnography (PSG).
PolysomnographyThe overnight PSG was performed in the sleep
laboratory using a digital system (EMBLA® S7000, Embla Systems, Inc., Broomfield, CO, United States) during the regular sleeping hours of the individuals. The following physiological variables were monitored simultaneously and continuously: Electroencephalogram (EEG), electro-oculogram, electromyogram (submental region, tibialis anterior muscle, masseter region, and seventh intercostal space), electrocardiogram (ECG), detection of airflow (thermocouple and nasal pressure), abdominal and thoracic breathing efforts (by inductance plethysmography), snoring, body position, peripheral oxygen saturation (SO2), and heart rate. Four trained technicians visually labeled all the PSGs according to the standard criteria for investigating sleep17. The EEG and leg movements were classified according to the criteria established in the manual of the American Academy of Sleep Medicine (AASM) for assessing sleep and associated events18. Apneas were classified according to rules recommended for adults in the AASM manual, and hypopneas were labeled according to the alternative rules18. A PSG technician randomly selected and reassessed 4% of the PSGs to verify the accuracy of sleep staging (concordance index of 93.3 ± 5.1, Kappa 0.91 ± 0.03). The apnea-hypopnea index (AHI) was used to determine the presence (AHI > 5) and severity of OSA (mild: 5 < AHI < 15; moderate: 15 < AHI < 30; and severe AHI > 30).
Holter evaluation during polysomnographyAn ECG channel was extracted from PSG, duplicated
and then analyzed with a Holter system manufactured by Cardios® (Smart Cardio, Cardio Systems, Sao Paulo, Brazil). The following characteristics of the ECG were analyzed: heart rate, QT and PR intervals, ventricular and atrial arrhythmias, and breaks. The complexity of the arrhythmias was described as follows: isolated, paired, or tachycardia. Anthropometric measurements were performed immediately before PSG and included body weight (kg), height (m), body mass index (BMI), and circumference (cm) of the neck and blood pressure.
Statistical AnalysisVersion 17.0 of the Statistical Package for Social Science
(SPSS) for Windows was used for data analysis. Descriptive statistics were used for the sample and group characteristics. The chi-square test was used to determine associations between subgroups. The general linear models (GLM) were used to analyze some variables. The a posteriori Tukey test was applied when necessary. A final adjustment of the logistic model was performed to analyze the main variables associated with the occurrence of cardiac arrhythmia. Data were expressed as median ± standard error for quantitative variables. Categorical variables are expressed as percentages. A p value ≤ 0.05 was considered statistically significant.
Results A total of 767 participants (461 men) with a mean age of
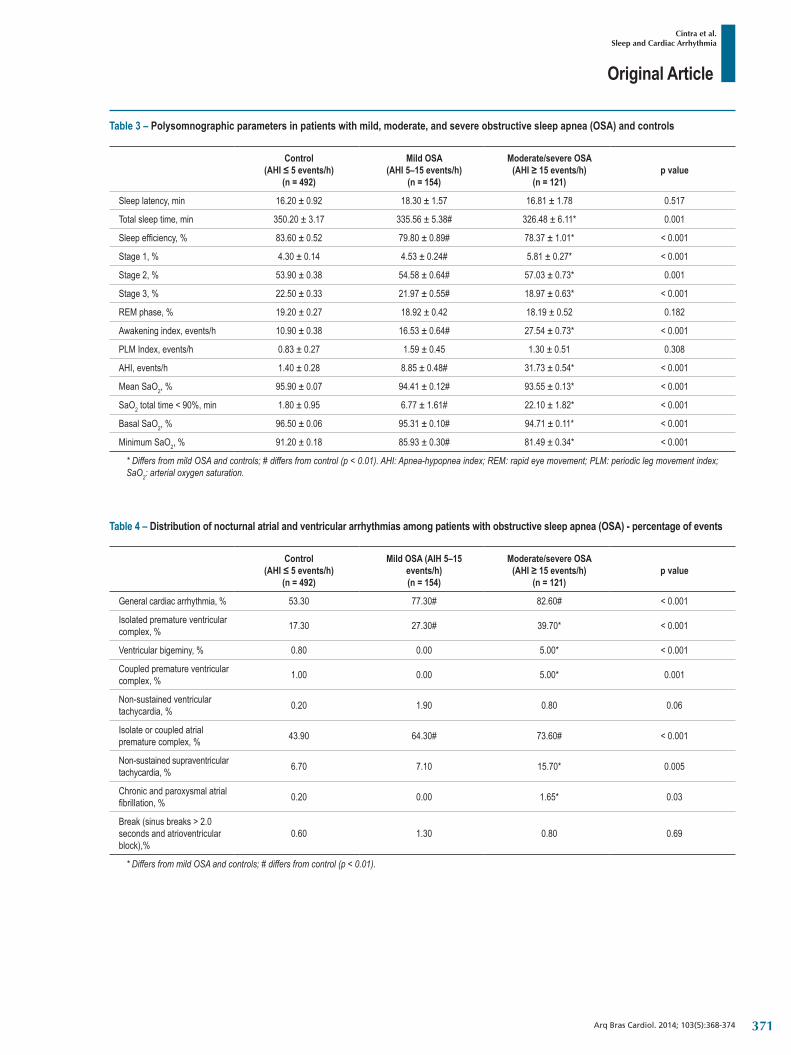
42.00 ± 0.53 years were included in the analysis. The ECG channel extraction and compatibility for the Holter system methods could not be performed in 334 subjects who were excluded from the analysis. The demographic characteristics of the sample are shown in Table 1. The presence of OSA, defined by AHI > 5, was observed in 37% of the population; 55.3% of these cases were classified as mild OSA and 44.7% had moderate or severe disease. The clinical and polysomnographic parameters of the patients with mild, moderate, or severe OSA and of the control group (without OSA) are shown in Tables 2 and 3, respectively. Sleep latency, percentage of REM sleep, and the periodic leg movement index were the only variables that did not reach significance when the groups were compared.
At least one kind of nocturnal cardiac rhythm disturbance (atrial or ventricular arrhythmias and/or break) was observed in 62.7% of the sample. The occurrence of nocturnal cardiac arrhythmias was more frequent with increased disease severity. Rhythm disturbance was observed in 53.3% of subjects without sleep breathing disorders, while 92.3% of patients with severe OSA had cardiac arrhythmia. The distribution of atrial arrhythmias, ventricular arrhythmias, and breaks are shown in Table 4. Both ectopic complexes, isolated from atrial and ventricular arrhythmias, were more frequent in patients with moderate/severe OSA than in controls (p < 0.001). Occurrences of nocturnal breaks and non-sustained ventricular tachycardia did not differ between groups.
369

Original Article
Cintra et al.Sleep and Cardiac Arrhythmia
Arq Bras Cardiol. 2014; 103(5):368-374
After controlling for potential confounder effects (age, BMI, smoking, diabetes, hypertension, and PSG parameters), age, sex, and AHI were independently associated with the occurrence of nocturnal cardiac arrhythmia (Table 5).
DiscussionThe main finding of this study was the demonstration that
nocturnal cardiac rhythm disorders occur more frequently in patients with OSA than in the general population, and that its prevalence increased with disease severity. The relationship between cardiac arrhythmias and sleep breathing disorders was assessed in several previous studies. Guilleminault et al19 using a 24-h Holter monitoring in 400 OSA patients, showed that 48% had nocturnal cardiac events. Olmetti al.20 analyzed an electrocardiographic recording during PSG and found nocturnal cardiac arrhythmia in 18.5% of the 257 consecutively selected patients with OSA.
The result of this study demonstrated that the prevalence of nocturnal cardiac arrhythmia was higher than that
previously described in the literature (92.3% of patients with OSA compared with 53.3% in the general population). Several explanations for this difference are possible. The use of a continuous monitoring system as a tool, with automatic detection of rhythm disturbances (Holter), may have detected the arrhythmias with greater accuracy, when compared with other methodologies used in clinical studies, such as 12-lead electrocardiography and electrocardiographic channel isolated from PSG. Furthermore, 37% of this population had an AHI > 5 events/h. This prevalence was also higher than that observed in other epidemiological studies21, possibly because it included individuals with high BMI and age > 70 years22-24. Finally, the use of a gold standard tool (GST) to detect breathing events during sleep can lead to a more effective screening of the population with OSA; and thus, to a better assessment of the prevalence of nocturnal arrhythmias.
The mechanisms involved in the pathophysiology of cardiac arrhythmias and OSA are probably multifactorial. In this study, we demonstrated that, in addition to age and gender, the AIH
Table 1 – Demographic characteristics of the sample
Characteristics Total (n = 767)
Mean age (years) 42.00 ± 0.53
Male gender (n) 352
Body mass index (kg/m2) 26.60 ± 0.18
Neck circumference (cm) 36.10 ± 0.17
Hypertension (%) 46.30
Diabetes (%) 7.30
Systolic blood pressure (mmHg) 124.40 ± 0.97
Diastolic blood pressure (mmHg) 79.33 ± 0.55
Smoking (%) 23.30
Table 2 – Clinical characteristics of patients with mild, moderate, and severe obstructive sleep apnea (OSA) and controls
Control (AHI ≤ 5 events/h)
n = 492
mild OSA (AHI 5–15 events/h)
n = 154
moderate/severe OSA (AHI ≥ 15 events/h)
n = 121p value
Age, years 37.47 ± 0.52 48.12 ± 0.88# 53.41 ± 1.01* < 0.001
Male gender, n 189 82 81 < 0.001
BMI, kg/m2 25.33 ± 0.20 28.45 ± 0.34# 30.37 ± 0.38* < 0.001
Neck Circumference, cm 35.02 ± 0.22 37.55 ± 0.37# 39.24 ± 0.42* < 0.001
Waist circumference, cm 81.10 ± 0.51 90.65 ± 0.86# 96.29 ± 0.98* < 0.001
Hip circumference, cm 97.79 ± 0.51 103.12 ± 0.85# 105.36 ± 0.97* < 0.001
Waist / hip ratio 0.85 ± 0.01 0.88 ± 0.02# 0.92 ± 0.02* 0.011
SBP, mmHg 118.95 ± 1.06 132.86 ± 1.78# 138.32 ± 2.04* < 0.001
DBP, mmHg 76.61 ± 0.62 83.47 ± 1.05# 84.32 ± 1.20* < 0.001
* Differs from mild OSA and controls; # Differs from the controls (p < 0.01). AHI: apnea-hypopnea index; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure.
370
Original Article
Cintra et al.Sleep and Cardiac Arrhythmia
Arq Bras Cardiol. 2014; 103(5):368-374
Table 3 – Polysomnographic parameters in patients with mild, moderate, and severe obstructive sleep apnea (OSA) and controls
Control (AHI ≤ 5 events/h)
(n = 492)
Mild OSA (AHI 5–15 events/h)
(n = 154)
Moderate/severe OSA (AHI ≥ 15 events/h)
(n = 121)p value
Sleep latency, min 16.20 ± 0.92 18.30 ± 1.57 16.81 ± 1.78 0.517
Total sleep time, min 350.20 ± 3.17 335.56 ± 5.38# 326.48 ± 6.11* 0.001
Sleep efficiency, % 83.60 ± 0.52 79.80 ± 0.89# 78.37 ± 1.01* < 0.001
Stage 1, % 4.30 ± 0.14 4.53 ± 0.24# 5.81 ± 0.27* < 0.001
Stage 2, % 53.90 ± 0.38 54.58 ± 0.64# 57.03 ± 0.73* 0.001
Stage 3, % 22.50 ± 0.33 21.97 ± 0.55# 18.97 ± 0.63* < 0.001
REM phase, % 19.20 ± 0.27 18.92 ± 0.42 18.19 ± 0.52 0.182
Awakening index, events/h 10.90 ± 0.38 16.53 ± 0.64# 27.54 ± 0.73* < 0.001
PLM Index, events/h 0.83 ± 0.27 1.59 ± 0.45 1.30 ± 0.51 0.308
AHI, events/h 1.40 ± 0.28 8.85 ± 0.48# 31.73 ± 0.54* < 0.001
Mean SaO2, % 95.90 ± 0.07 94.41 ± 0.12# 93.55 ± 0.13* < 0.001
SaO2 total time < 90%, min 1.80 ± 0.95 6.77 ± 1.61# 22.10 ± 1.82* < 0.001
Basal SaO2, % 96.50 ± 0.06 95.31 ± 0.10# 94.71 ± 0.11* < 0.001
Minimum SaO2, % 91.20 ± 0.18 85.93 ± 0.30# 81.49 ± 0.34* < 0.001
* Differs from mild OSA and controls; # differs from control (p < 0.01). AHI: Apnea-hypopnea index; REM: rapid eye movement; PLM: periodic leg movement index; SaO2: arterial oxygen saturation.
Table 4 – Distribution of nocturnal atrial and ventricular arrhythmias among patients with obstructive sleep apnea (OSA) - percentage of events
Control(AHI ≤ 5 events/h)
(n = 492)
Mild OSA (AIH 5–15 events/h)(n = 154)
Moderate/severe OSA(AHI ≥ 15 events/h)
(n = 121)p value
General cardiac arrhythmia, % 53.30 77.30# 82.60# < 0.001
Isolated premature ventricular complex, % 17.30 27.30# 39.70* < 0.001
Ventricular bigeminy, % 0.80 0.00 5.00* < 0.001
Coupled premature ventricular complex, % 1.00 0.00 5.00* 0.001
Non-sustained ventricular tachycardia, % 0.20 1.90 0.80 0.06
Isolate or coupled atrial premature complex, % 43.90 64.30# 73.60# < 0.001
Non-sustained supraventricular tachycardia, % 6.70 7.10 15.70* 0.005
Chronic and paroxysmal atrial fibrillation, % 0.20 0.00 1.65* 0.03
Break (sinus breaks > 2.0 seconds and atrioventricular block),%
0.60 1.30 0.80 0.69
* Differs from mild OSA and controls; # differs from control (p < 0.01).
371

Original Article
Cintra et al.Sleep and Cardiac Arrhythmia
Arq Bras Cardiol. 2014; 103(5):368-374
is an important factor related to nocturnal cardiac arrhythmia events. Hypoxia as a result of obstructive events is a potent stimulator for the sympathetic nervous system25. Fluctuations in sympathetic and parasympathetic activity in patients with OSA may predispose them to the development of atrial and ventricular arrhythmias.
Another strong mechanism involved in the pathophysiology of cardiac arrhythmias and OSA is structural heart disease, which could favor the occurrence of cardiac arrhythmia. Oliveira et al26, using three-dimensional echocardiography, showed that OSA induced an overload in the left atrium, resulting in remodeling. In addition, the effective use of CPAP can improve diastolic function of the left ventricle and the passive emptying of the left atrium27. A structural assessment of the heart by echocardiography was not performed in this population, which may be considered a limitation of this study.
We did not observe differences in the occurrence of nocturnal cardiac breaks. Harbison et al28 performed Holter ECG monitoring in 45 patients previously diagnosed with OSA syndrome and observed seven cases of cardiac break nocturnally, which were partially reversed with effective CPAP therapy. However, in randomized clinical trials to evaluate the role of CPAP in cardiac arrhythmias, there was no change after treatment with CPAP29, suggesting that other mechanisms, not limited to apnea, trigger arrhythmia. The relationship between cardiac breaks, obstructive apnea events, and CPAP is still not fully understood and should be further analyzed in subsequent studies.
The absence of information on the occurrence of cardiac arrhythmia during the day and the variability in the frequency of arrhythmias are also limitations of this study, because the results may not accurately reflect the actual severity of rhythm disturbances. However, the correlation between apnea
(observed by PSG) and the occurrence of cardiac arrhythmia (observed by Holter) in a population-based study can provide new insights into the treatment of arrhythmias as well as highlight the need to assess the sleep of these patients.
ConclusionNocturnal cardiac arrhythmias occurred more frequently in
patients with obstructive sleep apnea, and the prevalence increased with disease severity. Age, sex and the apnea-hypopnea index were predictors of nocturnal cardiac arrhythmias in this sample.
Author contributionsConception and design of the research: Cintra FD, Poyares
D; Acquisition of data: Cintra FD, Leite RP, Storti LJ; Analysis and interpretation of the data: Cintra FD; Statistical analysis: Poyares D;Obtaining financing: Poyares D, Tufik S; Writing of the manuscript: Cintra FD, Bittencourt LA, Poyares D; Critical revision of the manuscript for intellectual content: Cintra FD, Leite RP, Bittencourt LA, Poyares D, Tufik S, Paola A.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
This study was funded by FAPESP and AFIP.
Study Association
This study is not associated with any thesis or dissertation work.
Table 5 – Adjusted logistic model of predictors of the occurrence of nocturnal cardiac arrhythmia
Beta p value Prevalence ratio CI 95%
Male gender 0.40 0.032 1.49 1.04 - 2.16
Age 0.06 < 0.001 1.06 1.04 - 1.08
BMI -0.01 0.80 1.00 0.96 - 1.03
Smoking 0.13 0.51 1.14 0.77 - 1.67
Diabetes 0.90 0.08 2.45 0.90 - 6.70
Hypertension -0.24 0.26 0.79 0.53 - 1.19
AHI 0.04 0.007 1.04 1.01 - 1.07
Total time of oxygen saturation < 90% -0.01 0.18 0.99 0.98 - 1.00
Awakening index -0.02 0.19 0.98 0.96 - 1.01
Total time awake after sleep onset 0.00 0.95 1.00 0.99 - 1.01
Total sleep time 0.00 0.15 1.00 1.00 - 1.01
Sleep efficiency -0.02 0.25 0.98 0.94 - 1.02
Constant -0.83 0.62 0.44
CI 95%: 95% confidence interval of; BMI: body mass index; AHI: apnea-hypopnea index.
372
Original Article
Cintra et al.Sleep and Cardiac Arrhythmia
Arq Bras Cardiol. 2014; 103(5):368-374
1. Kimoff RJ. Sleep fragmentation in obstructive sleep apnea. Sleep. 1996;19(9 Suppl):S61-6.
2. Peled N, Greenberg A, Pillar G, Zinder O, Levi N, Lavie P. Contributions of hypoxia and respiratory disturbance index to sympathetic activation and blood pressure in obstructive sleep apnea syndrome. Am J Hypertens. 1998;11(11 Pt 1):1284-9.
3. Nieto FJ, Young TB, Lind BK, Shahar E, Samet JM, Redline S, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study. Sleep Heart Health Study. JAMA. 2000;283(14):1829-36. Erratum in: JAMA. 2002;288(16):1985.
4. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342(19):1378-84.
5. Bonsignore MR, Esquinas C, Barceló A, Sanchez-de-la-Torre M, Paternó A, Duran-Cantolla J, et al. Metabolic syndrome, insulin resistance and sleepiness in real-life obstructive sleep apnoea. Eur Respir J. 2012;39(5):1136-43.
6. Paulino A, Damy T, Margarit L, Stoïca M, Deswarte G, Khouri L, et al. Prevalence of sleep-disordered breathing in a 316-patient French cohort of sTabela congestive heart failure. Arch Cardiovasc Dis. 2009;102(3):169-75.
7. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnea-hypopnea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046-53.
8. Marshall NS, Wong KK, Liu PY, Cullen SR, Knuiman MW, Grunstein RR. Sleep apnea as an independent risk factor for all-cause mortality: the Busselton Health Study. Sleep. 2008;31(8):1079-85.
9. Reynolds EB, Seda G, Ware JC, Vinik AI, Risk MR, Fishback NF. Autonomic function in sleep apnea patients: increased heart rate variability except during REM sleep in obese patients. Sleep Breath. 2007;11(1):53-60.
10. Gilmartin GS, Lynch M, Tamisier R, Weiss JW. Chronic intermittent hypoxia in humans during 28 nights results in blood pressure elevation and increased muscle sympathetic nerve activity. Am J Physiol Heart Circ Physiol. 2010;299(3):H925-31.
11. Pitson DJ, Stradling JR. Autonomic markers of arousal during sleep in patients undergoing investigation for obstructive sleep apnoea, their relationship to EEG arousals, respiratory events and subjective sleepiness. J Sleep Res. 1998;7(1):53-9.
12. Henderson LA, Woo MA, Macey PM, Macey KE, Frysinger RC, Alger JR, et al. Neural responses during Valsalva maneuvers in obstructive sleep apnea syndrome. J Appl Physiol (1985). 2003;94(3):1063-74.
13. Olmetti F, La Rovere MT, Robbi E, Taurino AE, Fanfulla F. Nocturnal cardiac arrhythmia in patients with obstructive sleep apnea. Sleep Med. 2008;9(5):475-80.
14. Kish L. Survey sampling. New York: John Wiley & Sons Inc; 1965.
15. Korn EL, Graubard BI. Analyses of health surveys. New York: John Wiley & Sons Inc, 1999.
16. Santos-Silva R, Tufik S, Conway SG, Taddei JA, Bittencourt LR. Sao Paulo Epidemiologic Sleep Study: rationale, design, sampling, and procedures. Sleep Med. 2009;10(6):679-85.
17. Rechtschaffen A, Kales A. A manual of standardized terminology: techniques and scoring system for sleep stages of human subjects. Los Angeles: Brain Information Service/ Brain Research Institute; 1968.
18. Iber C, Ancoli-Israel S, Chesson Jr A, Quan S. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. Westchester: American Academy of Sleep Medicine; 2007.
19. Guilleminault C, Connolly SJ, Winkle RA. Cardiac arrhythmia and conduction disturbances during sleep in 400 patients with sleep apnea syndrome. Am J Cardiol. 1983;52(5):490-4.
20. Olmetti F, La Rovere MT, Robbi E, Taurino AE, Fanfulla F. Nocturnal cardiac arrhythmia in patients with obstructive sleep apnea. Sleep Med. 2008;9(5):475-80.
21. Redline S, Young T. Epidemiology and natural history of obstructive sleep apnea. Ear Nose Throat J. 1993;72(1):20-1, 24-6.
22. Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328(17):1230-5.
23. Durán J, Esnaola S, Rubio R, Iztueta A. Obstructive sleep apnea-hypopnea and related clinical features in a population-based sample of subjects aged 30 to 70 yr. Am J Respir Crit Care Med. 2001;163(3 Pt 1):685-9.
24. Ip MS, Lam B, Lauder IJ, Tsang KW, Chung KF, Mok YW, et al. A community study of sleep-disordered breathing in middle-aged Chinese men in Hong Kong. Chest. 2001;119(1):62-9.
25. Somers VK, Mark AL, Zavala DC, Abboud FM. Contrasting effects of hypoxia and hypercapnia on ventilation and sympathetic activity in humans. J Appl Physiol (1985). 1989;67(5):2101-6.
26. Oliveira W, Campos O, Bezerra Lira-Filho E, Cintra FD, Vieira M, Ponchirolli A, et al. Left atrial volume and function in patients with obstructive sleep apnea assessed by real-time three-dimensional echocardiography. J Am Soc Echocardiogr. 2008;21(12):1355-61.
27. Oliveira W, Campos O, Cintra F, Matos L, Vieira ML, Rollim B, et al. Impact of continuous positive airway pressure treatment on left atrial volume and function in patients with obstructive sleep apnoea assessed by real-time three-dimensional echocardiography. Heart. 2009;95(22):1872-8.
28. Harbison J, O’Reilly P, McNicholas WT. Cardiac rhythm disturbances in the obstructive sleep apnea syndrome: effects of nasal continuous positive airway pressure therapy. Chest. 2000;118(3):591-5.
29. Craig S, Pepperell JC, Kohler M, Crosthwaite N, Davies RJ, Stradling JR. Continuous positive airway pressure treatment for obstructive sleep apnoea reduces resting heart rate but does not affect dysrhythmias: a randomized controlled trial. J Sleep Res. 2009;18(3):329-36.
References
373

Original Article
Cintra et al.Sleep and Cardiac Arrhythmia
Arq Bras Cardiol. 2014; 103(5):368-374374

Original Article
Applicability of the Appropriate use Criteria for Myocardial Perfusion ScintigraphyAnderson de Oliveira1,2, Maria Fernanda Rezende1,3, Renato Corrêa3, Rodrigo Mousinho3, Jader Cunha Azevedo1,3, Sandra Marina Miranda1, Aline Ribeiro Oliveira1, Ricardo Fraga Gutterres2, Evandro Tinoco Mesquita1,3, Cláudio Tinoco Mesquita1,3
Universidade Federal Fluminense – UFF1, Niterói, RJ; Comissão Nacional de Energia Nuclear – CNEN2; Hospital Pró-Cardíaco3, Rio de Janeiro, RJ - Brazil
Mailing Address: Anderson Oliveira •Rua das Laranjeiras, 43, Apto. 1406, Laranjeiras - Postal Code: 22240-000, Rio de Janeiro, RJ – BrazilE-mail: [email protected]; [email protected] received December 18, 2013; revised manuscript March 18, 2014; accepted May 26, 2014.
DOI: 10.5935/abc.20140140
Abstract
Background: Appropriateness Criteria for nuclear imaging exams were created by American College of Cardiology (ACC) e American Society of Nuclear Cardiology (ASNC) to allow the rational use of tests. Little is known whether these criteria have been followed in clinical practice.
Objective: To evaluate whether the medical applications of myocardial perfusion scintigraphy (MPS) in a private nuclear medicine service of a tertiary cardiology hospital were suitable to the criteria of indications proposed by the American medical societies in 2005 and 2009 and compare the level of indication of both.
Methods: We included records of 383 patients that underwent MPS, November 2008 up to February 2009. Demographic characteristics, patient’s origin, coronary risk factors, time of medical graduation and appropriateness criteria of medical applications were studied. The criteria were evaluated by two independent physicians and, in doubtful cases, defined by a medical expert in MPS.
Results: Mean age was 65 ± 12 years. Of the 367 records reviewed, 236 (64.3%) studies were performed in men and 75 (20.4%) were internee. To ACC 2005, 255 (69.5%) were considered appropriate indication and 13 (3.5%) inappropriate. With ACC 2009, 249 (67.8%) were considered appropriate indications and 13 (5.2%) inappropriate.
Conclusions: We observed a high rate of adequacy of medical indications for MPS. Compared to the 2005 version, 2009 did not change the results. (Arq Bras Cardiol. 2014; 103(5):375-381)
Keywords: Myocardial/radionuclide imaging; Diagnostic Imaging; Myocardial Perfusion Imaging; Quality of Health Care.
IntroductionThe advances in medical knowledge and technological
development have increased the diagnostic capacity of medical tests. These improvements have led to a marked increase in the use of imaging tests and, consequently, in the associated costs. In the United States, a study with patients treated by Medicare, during 1993–2001, showed a mean annual increase of 6.1% in the number of cardiac stress imaging tests, whereas the increase in cardiac catheterization was 2% and percutaneous coronary interventions was less than 1%, for the total number of individuals with acute myocardial infarction1. Four million myocardial perfusion scintigraphy (MPS) tests were performed in 1998; in 2008 this number was 8 million2. This increase in the volume of diagnostic image procedures, higher than any other medical procedure in the United States, led to the need to create
instruments that suit the clinical practice with respect to the most recent scientific evidence3. For this purpose, the American College of Cardiology Foundation (ACC) and the American Society of Nuclear Cardiology (ASNC) published in 2005 the Appropriateness Criteria for Single-Photon Emission Computed Tomography (SPECT) Myocardial Perfusion Imaging4. In June 2009, a revised and updated version was published among other scientific communities. This revised edition was titled Appropriate Use Criteria for Cardiac Radionuclide Imaging5.
Studies worldwide have tested the application of these appropriateness criteria with the aim of assessing the quality of assistance and guiding strategies for improvement6. Gibbons e cols.1 demonstrated that 14% of scintigraphy procedures and 18% of stress echocardiography tests performed in a university hospital were deemed inappropriate, according to this instrument, and emphasized the need to improve assistance to optimize resources and improve the efficiency of the North-American health system1,7. Until now, no studies, such as the present study, have been conducted in Brazil. The aim of this study was to assess whether the medical use of MPS in a private nuclear medicine department of a tertiary cardiology hospital was appropriate, according to the criteria of indications proposed by the American medical associations in 2005 and 2009, and compare the degree of indication between both publications.
375

Original Article
Oliveira et al.Appropriateness criteria for scintigraphy
Arq Bras Cardiol. 2014; 103(5):375-381
MethodsThis was a retrospective review of 383 medical records
of consecutive patients subjected to resting and stress (physical or pharmacological) MPS scans, according to clinical indication, performed between November 2008 and February 2009. The analyzed variables included the following: demographic characteristics, patients’ origin (outpatient or inpatient), coronary risk factors, physician’s years of training (more than 10 years of training or not), and appropriateness of the use of the test according to the 2005 ACC/ASNC appropriateness criteria. Using the same medical records, we performed a reassessment of the ordered tests, according to the 2009 ACC/ASNC appropriateness criteria, and compared the degree of indication between 2005 and 2009.
Sixteen medical records were excluded from the study because data were incomplete, e.g., the resting or stress test was not performed, the scintigraphy report was absent, or data pertaining to the physician who ordered the test was nonexistent. Myocardial ischemia was deemed present in scintigraphic images when some of the 17 myocardial segments had reversible perfusion defect.
The appropriateness criteria are composed of scenarios or clinical indications that include most cases observed in nuclear medicine cardiac tests. Each of these scenarios is scored on a scale of 1 to 9: I) 7 to 9, classified as appropriate (the test is generally acceptable and consists in a reasonable approach to the scenario); II) 4 to 6, uncertain or possibly appropriate, may be acceptable, i.e., it is a reasonable approach to the indication, and uncertainty also implies the need for further investigation or data on patients to definitely categorize the procedure as appropriate or not and to update the criterion; III) 1 to 3, inappropriate, not a reasonable approach to the indication8. The appropriateness criteria were created by the American College of Cardiology together with several medical associations, according to the modified Delphi method used by the RAND Institute of the University of California in Los Angeles (RAND/UCLA)4, which includes the following four steps: (a) listing of the clinical indications for which the test can be used, (b) review of the clinical indications by a panel of interdisciplinary experts and rating of the indications, (c) meeting of the panel of experts with extensive discussion on the clinical indications and new rating, and (d) tabulation of the indications with their respective scores9.
As recommended by the appropriateness criteria5, patients were classified as symptomatic if the physician indicated the test due to thoracic pain syndrome, anginal equivalent, or electrocardiogram (ECG) findings indicative of ischemia. The following are examples of symptoms related with thoracic pain: feeling of chest tightness, heartburn, pain in the shoulder, palpitations, pain in the jaw, and new anomalies on ECG indicative of ischemic heart disease. Symptoms such as dyspnea or reduced tolerance to exertion, which are coherent with coronary artery disease (CAD), were also considered as anginal equivalent.
With regard to the variables under study, patients were considered hospitalized if they were in the emergency room or in any hospital unit. Age, sex, arterial hypertension, diabetes mellitus, smoking, family history of cardiovascular disease, obesity (body mass index ≥ 30 Kg/m²), menopause, sedentarism, peripheral vascular disease, cerebrovascular disease, renal failure, and thoracic pain syndrome (TPS) were the variables analyzed according to the information contained in the admission records for the test in the nuclear medicine sector. Patients who smoked till the day of the test or up to 5 years before were considered smokers. The reports of the tests considered as normal or not, according to the presence of ischemia, were also analyzed.
The appropriateness of the use of MPS was assessed by two independent physicians and indications were allocated to one of the 67 scenarios provided in the updated document of indications5 and classified as follows: (A) appropriate, (U) uncertain, and (I) inappropriate. If consensus between the two examiners was not reached, the opinion of a third physician, nuclear medicine physician or certified cardiologist with more than 10 years of experience in the field was used. The indications with incomplete information or those that were not included in the scenarios were deemed as nonclassifiable (NC)5.
The present study was approved by the Ethics Committee under number 324 in 11/25/2009.
The results of the variable age are presented as mean ± standard deviation and the remaining results are expressed in percentages. Comparisons were performed using the Mann-Whitney test for age and the chi-squared and Fisher’s exact tests for the remaining variables. Probability values < 0.05 were considered statistically significant. The statistical analyses were performed using the SPSS software, version 22.
ResultsOf the 367 consecutive patients under study, 282 (79.6%)
were outpatients and 75 (20.4%) were inpatients. The mean age was 64.6 ± 12.3 years. Male patients accounted for 64.3% (N = 236) of the tests. The most prevalent risk factor for coronary disease was arterial hypertension [223 (60.8%)], followed by dyslipidemia [184 cases (50.1%)], and thoracic pain [164 cases (44.7%)]. The demographic characteristics are described in Table 1.
Of the 183 referring physicians, 168 (91.8%) had more than 10 years of clinical practice. Eighteen (4.9%) tests were requested by physicians with less than 10 years of clinical practice and 349 (95.1%) tests were indicated by physicians with more than 10 years of clinical practice. As shown in Table 2, according to the 2005 criteria, of the 367 analyzed requests, 255 (69.5%) were classified as appropriate, 49 (13.4%) as uncertain, and 13 (3.5%) as inappropriate, whereas according to the 2009 criteria, 249 (67.8%) were classified as appropriate, 19 (5.2%) as uncertain, and 19 (5.2%) as inappropriate. Moreover, 50 (13.6%) and 80 (21.8%) of the indications according to the 2005 and 2009 ACC, respectively, were categorized as nonclassifiable because it was not possible to allocate them to any of the used criteria.
376

Original Article
Oliveira et al.Appropriateness criteria for scintigraphy
Arq Bras Cardiol. 2014; 103(5):375-381
Table 2 – 2005 and 2009 ACC appropriateness criteria
2005 2009
Criterion N (%) N (%)
Appropriate 255 (69.5) 249 (67.8)
Inappropriate 13 (3.5) 19 (5.2)
Uncertain 49 (13.6) 19 (5.2)
Nonclassifiable 50 (13.4) 80 (21.8)
Using the 2005 ACC, the four main indications classified as appropriate accounted for 56.4% of cases, whereas using the 2009 ACC this percentage was 55.9%. The main appropriate indications are described in Table 3. According to the 2005 ACC, the most frequent indication for MPS [67 cases (18.3%)] was thoracic pain with intermediate pretest probability, interpretable ECG, and ability to perform physical activity. According to the 2009 ACC, the most frequent classifiable indication was nonacute ischemic equivalent with intermediate pretest probability, interpretable ECG, and ability to perform physical activity [49 cases (19.7%)].
Of the indications categorized as inappropriate, the most frequent was in asymptomatic patients up to 1 year after revascularization, with previous symptoms of revascularization [5 patients (38.5%)] for 2005 ACC and
postrevascularization, asymptomatic, and less than 2 years after percutaneous coronary intervention [4 patients (21.1%)] for 2009 ACC. The inappropriate indications and their frequencies are shown in Table 4.
The comparison between appropriate and inappropriate referrals, using the 2005 ACC, showed a significant difference only with regard to obesity (p = 0.022). The same comparison performed according to the 2009 ACC showed a significant difference only for the variable SDT (p = 0.026). Tables 5 and 6 show the comparison between appropriate and inappropriate indications for MPS, according to the 2005 and 2009 ACC appropriateness criteria.
DiscussionThe aim of this study was to assess a new instrument
that promotes the improvement of clinical practices. The appropriateness criteria were developed by the ACC and ASNC with the purpose of assisting physicians and institutions, as well as reducing healthcare costs. In Brazil, until now, there have been no studies on indications for MPS based on these criteria.
In the present study, the clinical indications for MPS showed a high percentage of appropriateness (69.5% and 67.8% according to the 2005 and 2009 ACC, respectively) in a private cardiology hospital. The use of this instrument has expanded exponentially. A study on the appropriateness of transthoracic echocardiography requests according to the ACC appropriateness criteria for echocardiography10 was recently published. It compared the practices between a private cardiology hospital and a public university hospital. The results showed that approximately 25% of the tests were inappropriately requested11. The use of the appropriateness criteria has proved to be very useful for the evaluation of the quality of requests for complementary tests12. More recently, continuing education strategies, such as online dissemination of information regarding appropriate referral, have been proposed to improve clinical practices13. In the present study we assessed the requests for MPS, which is a test of difficult access and that involves radiation exposure.
Similarly to the study by Gibbons et al1, the present study was one of the first evaluations of the use of the appropriateness criteria for test requests in a nuclear medicine department in Latin America, according to the ACC/ASNC appropriateness criteria for SPECT perfusion imaging2. After excluding the cases categorized as nonclassifiable, the ACC/ASNC appropriateness criteria was applied to more than 87% and 78% of the clinical indications for MPS for the 2005 and 2009 ACC, respectively, in the department where the study was conducted. The inappropriate indications corresponded to 3.5% and 5.2% and the uncertain indications to 13.4% and 5.2%, for 2005 and 2009 ACC, respectively. These results highlight the need to improve the efficiency of our health system. In the outpatient context, the percentage of appropriate indications was lower (64.4% for 2005 and 2009 ACC) than that observed in the inpatient context (89.3% for 2005 and 81.3% for 2009 ACC). This analysis was not performed in the study by Gibbons et al1 because the sample only included hospitalized patients. Better interaction between the referring physician and the team responsible for
Table 1 – Demographic characteristics of the sample (N = 367)
Variables N (%)
Age (mean ± sd) 65 ± 12
Sex
Male 236 (64.3)
Origin
Inpatient 75 (20.4)
Outpatient 282 (79.6)
Complaint of thoracic pain 164 (44.7)
Comorbidities
Arterial hypertension 223 (60.8)
Dyslipidemia 184 (50.1)
Diabetes 98 (26.7)
Family history of cardiovascular disease 129 (35.1)
Smoking 63 (17.2)
Sedentarism 123 (33.5)
Menopause 84 (22.9)
Obesity (BMI ≥ 30 Kg/m²) 74 (20.2)
Peripheral vascular disease 12 (3.3)
Cerebrovascular disease 7 (1.9)
Renal failure 3 (0.8)
SD: standard deviation; BMI: body mass index.
377

Original Article
Oliveira et al.Appropriateness criteria for scintigraphy
Arq Bras Cardiol. 2014; 103(5):375-381
Table 3 – Most common appropriate indications for myocardial scintigraphy according to the 2005 and 2009 ACC appropriateness criteria
2005 2009
Indications N (%) Indications N (%)
Thoracic pain with intermediate pretest probability, interpretable ECG, and able to perform physical activity 67 (18.3) Nonclassifiable 86 (34.5)
Intermediate Duke e Framinghan scores 51 (13.9) Nonacute ischemic equivalent with intermediate pretest probability, interpretable ECG, and able to perform physical activity 49 (19.7)
With pain, after intervention or angioplasty 50 (13.6) Intermediate Duke score 34 (13.7)
Thoracic pain with intermediate pretest probability, noninterpretable ECG, and unable to perform physical activity 39 (10.6) Symptomatic postrevascularization 33 (13.3)
Thoracic pain with high pretest probability, interpretable ECG, and able to perform physical activity 16 (4.4) Nonacute ischemic equivalent with intermediate pretest probability,
noninterpretable ECG, or unable to perform physical activity 23 (9.2)
ECG: Electrocardiogram.
Table 4 – Inappropriate indications for myocardial scintigraphy, according to the ACC appropriateness criteria
2005 2009
Indications N (%) Indications N (%)
Asymptomatic until 1 year after revascularization, with previous symptoms 5 (38.5) Nonclassifiable 6 (31.6)
Thoracic pain with low pretest probability, interpretable ECG, and able to perform physical activity 4 (30.8) Postrevascularization, asymptomatic, and less than 2 years
after percutaneous coronary intervention 4 (21.1)
Low risk preoperative 2 (15.4) Pain or ischemic equivalent, low pretest probability, interpretable ECG, and able to perform physical activity 3 (15.8)
Asymptomatic or with previous study and high-risk Framinghan and annual scintigraphy study 1 (7.7) Low risk preoperative 2 (10.5)
Low intermediate preoperative, with tolerance to exertion ≥ 4 MET 1 (7.7) Other* 1 (5,3)
MET: metabolic equivalent; (*) Four indications had the same frequency.
Table 5 – Comparison between appropriate and inappropriate indications for myocardial scintigraphy, according to the 2005 ACC appropriateness criteria
Variables Appropriate N (%) Inappropriate N (%) p value
Sex
Female 100 (97.1) 3 (2.9)0.243
Male 155 (93.9) 10 (6.1)
Origin
Inpatient 67 (95.7) 3 (4.3)0.798
Outpatient 188 (94.9) 10 (5.1)
Dyslipidemia
No 123 (93.9) 8 (6.1)0.349
Yes 132 (96.4) 5 (3.6)
Obesity
No 205 (96.7) 7 (3.3)0.022
Yes 50 (89.3) 6 (10.7)
378

Original Article
Oliveira et al.Appropriateness criteria for scintigraphy
Arq Bras Cardiol. 2014; 103(5):375-381
Table 6 – Comparison between appropriate and inappropriate indications for myocardial scintigraphy, according to the 2009 ACC appropriateness criteria
Variables Appropriate N (%) Inappropriate N (%) p value
Sex
Female 93 (94.9) 5 (5.1)0.336
Male 156 (91.8) 14 (8.2)
Origin
Inpatient 61 (95.3) 3 (4.7)0.391
Outpatient 188 (92.2) 16 (7.8)
Dyslipidemia
No 114 (91.2) 11 (8,8)0.308
Yes 135 (94.4) 8 (5,6)
Thoracic pain syndrome
No 105 (89) 13 (11)0.026
Yes 144 (96) 6 (4)
performing the tests and the fact that hospitalized patients often have more serious diseases, for which the use of scintigraphy is more well established, probably contributed to higher rate of appropriate requests in the group of inpatients.
Another aspect observed in our study, which was emphasized by Hendel et al5, was the application of the appropriateness criteria to allow an institution, a group of physicians, and even a health manager to assess standards and practices and identify areas susceptible to improvement. In addition, the criteria are a useful instrument for training, awareness and development of standards of practice regarding the appropriate request of tests. The following are among the most frequent inappropriate indications for myocardial scintigraphy observed in the clinical practice: (1) scintigraphy in asymptomatic patients and (2) scintigraphy in asymptomatic patients with less than 2 years of revascularization and complaints of symptoms before angioplasty14. The findings that routine evaluation of patients in the first year after coronary angioplasty corresponded to 38.5 % of inappropriate indications for myocardial scintigraphy according to the 2005 ACC, and that 21.1% of inappropriate requests according to the 2009 ACC corresponded to the routine evaluation of patients in the first 2 years after coronary angioplasty suggest that these indications should be the focus of educational programs and other interventions aimed at the referring physicians. Gibbons et al15 implemented a program of quality improvement focusing on inappropriate requests for scintigraphy and, although they did not observe a significant improvement in the rate of appropriate referrals, they suggested that specific efforts should be made, based on the data obtained from appropriateness assessment. Saifi et al13 demonstrated that the online use of a continuing education instrument can promote the increase in the number of appropriate myocardial scintigraphy tests.
The appropriateness criteria are an instrument in progress and, with the publication of the new version, some authors observed a change in the rate of nonclassifiable tests and an increase in the rate of uncertain and inappropriate tests14,16,17. In the sample analyzed in this study, the rate of appropriate tests remained unchanged, the rate of uncertain tests decreased, and the rate of nonclassifiable tests increased. These differences may be associated with local experience and the most common type of indication in a given region. Moreover, of the 182 clinicians that requested tests, 95% had more than 10 years of clinical practice. This finding indicates that the analyzed population consists of experienced physicians, which is not necessarily representative of the situation in most institutions.
The update of criteria and the conduction of more studies in other regions of Brazil are necessary for the inclusion of more indications. Although the criteria of 2009 were not available to cardiologists when the tests included in this study were requested, we believe the analyses are valid because there was no significant change in clinical practices between the 2005 and 2009 publications of the appropriateness criteria; these publications were an attempt to improve the instrument5. Despite the limitations of a retrospective study, the present analysis is valid because it gives an overview of this practice.
The rational use of complementary tests in cardiology is one of the major challenges experienced by clinical practitioners today18-20. Although technology has allowed these methods to aggregate an increasing amount of valuable information, its indiscriminate use may not contribute in changing the outlined strategy, and may even add costs and risks inherent to the techniques, such as exposure to contrast media or radiation21,22. The search for quality directly involves the refinement of clinical referrals as a way of selecting patients who are most likely to benefit from these tests23,24. This study,
379

Original Article
Oliveira et al.Appropriateness criteria for scintigraphy
Arq Bras Cardiol. 2014; 103(5):375-381
which is the first in the Brazilian literature to focus on the use of the appropriateness criteria for myocardial scintigraphy, showed that this instrument is indeed useful for this purpose and that new studies should be conducted in different contexts so as to contribute to better clinical practices.
ConclusionsIn this study there was a high appropriateness of clinical
indications for MPS in a cardiology hospital, according to the appropriateness criteria, in particular among hospitalized patients. Moreover, there was no significant difference between the percentages of appropriate and inappropriate tests when using the 2005 and 2009 criteria. Further prospective studies and studies involving more physicians with less than 10 years of clinical practice should be developed to confirm the results presented in this article.
Author contributionsConception and design of the research, Analysis and
interpretation of the data and Writing of the manuscript:
Oliveira A, Rezende MF, Corrêa R, Mousinho R, Azevedo JC, Miranda SM, Oliveira AR, Gutterres RF, Mesquita ET, Mesquita CT; Acquisition of data: Oliveira A, Rezende MF, Corrêa R, Mousinho R, Mesquita CT; Statistical analysis: Oliveira A, Mesquita CT; Critical revision of the manuscript for intellectual content: Oliveira A, Rezende MF, Azevedo JC, Miranda SM, Oliveira AR, Gutterres RF, Mesquita ET, Mesquita CT.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
This study was funded by FAPERJ.
Study Association
This article is part of the thesis of Doctoral submitted by Anderson de Oliveira, from Universidade Federal Fluminense.
1. Gibbons RJ, Miller TD, Hodge D, Urban L, Araoz PA, Pellikka P, et al. Application of appropriateness criteria to stress single-photon emission computed tomography sestamibi studies and stress echocardiograms in an academic medical center. J Am Coll Cardiol. 2008;51(13):1283-9.
2. Bonow RO. Is appropriateness appropriate? J Am Coll Cardiol. 2008;51(13):1290-1.
3. Lin FY, Rosenbaum LR, Gebow D, Kim RJ, Wolk MJ, Patel MR, et al. Cardiologist concordance with the American College of Cardiology appropriate use criteria for cardiac testing in patients with coronary artery disease. Am J Cardiol. 2012;110(3):337-44.
4. Brindis RG, Douglas PS, Hendel RC, Peterson ED, Wolk MJ, Allen JM, et al; American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group; American Society of Nuclear Cardiology; American Heart Association. ACCF/ASNC appropriateness criteria for single-photon emission computed tomography myocardial perfusion imaging (SPECT MPI): a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group and the American Society of Nuclear Cardiology endorsed by the American Heart Association. J Am Coll Cardiol. 2005;46(8):1587-605. Erratum in: J Am Coll Cardiol. 2005;46(11):2148-50.
5. Hendel RC, Berman DS, Di Carli MF, Heidenreich PA, Henkin RE, Pellikka PA, et al; American College of Cardiology Foundation Appropriate Use Criteria Task Force; American Society of Nuclear Cardiology; American College of Radiology; American Heart Association; American Society of Echocardiography; Society of Cardiovascular Computed Tomography; Society for Cardiovascular Magnetic Resonance; Society of Nuclear Medicine. ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 appropriate use criteria for cardiac radionuclide imaging: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the American Society of Nuclear Cardiology, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the Society of Cardiovascular Computed Tomography, the Society for Cardiovascular Magnetic Resonance, and the Society of Nuclear Medicine. Circulation. 2009;119(22):e561-87.
6. Koh AS, Flores JL, Keng FY, Tan RS, Chua TS. Evaluation of the American College of Cardiology Foundation/American Society of Nuclear Cardiology appropriateness criteria for SPECT myocardial perfusion imaging in an Asian tertiary cardiac center. J Nucl Cardiol. 2011;18(2):324-30.
7. Chew M, Koh AS, Salunat-Flores JL, Keng FY, Chua TS. Evaluation of the Appropriateness Criteria of SPECT Myocardial Perfusion Imaging in a Large Asian Academic Hospital: A Pilot Prospective Study. Heart, lung & circulation. 2009;18:S34-S5.
8. Badheka AO, Hendel RC. Radionuclide cardiac stress testing. Curr Opin Cardiol. 2011;26(5):370-8.
9. Patel MR, Spertus JA, Brindis RG, Hendel RC, Douglas PS, Peterson ED, et al; American College of Cardiology Foundation. ACCF proposed method for evaluating the appropriateness of cardiovascular imaging. J Am Coll Cardiol. 2005;46(8):1606-13.
10. Douglas PS, Khandheria B, Stainback RF, Weissman NJ, Brindis RG, Patel MR, et al; American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group; American Society of Echocardiography; American College of Emergency Physicians; American Society of Nuclear Cardiology; Society for Cardiovascular Angiography and Interventions; Society of Cardiovascular Computed Tomography; Society for Cardiovascular Magnetic Resonance; American College of Chest Physicians; Society of Critical Care Medicine. ACCF/ASE/ACEP/ASNC/SCAI/SCCT/SCMR 2007 appropriateness criteria for transthoracic and transesophageal echocardiography: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American Society of Echocardiography, American College of Emergency Physicians, American Society of Nuclear Cardiology, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and the Society for Cardiovascular Magnetic Resonance endorsed by the American College of Chest Physicians and the Society of Critical Care Medicine. J Am Coll Cardiol. 2007;50(2):187-204.
11. Barbosa FC, Mesquita ET, Barachi LB, Salgado A, Kazuo R, Rosa ML, et al. Comparaçao da adequaçao de solicitaçao de ecocardiograma entre hospitais público e privado. Arq Bras Cardiol. 2011;97(4):281-8.
References
380

Original Article
Oliveira et al.Appropriateness criteria for scintigraphy
Arq Bras Cardiol. 2014; 103(5):375-381
12. Aldweib N, Negishi K, Seicean S, Jaber WA, Hachamovitch R, Cerqueira M, et al. Appropriate test selection for single-photon emission computed tomography imaging: association with clinical risk, posttest management, and outcomes. Am Heart J. 2013;166(3):581-8.
13. Saifi S, Taylor AJ, Allen J, Hendel R. The use of a learning community and online evaluation of utilization for SPECT myocardial perfusion imaging. JACC Cardiovasc Imaging. 2013;6(7):823-9.
14. Farrell MB, Cerqueira MD. Understanding appropriate use criteria in nuclear medicine. J Nucl Med Technol. 2012;40(2):81-6.
15. Gibbons RJ, Askew JW, Hodge D, Kaping B, Carryer DJ, Miller T. Appropriate use criteria for stress single-photon emission computed tomography sestamibi studies: a quality improvement project. Circulation. 2011;123(5):499-503.
16. Carryer DJ, Hodge DO, Miller TD, Askew JW, Gibbons RJ. Application of appropriateness criteria to stress single photon emission computed tomography sestamibi studies: a comparison of the 2009 revised appropriateness criteria to the 2005 original criteria. Am Heart J. 2010;160(2):244-9.
17. Gholamrezanezhad A, Shirafkan A, Mirpour S, Rayatnavaz M, Alborzi A, Mogharrabi M, et al. Appropriateness of referrals for single-photon emission computed tomography myocardial perfusion imaging (SPECT-MPI) in a developing community: a comparison between 2005 and 2009 versions of ACCF/ASNC appropriateness criteria. J Nucl Cardiol. 2011;18(6):1044-52.
18. McCully RB, Pellikka PA, Hodge DO, Araoz PA, Miller TD, Gibbons RJ. Applicability of appropriateness criteria for stress imaging: similarities and differences between stress echocardiography and single-photon emission computed tomography myocardial perfusion imaging criteria. Circ Cardiovasc Imaging. 2009;2(3):213-8.
19. Lin FY, Dunning AM, Narula J, Shaw LJ, Gransar H, Berman DS, et al. Impact of an automated multimodality point-of-order decision support tool on rates of appropriate testing and clinical decision making for individuals with suspected coronary artery disease: a prospective multicenter study. J Am Coll Cardiol. 2013;62(4):308-16.
20. White RD, Patel MR, Abbara S, Bluemke DA, Herfkens RJ, Picard M, et al; American College of Radiology; American College of Cardiology Foundation. 2013 ACCF/ACR/ASE/ASNC/SCCT/SCMR appropriate utilization of cardiovascular imaging in heart failure: an executive summary: a joint report of the ACR Appropriateness Criteria (R) Committee and the ACCF Appropriate Use Criteria Task Force. J Am Coll Radiol. 2013;10(7):493-500.
21. Koukouraki S, Pagonidis K, Perisinakis K, Klinaki I, Stathaki M, Damilakis J, et al. Hybrid cardiac imaging: insights in the dilemma of the appropriate clinical management of patients with suspected coronary artery disease. Eur J Radiol. 2013;82(2):281-7.
22. Nelson KH, Willens HJ, Hendel RC. Utilization of radionuclide myocardial perfusion imaging in two health care systems: assessment with the 2009 ACCF/ASNC/AHA appropriateness use criteria. J Nucl Cardiol. 2012;19(1):37-42.
23. Druz RS, Phillips LM, Sharifova G. Clinical evaluation of the appropriateness use criteria for single-photon emission-computed tomography: differences by patient population, physician specialty, and patient outcomes. ISRN Cardiol. 2011;2011:798318.
24. Hoffmann U, Venkatesh V, White RD, Woodard PK, Carr JJ, Dorbala S, et al. ACR Appropriateness Criteria((R)) acute nonspecific chest pain-low probability of coronary artery disease. J Am Coll Radiol. 2012;9(10):745-50.
381

Original Article
Congenital Heart Disease as a Warning Sign for the Diagnosis of the 22q11.2 DeletionMarcília S. Grassi1, Cristina M. A. Jacob1, Leslie D. Kulikowski3, Antonio C. Pastorino1, Roberta L. Dutra3, Nana Miura2, Marcelo B. Jatene2, Stephanie P. Pegler1, Chong A. Kim1, Magda Carneiro-Sampaio1
Instituto da Criança – HC-FMUSP1; Instituto do Coração – HC-FMUSP2; Departamento de Patologia da Faculdade de Medicina da Universidade de São Paulo3, São Paulo, SP - Brazil
Mailing Address: Marcília Sierro Grassi •Avenida Dr. Enéas de Carvalho Aguiar, 647, Postal Code 05403.000, Sao Paulo, SP – BrazilE-mail: [email protected] received January 06, 2014; revised manuscript July 07, 2014; accepted July 23, 2014.
DOI: 10.5935/abc.20140145
Abstract
Background: To alert for the diagnosis of the 22q11.2 deletion syndrome (22q11.2DS) in patients with congenital heart disease (CHD).
Objective: To describe the main CHDs, as well as phenotypic, metabolic and immunological findings in a series of 60 patients diagnosed with 22q11.2DS.
Methods: The study included 60 patients with 22q11.2DS evaluated between 2007 and 2013 (M:F = 1.3, age range 14 days to 20 years and 3 months) at a pediatric reference center for primary immunodeficiencies. The diagnosis was established by detection of the 22q11.2 microdeletion using FISH (n = 18) and/or MLPA (n = 42), in association with clinical and laboratory information. Associated CHDs, progression of phenotypic facial features, hypocalcemia and immunological changes were analyzed.
Results: CHDs were detected in 77% of the patients and the most frequent type was tetralogy of Fallot (38.3%). Surgical correction of CHD was performed in 34 patients. Craniofacial dysmorphisms were detected in 41 patients: elongated face (60%) and/or elongated nose (53.3%), narrow palpebral fissure (50%), dysplastic, overfolded ears (48.3%), thin lips (41.6%), elongated fingers (38.3%) and short stature (36.6%). Hypocalcemia was detected in 64.2% and decreased parathyroid hormone (PTH) level in 25.9%. Decrease in total lymphocytes, CD4 and CD8 counts were present in 40%, 53.3% and 33.3%, respectively. Hypogammaglobulinemia was detected in one patient and decreased concentrations of immunoglobulin M (IgM) in two other patients.
Conclusion: Suspicion for 22q11.2DS should be raised in all patients with CHD associated with hypocalcemia and/or facial dysmorphisms, considering that many of these changes may evolve with age. The 22q11.2 microdeletion should be confirmed by molecular testing in all patients. (Arq Bras Cardiol. 2014; 103(5):382-390)
Keywords: DiGeorge Syndrome; Crromosome Delection; Heart Defects, Congenital; Hypocalcemia; Chromosomes, Human.
IntroductionThe 22q11.2 deletion syndrome (22q11.2DS) is considered
the most frequent chromosomal microdeletion syndrome in humans, with an incidence of 1:4,000-5,000 live births1,2. This syndrome is currently recognized as occurring with a higher frequency than previously estimated, although precise information about its incidence in our country are unknown.
Microdeletions in the 22q11.2 region can occur in various syndromes such as the DiGeorge (DGS), velocardiofacial and the conotruncal anomaly face syndromes. These diseases represent different phenotypes of the same chromosomal abnormality, which are currently
grouped and titled 22q11.2DS1,3. This microdeletion is not detected on G-banding karyotyping, a routine cytogenetic exam. The molecular diagnosis of the syndrome is rather established by other techniques such as fluorescence in situ hybridization (FISH) and/or quantitative genomic analysis by multiplex ligation-dependent probe amplification (MLPA)4,5.
Congenital heart diseases (CHDs) are one of the most frequent malformations, with an incidence that ranges from 8 to 10 per 1,000 live births, representing an important cause of morbimortality in the first year of life6. The etiology of cardiopathies associated with other types of congenital malformations can be monogenic, as in Holt-Oram, Marfan, Fanconi and Noonan syndromes, or chromosomal, as in Down, 22q1.2DS, 18 trisomy (Edwards) and 13 trisomy (Patau) syndromes7. CHDs with conotruncal defects represent an important characteristic in several genetic syndromes, in particular in 22q11.2DS2. It is estimated that 5% of the patients with cardiopathy have DGS, which is considered the second most common primary immunodeficiency8-11.
Clinical manifestations that should arise suspicion for 22q11.2SD are CHD (75%), abnormal psychomotor development (68%), hypocalcemia-associated seizure
382

Original Article
Grassi et al.Cardiopathies and 22q11.2 deletion syndrome
Arq Bras Cardiol. 2014; 103(5):382-390
(60%), velopharyngeal insufficiency with nasal voice (46%), genitourinary abnormalities (36%), skeletal abnormalities (17%) and facial dysmorphisms (11-17%)2,12-15. The immunological changes associated with 22q11.2DS are variable and secondary to thymic hypoplasia or agenesis, classically named DGS by immunologists1,5,14-17.
The aim of this study is to describe the main cardiopathies, as well as phenotypic, metabolic and immunologic abnormalities in a series of 60 patients with 22q11.2DS.
MethodsThis is a descriptive, transversal, retrospective and
prospective study evaluating all patients with 22q11.2DS followed at the Allergy and Immunology Unit and Genetic Unit at Instituto da Criança of HC-FMUSP between June 2007 until December 2013. Some of the patients were referred from the Pediatric Cardiology Unit of Instituto do Coração (INCOR) – HC-FMUSP after active search at this institution. The sample was composed of 60 children and adolescentes (34 males), with age range from 14 days to 20 years and 3 months (mean 114.2 months, standard deviation 83 months). All the individuals belonged to Brazilian families, and there was no predominance in the cohort of European, African or Oriental descent. The diagnostic criteria adopted were those proposed by the International Union of Immunological Societies-IUIS18, which included compatible clinical signs and presence of the 22q11.2 microdeletion. All patients had normal karyotype by G-banding. Information about patient’s identification, clinical history, physical examinatin and results from laboratory and cytogenomic analyses were collected in a protocol form.
The molecular analysis of the microdeletion was conducted at the Cytogenomics Laboratory of the Department of Pathology, with fluorescent in situ hybridization (FISH) using a specific probe for the 22q11.2 region. Commercial probes of unique sequences were used for the specific region in 22q11.2 (probes DGS/VCFS, TUPLE1 and N25 D22S75, Cytocell, Cambridge, UK)4,19 and/or MLPA using various kits (P036-E1, P070-B2, P064-B3, MRC-Holland, Amsterdam, Netherlands – www.mlpa.com). Generated data were analyzed with the software GeneMarker® (Softgenetics, LLC, State College, PA, USA – www.softgenetics.com). These techniques are demonstrated in Figure 1.
All patients underwent clinical and imaging evaluations at the Pediatric Cardiology Unit.
Immunocompetence was evaluated with complete blood count, measurement of serum immunoglobulin levels (IgG, IgM and IgA) by nephelometry, and determination of lymphocyte subpopulations in peripheral blood (flow cytometry - BD FACSCalibur) at the laboratory of the Central Institute of HC-FMUSP, using as comparison reference values already described20,21.
Other performed tests included serum measurement of parathyroid hormone level (PTH, automated chemiluminescent enzyme immunoassay), ionic calcium, total calcium and phosphorus (automated colorimetric method), triiodothyronine (T3), thyroxine (T4), free thyroxine (free T4)
and TSH (automated immunoassay), as well as determination of antithyroglobulin and antithyroperoxidase antibodies (indirect immunofluorescence).
Statistical tests were performed with the software MedCalc 10.2 (MedCalc Software, 2009).
The study was approved by the Ethics Committee for Analysis of Research Project of Hospital das Clínicas – CAPPesq, registration number 0911/11.
ResultsThe presence of CHDs was identified in 47 patients (77%)
and surgical correction was performed in 34 of these, the most frequent of which were tetralogy of Fallot, ventricular septal defect and pulmonary artery atresy, as described in Table 1 and Graph 1.
Other important phenotypic features found in patients from the overall cohort with 22q11.2DS are shown in Table 2. Facial features, as well as morphology of the ears, mouth, nose and eyes of some patients are shown in Figures 2 and 3.
The presence of facial dysmorphisms was not recognized during the neonatal period in many patients, becoming more evident with increasing age, as observed in Figure 4.
Hypocalcemia was diagnosed in 27 of the 42 patients (64.2%) in whom ionic calcium was measured, 16 (59.3%) of which occurred in the neonatal period. Of these, PTH was measured in 27 patients and was found to be reduced in 7 patients (25.9%). Seizures occurred in 6 patients.
During follow-up of 20 patients with 22q11.2DS through school years and adolescence, we observed that 11 progressed with behavioral and psychiatric abnormalities. The most common finding was attention deficit hyperactivity disorder (ADHD) in 6 patients, 4 of which had the hyperactive/impulsive type and 2 had the predominantly innatentive type. Other findings included learning disability (15%), anxiety (10%) and mental retardation (5%). Until present, none of the patients has progressed with compulsive-obsessive, schizoaffective or psychotic disorders.
In this study, low total lymphocyte count was found in 40% of the patients (18/45 cases), whereas low CD4+ lymphocytes occurred in 53.3% (16/30) and low CD8+ in 33.3% (10/30), as demonstrated in Graph 2. The evaluation of humoral immunity detected 2 patients with reduced IgM concentrations (29.6 mg/dL and 17.6 mg/dL) and one 9-month-old patient with IgG of 328 mg/dL, currently receiving replacement therapy with intravenous gamma globulin.
DiscussionEven though 22q11.2SD is considered in the literature to be
a relatively frequent chromosomal abnormality, pediatricians, neonatologists and cardiologists in our country have not been recognizing it sistematically, and the publications with significant number of patients, particularly in the first year of life, are scarce1,2. In a study conducted at Hospital das Clínicas of HC-FMUSP with 1,008 patients with primary immunodeficiency, only 32 patients with 22q11.2DS were
383
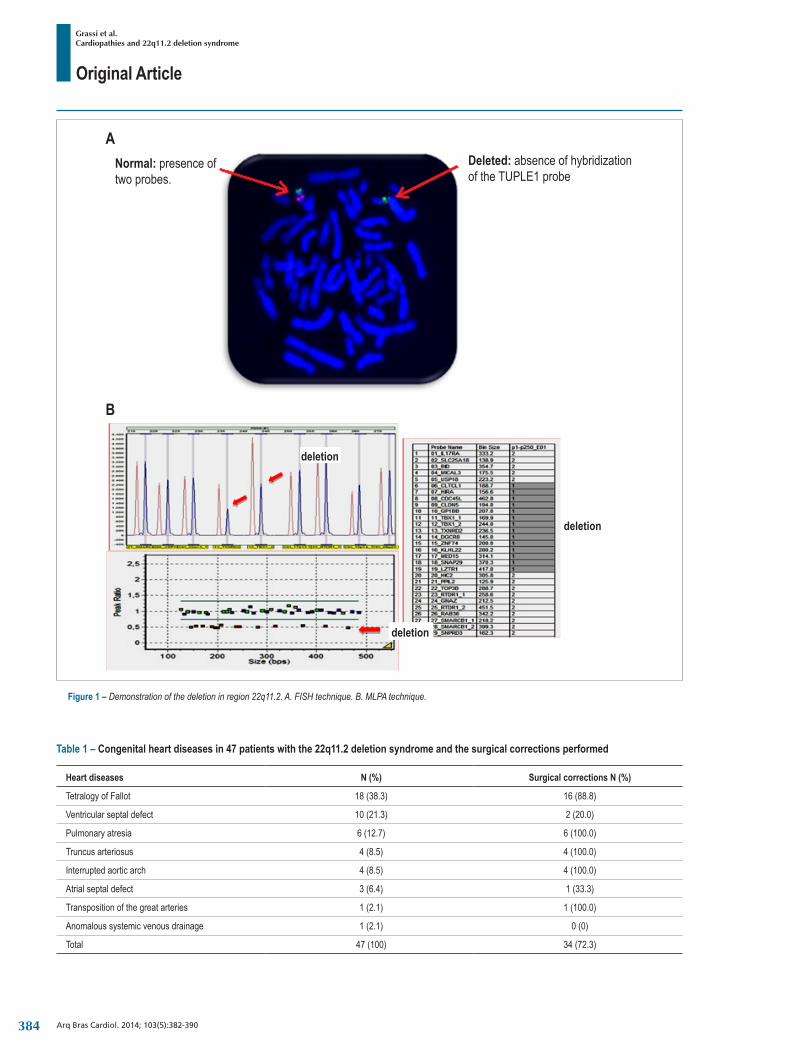
Original Article
Grassi et al.Cardiopathies and 22q11.2 deletion syndrome
Arq Bras Cardiol. 2014; 103(5):382-390
Table 1 – Congenital heart diseases in 47 patients with the 22q11.2 deletion syndrome and the surgical corrections performed
Heart diseases N (%) Surgical corrections N (%)
Tetralogy of Fallot 18 (38.3) 16 (88.8)
Ventricular septal defect 10 (21.3) 2 (20.0)
Pulmonary atresia 6 (12.7) 6 (100.0)
Truncus arteriosus 4 (8.5) 4 (100.0)
Interrupted aortic arch 4 (8.5) 4 (100.0)
Atrial septal defect 3 (6.4) 1 (33.3)
Transposition of the great arteries 1 (2.1) 1 (100.0)
Anomalous systemic venous drainage 1 (2.1) 0 (0)
Total 47 (100) 34 (72.3)
Figure 1 – Demonstration of the deletion in region 22q11.2. A. FISH technique. B. MLPA technique.
B
ANormal: presence oftwo probes.
Deleted: absence of hybridizationof the TUPLE1 probe
deletion
deletion
deletion
384
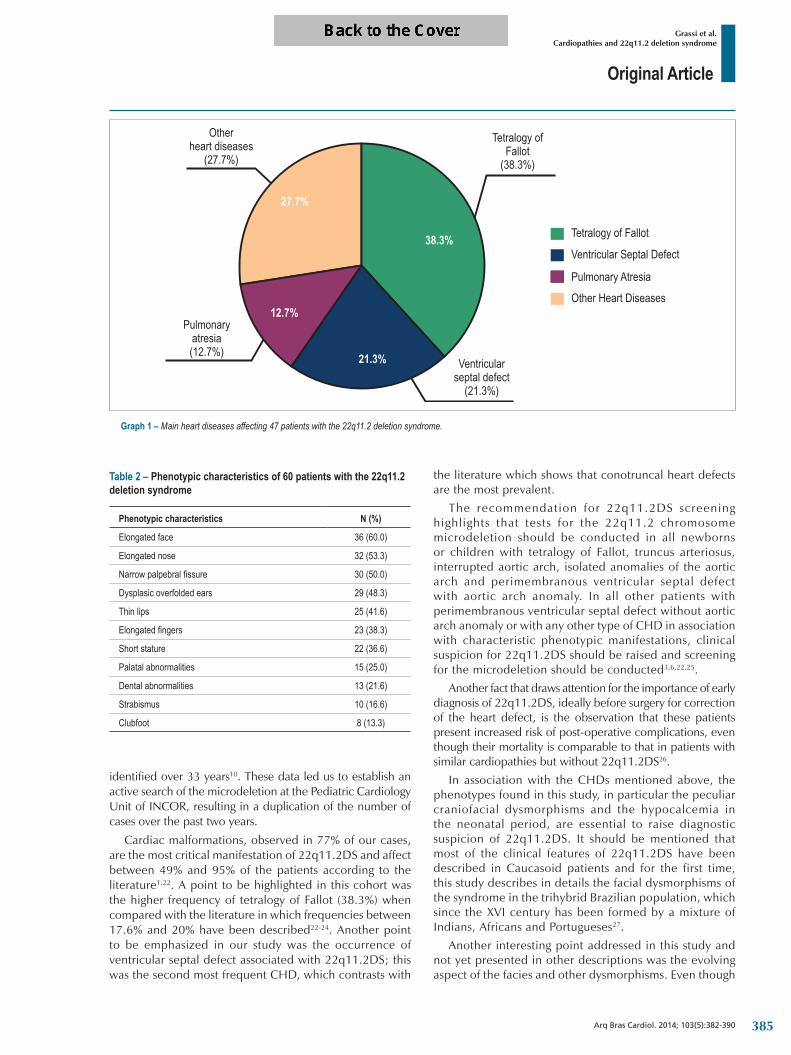
Original Article
Grassi et al.Cardiopathies and 22q11.2 deletion syndrome
Arq Bras Cardiol. 2014; 103(5):382-390
Graph 1 – Main heart diseases affecting 47 patients with the 22q11.2 deletion syndrome.
Otherheart diseases
(27.7%)
Tetralogy ofFallot
(38.3%)
Ventricularseptal defect
(21.3%)
Pulmonaryatresia(12.7%)
Tetralogy of Fallot
Ventricular Septal Defect
Pulmonary AtresiaOther Heart Diseases
38.3%
12.7%
21.3%
27.7%
identified over 33 years10. These data led us to establish an active search of the microdeletion at the Pediatric Cardiology Unit of INCOR, resulting in a duplication of the number of cases over the past two years.
Cardiac malformations, observed in 77% of our cases, are the most critical manifestation of 22q11.2DS and affect between 49% and 95% of the patients according to the literature1,22. A point to be highlighted in this cohort was the higher frequency of tetralogy of Fallot (38.3%) when compared with the literature in which frequencies between 17.6% and 20% have been described22-24. Another point to be emphasized in our study was the occurrence of ventricular septal defect associated with 22q11.2DS; this was the second most frequent CHD, which contrasts with
Table 2 – Phenotypic characteristics of 60 patients with the 22q11.2 deletion syndrome
Phenotypic characteristics N (%)
Elongated face 36 (60.0)
Elongated nose 32 (53.3)
Narrow palpebral fissure 30 (50.0)
Dysplasic overfolded ears 29 (48.3)
Thin lips 25 (41.6)
Elongated fingers 23 (38.3)
Short stature 22 (36.6)
Palatal abnormalities 15 (25.0)
Dental abnormalities 13 (21.6)
Strabismus 10 (16.6)
Clubfoot 8 (13.3)
the literature which shows that conotruncal heart defects are the most prevalent.
The recommendation for 22q11.2DS screening highlights that tests for the 22q11.2 chromosome microdeletion should be conducted in all newborns or children with tetralogy of Fallot, truncus arteriosus, interrupted aortic arch, isolated anomalies of the aortic arch and perimembranous ventricular septal defect with aortic arch anomaly. In all other patients with perimembranous ventricular septal defect without aortic arch anomaly or with any other type of CHD in association with characteristic phenotypic manifestations, clinical suspicion for 22q11.2DS should be raised and screening for the microdeletion should be conducted3,6,22,25.
Another fact that draws attention for the importance of early diagnosis of 22q11.2DS, ideally before surgery for correction of the heart defect, is the observation that these patients present increased risk of post-operative complications, even though their mortality is comparable to that in patients with similar cardiopathies but without 22q11.2DS26.
In association with the CHDs mentioned above, the phenotypes found in this study, in particular the peculiar craniofacial dysmorphisms and the hypocalcemia in the neonatal period, are essential to raise diagnostic suspicion of 22q11.2DS. It should be mentioned that most of the clinical features of 22q11.2DS have been described in Caucasoid patients and for the first time, this study describes in details the facial dysmorphisms of the syndrome in the trihybrid Brazilian population, which since the XVI century has been formed by a mixture of Indians, Africans and Portugueses27.
Another interesting point addressed in this study and not yet presented in other descriptions was the evolving aspect of the facies and other dysmorphisms. Even though
385

Original Article
Grassi et al.Cardiopathies and 22q11.2 deletion syndrome
Arq Bras Cardiol. 2014; 103(5):382-390
the dysmorphisms of 22q11.2DS recognized later in life (narrow palpebral fissures, elongated nose, overfolded ears) are already present at birth, the facies of the newborn and young infant draws less attention as a “syndromic facies” for the general pediatrician and/or cardiologist in this phase of life.
Palatal abnormalities occur in 9–16% of the patients with 22q11.2DS and are associated with a high morbidity. It is, therefore, fundamental to examine the palate carefully and include a search for bifid uvula which may suggest the presence of submucosal cleft palate2,14. In this series, we observed that this finding was more frequent than that described in the literature. Goldmuntz et al in 2005 demonstrated that in addition to cleft palate, about 80% of the patients also present velopharyngeal insufficiency manifesting as nasal voice and compensatory articulation disorders3. Nasal voice is an underappreciated sign for suspicion of 22q11.2DS, probably because it is observed later in life, but it should be considered a warning sign for the occurrence of the syndrome.
Parathyroid hypoplasia or aplasia is very common in 22q11.2DS due to involvement of the third and fourth pharyngeal arches during embryogenesis. In 49% to 60% of the newborns affected by the syndrome, transient hypocalcemia may be present leading to tetany and seizures of difficult control22, data that was similar in the patients in this study. Pediatricians and cardiologists should be attentive
during the neonatal period to the presence of hypocalcemia without other apparent physiopathological cause, a manifestation that is highly suggestive of the syndrome.
Another variable manifestation in 22q11.2DS is immunodeficiency, considered to be due to abnormal development of the thymus, denominated DGS in these cases. Around 80% of the patients with DGS have immune system abnormalities. Even though the thymus is hypoplasic or absent in great part of the patients, most present mild to moderate immunodeficiency, independent of other clinical features28,29. A study conducted by Patel et al29 showed that a minority of the patients have low immunoglobulin levels and, in general, between 2% and 3% need immunoglobulin replacement therapy29. In our study, 3 patients had low levels of immunoglobulins and only 1 patient required immunoglobulin replacement therapy.
Since in patients with 22q11.2DS the initial manifestation may be hyperactivity, anxiety and depression, the authors emphasize the importance of an early diagnosis and a multiprofessional follow-up appropriate for these patients. The diagnosis of ADHD, anxiety disorders, mood disorders and disorders of the autism spectrum can occur in one third to half of the children with the deletion. Mood abnormalities and psychotic disorders can increase significantly during early adulthood, it is therefore fundamental to monitor carefully the occurrence of psychiatric symptoms during adolescence and early
Figure 2 – A) Preschooler with elongated nose. B) Preschooler with narrow palpebral fissure and thin lips. C) School-age child with elongated face and nose. D) Typical facies with narrow palpebral fissure, prominent nose, and mouth with thin lips.
386

Original Article
Grassi et al.Cardiopathies and 22q11.2 deletion syndrome
Arq Bras Cardiol. 2014; 103(5):382-390
adulthood30. These patients may also present poor academic performance, which is an important aspect to be addressed with the educational institutions.
It is imperative to disseminate warning signs for the 22q11.2DS among general pediatricians, neonatologists and pediatric cardiologists. Even though the pioneering proposal of Instituto da Criança and adopted by the Ministry of Health for detection of primary immunodeficiencies in the first year of life already includes 4 signs associated with the diagnosis of 22q11.2DS (CHD, in particular anomalies of the great vessels; lymphopenia < 2,500/mm; hypocalcemia with or without seizures; and absence of a thymic image on chest radiograph)31,32 it would be important to establish specific warning signs for this syndrome, adding phenotypic abnormalities and velopharyngeal insufficiency to the ones described above.
The current study has limitations peculiar to a transversal descriptive study, but highlights the main clinical and laboratorial findings of a highly selected population. The description of this population, however, allows us to identify and understand the demographic features of the studied group and the morbidity profile of the 22q11.2DS, and may offer data for a more adequate health policy for these patients.
The management of children with 22q11.2DS requires interaction of a multidisciplinary team of pediatrician, cardiologist, geneticist, and in some circumstances, endocrinologist, neurologist, plastic surgeon, psychologist and speech therapist.
ConclusionConsidering that in our country 2.5 million children are
born each year, we estimate that 500 to 750 new cases of 22q11.2DS should be identified yearly, which indicates that the syndrome is currently underdiagnosed. It is therefore crucial to maintain an alert for the occurrence of the syndrome in the presence of CHD associated with hypocalcemia, facial dysmorphisms, velopharyngeal insufficiency, thymic hypoplasia or absence on chest radiograph, and confirm the diagnosis by identification of the microdeletion.
Author contributionsConception and design of the research and Statistical
analysis: Grassi MS, Jacob CMA, Pastorino AC, Carneiro-Sampaio M; Acquisition of data: Grassi MS, Jacob CMA, Pastorino AC, Miura N, Jatene MB, Pegler SP, Carneiro-Sampaio M; Analysis and interpretation of the data: Grassi MS, Jacob
Figure 3 – Main phenotypic characteristics of patients with the 22q11.2 deletion syndrome. A) Narrow palpebral fissure. B) Elongated face and/or nose. C) Thin lips.
387
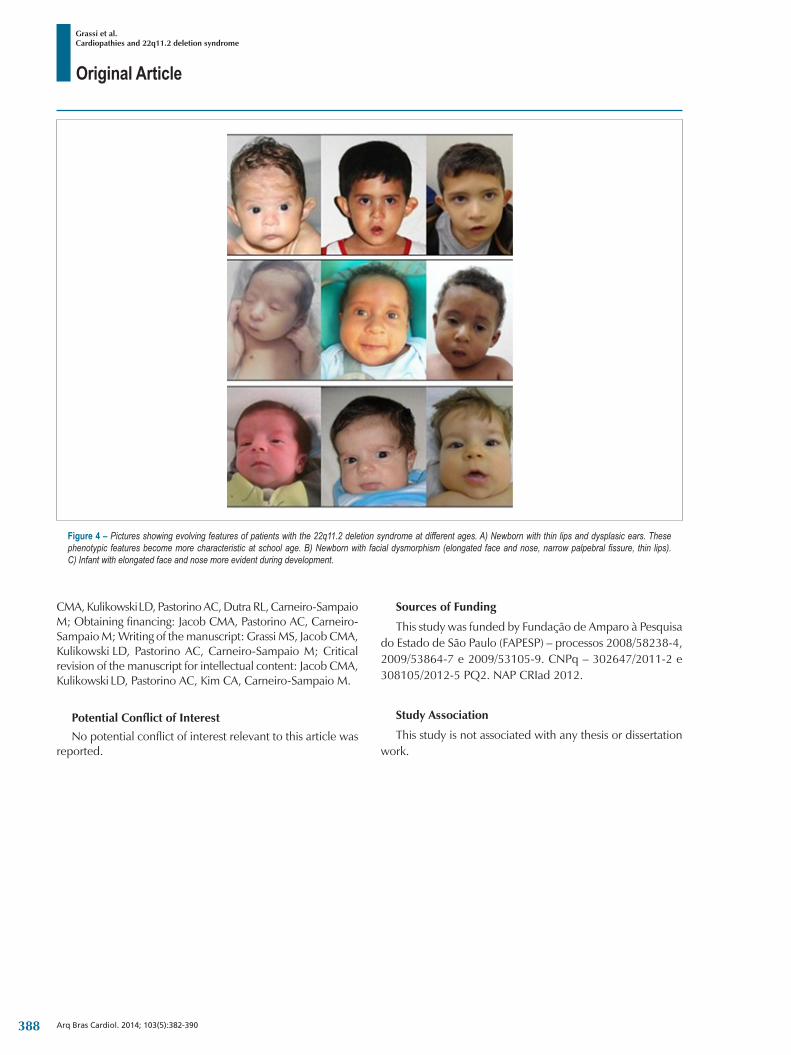
Original Article
Grassi et al.Cardiopathies and 22q11.2 deletion syndrome
Arq Bras Cardiol. 2014; 103(5):382-390
CMA, Kulikowski LD, Pastorino AC, Dutra RL, Carneiro-Sampaio M; Obtaining financing: Jacob CMA, Pastorino AC, Carneiro-Sampaio M; Writing of the manuscript: Grassi MS, Jacob CMA, Kulikowski LD, Pastorino AC, Carneiro-Sampaio M; Critical revision of the manuscript for intellectual content: Jacob CMA, Kulikowski LD, Pastorino AC, Kim CA, Carneiro-Sampaio M.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
This study was funded by Fundaçao de Amparo à Pesquisa do Estado de Sao Paulo (FAPESP) – processos 2008/58238-4, 2009/53864-7 e 2009/53105-9. CNPq – 302647/2011-2 e 308105/2012-5 PQ2. NAP CRIad 2012.
Study Association
This study is not associated with any thesis or dissertation work.
Figure 4 – Pictures showing evolving features of patients with the 22q11.2 deletion syndrome at different ages. A) Newborn with thin lips and dysplasic ears. These phenotypic features become more characteristic at school age. B) Newborn with facial dysmorphism (elongated face and nose, narrow palpebral fissure, thin lips). C) Infant with elongated face and nose more evident during development.
388

Original Article
Grassi et al.Cardiopathies and 22q11.2 deletion syndrome
Arq Bras Cardiol. 2014; 103(5):382-390
1. Gennery AR. Immunological aspects of 22q 11.2 deletion syndrome. Cell Mol Life Sci. 2012;69(1):17-27.
2. Kobrynski L, Sull ivan K. Velocardiofacial syndrome, DiGeorge syndrome: the chromosome 22q11.2 deletion syndromes. Lancet. 2007;370(9596):1443- 52.
3. Goldmuntz E. DiGeorge Syndrome: new insights. Clin Perinatol. 2005;32(4):963-78.
4. Pinkel D, Straume T, Gray JW. Cytogenetic analysis using quantitative, high-sensitivity, fluorescence hybridization. Proc Natl Acad Sci U S A. 1986;83(9):2934-8
5. Dutra RL, Honjo RS, Kulikowski LD, Fonseca FM, Pieri PC, Jehee FS, et al. Copy number variation in Williams-Beuren syndrome: suitable diagnostic strategy for developing countries. BMC Res Notes. 2012; 5:13.
6. Momma K. Cardiovascular anomalies associated with chromosome 22q11.2 deletion syndrome. Am J Cardiol. 2010;105(11):1617-24.
7. Fahed AC, Gelb BD, Seidman JG, Seidman CE. Genetics of congenital heart disease: the glass half empty. Circ Res. 2013;112(4):707-20.
8. Porto MH, Birroli MI, Duarte AJ, Carneiro-Sampaio MM. Peripheral lymphocyte subpopulations in selective IgA deficiency. Rev Hosp Clin Fac Med Sao Paulo. 1988;43(6):294-7.
9. Jacob CM, Pastorino AC, Fahl K, Carneiro-Sampaio M, Monteiro RC. Autoimmunity in IgA deficiency: revisiting the role of IgA as a housekeeper. J Clin Immunol. 2008;28(Suppl 1):S56-61.
10. Carneiro-Sampaio MM, Vasconcelos DM, Kokron CM, Jacob CM, Barros MT, Dorna MB, et al. Primary Immunodeficiency Diseases in Diferente Age Groups: A Report on 1008 Cases from a Single Brazilian Reference Center. J Clin Immunol. 2013;33(4):716-24.
11. Fomin AFB, Pastorino AC, Kim CA, Pereira CA, Carneiro-Sampaio M, Abe-Jacob CM. DiGeorge Syndrome: a not so rare disease. Clinics (Sao Paulo). 2010;65(9):865-9.
12. Karayiorgou M, Simon TJ, Gogos JA. 22q11.2 microdeletions: linking DNA structural variation to brain dysfunction and schizophrenia. Nat Rev Neurosci. 2010;1(6):402-16.
13. De la Morena MT, Eitson JL, Dozmorov IM, Belkaya S, Hoover AR, Anguiano E, et al. Signature MicroRNA expression patterns identified in humans with 22q11.2 deletion/DiGeorge syndrome. Clin Immunol. 2013;147(1):11-22.
References
Graph 2 – Distribution of values of total lymphocytes, CD4+, CD8+ and CD19+ in patients with the 22q11.2 deletion syndrome. A) Number of total lymphocytes. B) CD4+ count. C) CD8+ count. D) CD19+ count. Each dot ( • ) corresponds to an individual patient. Max: Maximum; Min: Mimum
B
max50004500
40003500
300025002000
0-6 m
onths
6-12 m
onths
1-2 ye
ars2-3
years
3-4 ye
ars4-6
years
6-9 ye
ars9-1
2 yea
rs12
-15 ye
ars15
-18 ye
ars Age
median min
1500
1000500
0
A
max12000
10000
8000
6000
4000
2000
0
0-6 m
onths
6-12 m
onths
1-2 ye
ars2-3
years
3-4 ye
ars4-6
years
6-9 ye
ars9-1
2 yea
rs12
-15 ye
ars15
-18 ye
ars Age
median min
C
max2000
18001600
14001200
1000800
0-6 m
onths
6-12 m
onths
1-2 ye
ars2-3
years
3-4 ye
ars4-6
years
6-9 ye
ars9-1
2 yea
rs12
-15 ye
ars15
-18 ye
ars Age
median min
600
400
200
0
D
max4000
3500
3000
2500
2000
1500
1000
0-6 m
onths
6-12 m
onths
1-2 ye
ars2-3
years
3-4 ye
ars4-6
years
6-9 ye
ars9-1
2 yea
rs12
-15 ye
ars15
-18 ye
ars Age
median min
500
0
Nº(x
10 /l)9
cellu
lerNº
cellu
ler (x
10 /l)9
Nº(x
10 /l)9
cellu
lerNº
célul
as (x
10 /l)9
389

Original Article
Grassi et al.Cardiopathies and 22q11.2 deletion syndrome
Arq Bras Cardiol. 2014; 103(5):382-390
14. Ryan AK, Goodship JA, Wilson DI, Philip N, Levy A, Seidel H, et al. Spectrum of clinical features associated with interstitial chromosome 22q11 deletions: a European collaborative study. J Med Genet. 1997;34(10):798-804.
15. Duke SG, McGuirt WF Jr, Jewett T, Fasano MB. Velocardiofacial syndrome: incidence of immune cytopenias. Velocardiofacial syndrome: incidence of immune cytopenias. Arch Otolaryngol Head Neck Surg. 2000;126(9):1141-5.
16. Belangero S, Bellucco F, Kulikowski L, Christofolini D, Cernach M, Melaragno M. 22q11.2 deletion in patients with conotruncal heart defect and del22q syndrome phenotype. Arq Bras Cardiol. 2009;92(4):307-11.
17. Markert ML, Devlin BH, McCarthy EA. Thymus transplantation. Clin Immunol. 2010;135(2):236-46.
18. Al-Herz W, Bousfiha A, Casanova JL, Chapel H, Conley ME, Cunningham-Rundles C, et al. Primary immunodeficiency diseases: an update on the classification from the international union of immunological societies expert committee for primary immunodeficiency. Front Immunol. 2011;2:54.
19. Edelmann L, Hirschhorn K. Clinical utility of array CGH for the detection of chromosomal imbalances associated with mental retardation and multiple congenital anomalies. Ann N Y Acad Sci. 2009;1151:157-66.
20. Aksu G, Genel F, Koturoglu G, Kurugol Z, Kutukçuler N. Serum immunoglobulin (IgG, IgM, IgA) and subclass concentrations in healthy children: a study using nephelometric technique. Turk J Pediatr. 2005;47(1):19-24.
21. van Gent R, van Tilburg CM, Nibbelke EE, Otto SA, Gaiser JF, Jansssens-Korpela PL et al. Refined characterization and reference values oh the pediatric T- and B- cell compartments. Clinical Immunol. 2009;133(1):95-107.
22. Ziolkowska L, Kawalec W, Turska-Kmiec A, Krajewska-Walasek M, Brzezinska-Rajszys G, Daszkowska J, et al. Chromosome 22q11.2 microdeletion in children with conotruncal heart defects: frequency, associated cardiovascular anomalies, and outcome following cardiac surgery. Eur J Pediatr. 2008;167(10):1135-40.
23. McDonald-McGinn DM, Kathleen E. Sullivan KE. Chromosome 22q11.2 Deletion Syndrome (DiGeorge Syndrome/ Velocardiofacial Syndrome). Medicine.(Baltimore). 2011;90(1):1-18.
24. Rosa RFM, Trevisan P, Koshiyama DB, Pillsa CB, Zens PRG, Varella- Garcia M, et al. Síndrome de deleçao 22q11 e cardiopatias congênitas complexas. Rev Assoc Med Bras. 2011;57(1):62-5.
25. Rosa RF, Zen PR, Ricachinevsky CP, Pilla CB, Pereira VL, Roman T, et al. 22q11.2 duplication and congenital heart defects. Arq Bras Cardiol. 2009;93(4):e67-9.
26. McDonald R, Dodgen A, Goyal S, Gossett JM, Shinkawa T, Uppu SC, et al. Impact of 22q11.2 deletion on the postoperative course of children after cardiac surgery. Pediatr Cardiol. 2013;34(2):341-7.
27. Pena DJ, Pietro G, Fuchshuber-Moraes M, Genro JP, Hutz MH, Kehdy FSG, et al. The genomic ancestry of individuals from different geographical regions of Brazil is more uniform than expected. PLoS One. 2011;6(2):e17063.
28. Sullivan KE. Immunologic issues in VCFS/ chromosome 22q11.2 deletion syndrome. Prog Pediatr Cardiol. 2002;15(2):103-8.
29. Patel K, Akhter J, Kobrynski L, Benjamin Gathmann MA, Davis O, Sullivan KE, et al. International DiGeorge Syndrome Immunodeficiency Consortium. Immunoglobulin deficiencies: the B-lymphocyte side of DiGeorge Syndrome. J Pediatr. 2012;161(5):950-3.
30. Drew LJ, Crabtree GW, Markx S, Stark KL, Chaverneff F, Xu B, et al. The 22q11.2 microdeletion: fifteen years of insights into the genetic and neural complexity of psychiatric disorders. Int J Dev Neurosci. 2011;29(3):259-81.
31. Carneiro-Sampaio M, Jacob CM, Leone CR. A proposal of warning signs for primary immunodeficiencies in the first year of life. Pediatr Allergy Immunol. 2011;22(3):345-6.
32. Hospital das Clínicas/FMUSP. Instituto da Criança. (Sao Paulo).12 sinais de alerta para Imunodeficiências Primárias no 1º anos de vida. [Citado em 2013 ago 26]. Disponível em: http://portal.saude.gov.br/portal/saude/visualizar_texto.cfm.dtxt =41993
390
Original Article
Impact of Intensive Physiotherapy on Cognitive Function after Coronary Artery Bypass Graft SurgeryElder dos Santos Cavalcante1, Rosmeiri Magario2, César Augusto Conforti3, Gerson Cipriano Júnior4, Ross Arena5, Antonio Carlos C. Carvalho1, Enio Buffolo1, Bráulio Luna Filho1
UNIFESP - Universidade Federal de São Paulo1; USP - Universidade de São Paulo2, SP; Santa Casa de Misericórdia de Santos3, Santos, SP; UNB - Universidade de Brasília4, DF - Brazil; Virginia Commonwealth University5, Richmond, VA - EUA
Mailing Address: Elder dos Santos Cavalcante •Av. Francisco Glicério 121, 63, Gonzaga - Postal Code 11065-402, Santos, SP – BrazilEmail: [email protected]; [email protected] Manuscript received December 8, 2013; revised manuscript May 18, 2014; accepted May 29, 2014.
DOI: 10.5935/abc.20140161
Abstract
Background: Coronary artery bypass graft (CABG) is a standard surgical option for patients with diffuse and significant arterial plaque. This procedure, however, is not free of postoperative complications, especially pulmonary and cognitive disorders.
Objective: This study aimed at comparing the impact of two different physiotherapy treatment approaches on pulmonary and cognitive function of patients undergoing CABG.
Methods: Neuropsychological and pulmonary function tests were applied, prior to and following CABG, to 39 patients randomized into two groups as follows: Group 1 (control) – 20 patients underwent one physiotherapy session daily; and Group 2 (intensive physiotherapy) – 19 patients underwent three physiotherapy sessions daily during the recovery phase at the hospital. Non-paired and paired Student t tests were used to compare continuous variables. Variables without normal distribution were compared between groups by using Mann-Whitney test, and, within the same group at different times, by using Wilcoxon test. The chi-square test assessed differences of categorical variables. Statistical tests with a p value ≤ 0.05 were considered significant.
Results: Changes in pulmonary function were not significantly different between the groups. However, while Group 2 patients showed no decline in their neurocognitive function, Group 1 patients showed a decline in their cognitive functions (P ≤ 0.01).
Conclusion: Those results highlight the importance of physiotherapy after CABG and support the implementation of multiple sessions per day, providing patients with better psychosocial conditions and less morbidity. (Arq Bras Cardiol. 2014; 103(5):391-397)
Keywords: Myocardial Revascularization / rehabilitation; Postoperative Care; Physical Therapy Speciality.
IntroductionCoronary artery bypass grafting (CABG) is effective to treat
advanced coronary artery disease (CAD), improving quality of life and prognosis of patients with that condition1-3.
Although CABG is the standard surgical option for CAD, the potential for postoperative complications may interfere with patient recovery. The most frequently complications are: pulmonary and/or cognitive function decline; infections; cardiac arrhythmias; acute myocardial infarction; and acute renal failure4. Undoubtedly, pulmonary complications are the most frequent findings4,5. The decrease in total lung capacity (TLC) and subdivisions [vital capacity (VC), functional residual
capacity (FRC), residual volume (RV) and expiratory reserve volume (ERV] following CABG may trigger complications6,7. This decrease results from the monotonous pattern of shallow breaths without periodic maximal insufflations due to respiratory drive depression caused by both anesthesia and the surgical technique8,9.
Other causes of morbidity in the postoperative period of CABG include neurological complications, which affect up to 75% of the patients5. These complications are divided into three levels: 1) cognitive changes (incidence ranging from 33% to 83%); 2) postoperative delirium (incidence ranging from 10% to 30%); and 3) stroke (incidence ranging from 1% to 6%)1,2. Affective and cognitive changes, described as changes in intellectual and behavioral functions, have been defined as comprising the inability to perform arithmetic functions, large mood swings, and explosive temper. Unfortunately, these cognitive changes have not received considerable attention, but are part of the patients’ complains as follows: “I am not the same after surgery” or “I don’t have the same disposition”2.
The mechanisms of neurocognitive changes are still a matter of debate. Possible hypotheses include cerebral hypoperfusion, cerebral macro- and microembolism, and
391

Original Article
Cavalcante et al.Physiotherapy After Coronary Artery Bypass Graft Surgery
Arq Bras Cardiol. 2014; 103(5):391-397
secondary encephalic damage due to systemic inflammatory response1,5. Investigations exploring potential interventions to maintain normal cognitive function are important, mainly when considering the negative impact of its moderate or minor loss on the patient’s quality of life10.
Although physiotherapy is considered to improve post-CABG functional mobility, its ability to prevent pulmonary and/or neurocognitive complications has not been sufficiently investigated. In addition, the frequency of the physiotherapy treatment approaches can differ, and there is no consensus on its ideal protocol. This study assessed the impact of two different physiotherapy protocols on pulmonary and neurocognitive functions of patients recently submitted to CABG11.
MethodsThis is a prospective study with patients randomized
into two subgroups of different physiotherapy treatment approaches, by use of a list made from a table of random numbers. Control patients (Group 1) underwent physiotherapy only once a day in the morning. The intensive physiotherapy group (Group 2) underwent the same treatment three times a day: morning, afternoon and early evening. This study was performed at Sao Paulo Hospital, in the city of Sao Paulo, and at Santa Casa de Misericórdia of the city of Santos, both in the state of Sao Paulo, Brazil. Approval of the local ethics committee was obtained prior to study initiation, and all patients signed a written informed consent.
ParticipantsParticipants were recruited by the cardiac surgery team.
The inclusion criterion was to undergo CABG with cardiopulmonary bypass (CPB). The exclusion criteria were as follows: emergency surgical indication for CABG; age > 74 years; left ventricular ejection fraction < 30%; and cognitive deficits preventing the performance of neurocognitive tests.
Postoperative Clinical EvaluationPostoperative complications were assessed via search in
the patients’ medical records by the same medical team and meeting standardized diagnostic criteria.
Pulmonary Function EvaluationPulmonary expiratory volumes and respiratory muscle
strength were assessed during the preoperative period, and on the third and sixth postoperative days. The last evaluation was on the day of hospital discharge. Forced vital capacity (FVC) and forced expiratory volume in the first second (FEV1) were determined with a spirometer (Microquark, Cosmed, Rome, Italy). Maximal inspiratory and expiratory pressures (MaxIP and MaxEP, respectively), which are indicators of respiratory muscle strength, were assessed with a manovacuometer (Gerar®, Sao Paulo, SP, Brazil). All procedures abided by the American Thoracic Society/European Respiratory Society Statement on respiratory muscle testing12. The pulmonary function results were interpreted by the first author (ESC), who was blind to group assignment.
Cognitive Function EvaluationThe cognitive assessment, carried out in all patients,
consisted of a battery of four tests applied by a certified psychologist (RM) in the pre- (one day before surgery) and postoperative (on the day of hospital discharge) periods. The tests included: the Digit Span Subtest of the Wechsler Adult Intelligence Scale-Revised12,13; the Benton Revised Visual Retention Test14; the Trail Making Test15; and the Digit Symbol Subtest of the Wechsler Adult Intelligence Scale-Revised12.
Those tests focused on different cognitive aptitudes. Selective attention, ability for alternating sequence, mental flexibility, and visual skill to search were assessed by using the Trail Making Test. Short-term memory, visual skill and attention were assessed by using the Digit Span Test. Recent memory and verbal immediate recall were assessed by using the Digit Symbol Test, and visual motor coordination speed, by using the Coding Test. Finally, visual memory, visual discernment and visual motor skill were assessed by using the Benton Visual Test. All these tests are acknowledged by the American Society of Neuropsychiatry13.
Patients were instructed about the tests before taking them to ensure their understanding12,15. The psychologist interpreted the cognitive tests blindly to group assignment13.
Physiotherapy ProtocolOn the first and second postoperative days, the patients
remained at the Postoperative Intensive Care Unit under the care of the cardiovascular surgery physiotherapy team and following a specific postoperative protocol. The physiotherapy protocol of this study was applied by co-authors ESC and CAC during length of stay in cardiac ward on the third postoperative day. This day was chosen to avoid interference with the medical staff of the intensive care unit.
The breathing exercises consisted of the following trainings with four sets of ten repetitions: diaphragmatic breathing pattern; and ventilatory pattern inspiration in 2 times associated with elevation of the arms. This protocol is based on respiratory kinesiotherapy.
Data AnalysisVariables were expressed as means, proportions,
standard deviation and frequency, according to their nature. Continuous variables with normal distribution were compared intragroup (same group at different times) and intergroup (Group 1 versus Group 2) by using paired and non-paired Student t tests, respectively. Chi-square test was applied for categorical variables. For variables without normal distribution, the Mann-Whitney test was used for comparison between different groups, and Wilcoxon test for intragroup analysis at different times.
Assuming a 5% alpha error and a 20% beta error, a sample of at least 18 patients in each group was estimated to be necessary to detect a 30% difference between the physiotherapy protocols evaluated. Statistical tests with p value ≤ 0.05 were considered significant. The SPSS for Windows, version 11, was used for statistical analyses.
392
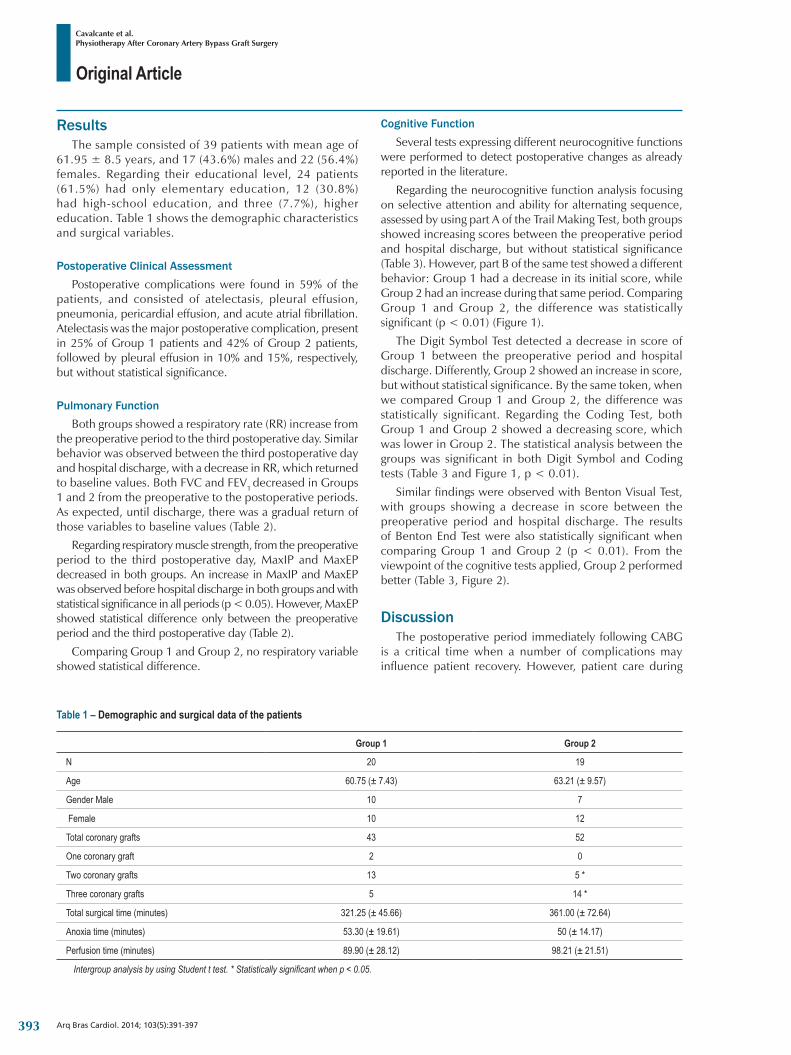
Original Article
Cavalcante et al.Physiotherapy After Coronary Artery Bypass Graft Surgery
Arq Bras Cardiol. 2014; 103(5):391-397
Table 1 – Demographic and surgical data of the patients
Group 1 Group 2
N 20 19
Age 60.75 (± 7.43) 63.21 (± 9.57)
Gender Male 10 7
Female 10 12
Total coronary grafts 43 52
One coronary graft 2 0
Two coronary grafts 13 5 *
Three coronary grafts 5 14 *
Total surgical time (minutes) 321.25 (± 45.66) 361.00 (± 72.64)
Anoxia time (minutes) 53.30 (± 19.61) 50 (± 14.17)
Perfusion time (minutes) 89.90 (± 28.12) 98.21 (± 21.51)
Intergroup analysis by using Student t test. * Statistically significant when p < 0.05.
ResultsThe sample consisted of 39 patients with mean age of
61.95 ± 8.5 years, and 17 (43.6%) males and 22 (56.4%) females. Regarding their educational level, 24 patients (61.5%) had only elementary education, 12 (30.8%) had high-school education, and three (7.7%), higher education. Table 1 shows the demographic characteristics and surgical variables.
Postoperative Clinical AssessmentPostoperative complications were found in 59% of the
patients, and consisted of atelectasis, pleural effusion, pneumonia, pericardial effusion, and acute atrial fibrillation. Atelectasis was the major postoperative complication, present in 25% of Group 1 patients and 42% of Group 2 patients, followed by pleural effusion in 10% and 15%, respectively, but without statistical significance.
Pulmonary FunctionBoth groups showed a respiratory rate (RR) increase from
the preoperative period to the third postoperative day. Similar behavior was observed between the third postoperative day and hospital discharge, with a decrease in RR, which returned to baseline values. Both FVC and FEV1 decreased in Groups 1 and 2 from the preoperative to the postoperative periods. As expected, until discharge, there was a gradual return of those variables to baseline values (Table 2).
Regarding respiratory muscle strength, from the preoperative period to the third postoperative day, MaxIP and MaxEP decreased in both groups. An increase in MaxIP and MaxEP was observed before hospital discharge in both groups and with statistical significance in all periods (p < 0.05). However, MaxEP showed statistical difference only between the preoperative period and the third postoperative day (Table 2).
Comparing Group 1 and Group 2, no respiratory variable showed statistical difference.
Cognitive FunctionSeveral tests expressing different neurocognitive functions
were performed to detect postoperative changes as already reported in the literature.
Regarding the neurocognitive function analysis focusing on selective attention and ability for alternating sequence, assessed by using part A of the Trail Making Test, both groups showed increasing scores between the preoperative period and hospital discharge, but without statistical significance (Table 3). However, part B of the same test showed a different behavior: Group 1 had a decrease in its initial score, while Group 2 had an increase during that same period. Comparing Group 1 and Group 2, the difference was statistically significant (p < 0.01) (Figure 1).
The Digit Symbol Test detected a decrease in score of Group 1 between the preoperative period and hospital discharge. Differently, Group 2 showed an increase in score, but without statistical significance. By the same token, when we compared Group 1 and Group 2, the difference was statistically significant. Regarding the Coding Test, both Group 1 and Group 2 showed a decreasing score, which was lower in Group 2. The statistical analysis between the groups was significant in both Digit Symbol and Coding tests (Table 3 and Figure 1, p < 0.01).
Similar findings were observed with Benton Visual Test, with groups showing a decrease in score between the preoperative period and hospital discharge. The results of Benton End Test were also statistically significant when comparing Group 1 and Group 2 (p < 0.01). From the viewpoint of the cognitive tests applied, Group 2 performed better (Table 3, Figure 2).
DiscussionThe postoperative period immediately following CABG
is a critical time when a number of complications may influence patient recovery. However, patient care during
393
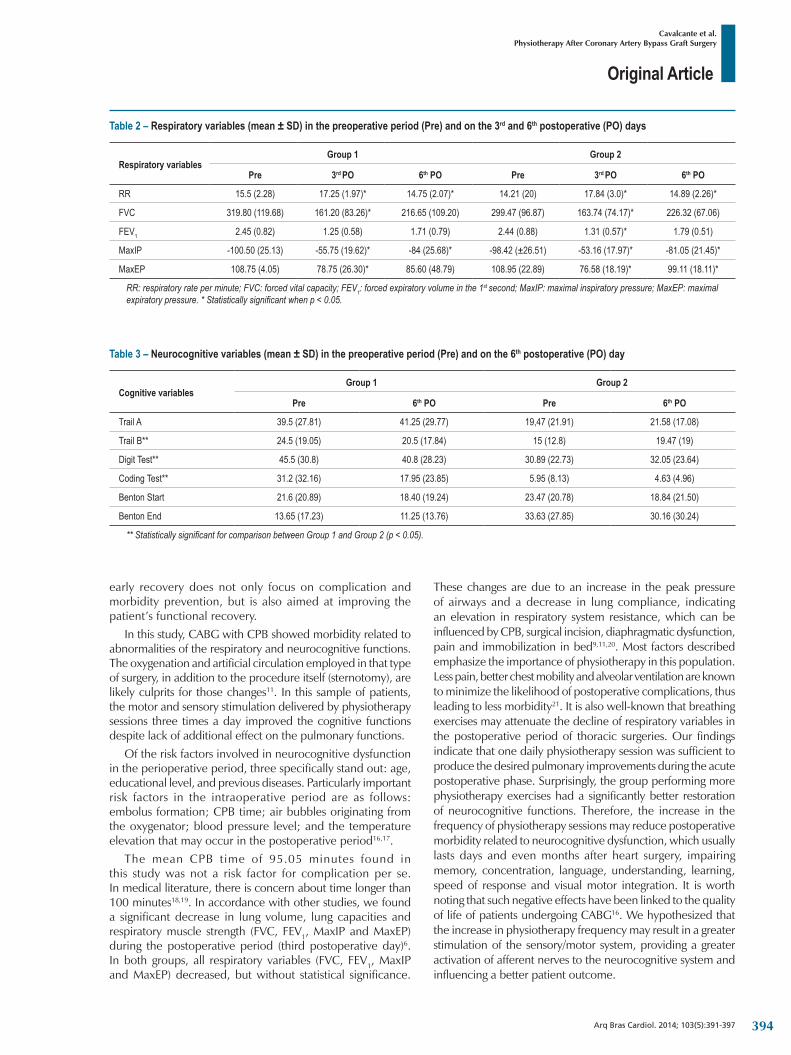
Original Article
Cavalcante et al.Physiotherapy After Coronary Artery Bypass Graft Surgery
Arq Bras Cardiol. 2014; 103(5):391-397
Table 2 – Respiratory variables (mean ± SD) in the preoperative period (Pre) and on the 3rd and 6th postoperative (PO) days
Respiratory variablesGroup 1 Group 2
Pre 3rd PO 6th PO Pre 3rd PO 6th PO
RR 15.5 (2.28) 17.25 (1.97)* 14.75 (2.07)* 14.21 (20) 17.84 (3.0)* 14.89 (2.26)*
FVC 319.80 (119.68) 161.20 (83.26)* 216.65 (109.20) 299.47 (96.87) 163.74 (74.17)* 226.32 (67.06)
FEV1 2.45 (0.82) 1.25 (0.58) 1.71 (0.79) 2.44 (0.88) 1.31 (0.57)* 1.79 (0.51)
MaxIP -100.50 (25.13) -55.75 (19.62)* -84 (25.68)* -98.42 (±26.51) -53.16 (17.97)* -81.05 (21.45)*
MaxEP 108.75 (4.05) 78.75 (26.30)* 85.60 (48.79) 108.95 (22.89) 76.58 (18.19)* 99.11 (18.11)*
RR: respiratory rate per minute; FVC: forced vital capacity; FEV1: forced expiratory volume in the 1st second; MaxIP: maximal inspiratory pressure; MaxEP: maximal expiratory pressure. * Statistically significant when p < 0.05.
Table 3 – Neurocognitive variables (mean ± SD) in the preoperative period (Pre) and on the 6th postoperative (PO) day
Cognitive variablesGroup 1 Group 2
Pre 6th PO Pre 6th PO
Trail A 39.5 (27.81) 41.25 (29.77) 19,47 (21.91) 21.58 (17.08)
Trail B** 24.5 (19.05) 20.5 (17.84) 15 (12.8) 19.47 (19)
Digit Test** 45.5 (30.8) 40.8 (28.23) 30.89 (22.73) 32.05 (23.64)
Coding Test** 31.2 (32.16) 17.95 (23.85) 5.95 (8.13) 4.63 (4.96)
Benton Start 21.6 (20.89) 18.40 (19.24) 23.47 (20.78) 18.84 (21.50)
Benton End 13.65 (17.23) 11.25 (13.76) 33.63 (27.85) 30.16 (30.24)
** Statistically significant for comparison between Group 1 and Group 2 (p < 0.05).
early recovery does not only focus on complication and morbidity prevention, but is also aimed at improving the patient’s functional recovery.
In this study, CABG with CPB showed morbidity related to abnormalities of the respiratory and neurocognitive functions. The oxygenation and artificial circulation employed in that type of surgery, in addition to the procedure itself (sternotomy), are likely culprits for those changes11. In this sample of patients, the motor and sensory stimulation delivered by physiotherapy sessions three times a day improved the cognitive functions despite lack of additional effect on the pulmonary functions.
Of the risk factors involved in neurocognitive dysfunction in the perioperative period, three specifically stand out: age, educational level, and previous diseases. Particularly important risk factors in the intraoperative period are as follows: embolus formation; CPB time; air bubbles originating from the oxygenator; blood pressure level; and the temperature elevation that may occur in the postoperative period16,17.
The mean CPB time of 95.05 minutes found in this study was not a risk factor for complication per se. In medical literature, there is concern about time longer than 100 minutes18,19. In accordance with other studies, we found a significant decrease in lung volume, lung capacities and respiratory muscle strength (FVC, FEV1, MaxIP and MaxEP) during the postoperative period (third postoperative day)6. In both groups, all respiratory variables (FVC, FEV1, MaxIP and MaxEP) decreased, but without statistical significance.
These changes are due to an increase in the peak pressure of airways and a decrease in lung compliance, indicating an elevation in respiratory system resistance, which can be influenced by CPB, surgical incision, diaphragmatic dysfunction, pain and immobilization in bed9,11,20. Most factors described emphasize the importance of physiotherapy in this population. Less pain, better chest mobility and alveolar ventilation are known to minimize the likelihood of postoperative complications, thus leading to less morbidity21. It is also well-known that breathing exercises may attenuate the decline of respiratory variables in the postoperative period of thoracic surgeries. Our findings indicate that one daily physiotherapy session was sufficient to produce the desired pulmonary improvements during the acute postoperative phase. Surprisingly, the group performing more physiotherapy exercises had a significantly better restoration of neurocognitive functions. Therefore, the increase in the frequency of physiotherapy sessions may reduce postoperative morbidity related to neurocognitive dysfunction, which usually lasts days and even months after heart surgery, impairing memory, concentration, language, understanding, learning, speed of response and visual motor integration. It is worth noting that such negative effects have been linked to the quality of life of patients undergoing CABG16. We hypothesized that the increase in physiotherapy frequency may result in a greater stimulation of the sensory/motor system, providing a greater activation of afferent nerves to the neurocognitive system and influencing a better patient outcome.
394

Original Article
Cavalcante et al.Physiotherapy After Coronary Artery Bypass Graft Surgery
Arq Bras Cardiol. 2014; 103(5):391-397
Figure 1 – Evolution of the neurocognitive functions - Trail B Test, Digit Test and Coding Test - during the preoperative period (Pre) and on the 6th postoperative (PO) day. The results are expressed as mean ± SD. The comparison between groups was performed by using Mann-Whitney Test (* p < 0.01).
**
*
* *
*
0
10
20
30
40
50
60
70
80
90
100
Perc
enta
ge
Pre 6th
Group 1 Group 2
Code
Group 1 Group 1Group 2 Group 2
Pre Pre Pre Pre6th 6th 6th 6th 6thPre
DigitTrail B
Figure 2 – Evolution of the neurocognitive functions - Benton Test Start and Benton Test End - during the preoperative period (Pre) and on hospital discharge (6th day). The results are expressed as mean ± SD. The comparison between groups was performed by using Mann-Whitney Test (* p < 0.01).
* **
*
100
90
80
70
60
50
40
30
20
10
0
Perc
enta
ge
Pre 6th
Group 1 Group 2 Group 1 Group 2
Pré 6th Pre 6th Pré 6th
Benton Start Benton End
395

Original Article
Cavalcante et al.Physiotherapy After Coronary Artery Bypass Graft Surgery
Arq Bras Cardiol. 2014; 103(5):391-397
The major exclusion criterion for this study was age older than 74 years. Neurocognitive function decline in the postoperative period (reported as up to 9%) is much more common and expected above that age. The cohort assessed in this study had a mean age of 60 years, which has been related to a smaller effect on neurocognitive functions in the postoperative period. When age was related to cognitive function, only the Digit Span test, which assesses visual motor coordination speed, found different scores, represented by a smaller one in Group 222.
In this study, some results of cognitive impairment in patients undergoing CABG with CPB differed from those reported in the medical literature. Most of the neurocognitive tests performed showed increased or slightly decreased scores between the preoperative period and hospital discharge in Group 2, which underwent much more intense and frequent physiotherapy sessions.
Evaluation of selective attention and ability for alternating sequence, assessed by using Trail Making Test, part A, in both groups showed a slight score increase between the preoperative period and hospital discharge. However, in part B of the same test, Group 2, unlike Group 1, increased its score between the preoperative period and hospital discharge, suggesting that greater stimuli improved cognitive function. Similar behavior occurred when the short-term memory and verbal immediate recall were evaluated by using Digit Symbol Test: Group 1 showed a score decrease, while Group 2 showed a score increase. When the speed of visual motor coordination and visual memory (Coding and Benton Visual Tests) were analyzed, a decline in both groups was observed, being bigger in Group 1 (p < 0.01).
The medical l i terature has reported that mild neurocognitive abnormalities may occur following cardiac surgery16. Surprisingly, some tests showed an increase in the scores of the group treated with physiotherapy three times a day. To our knowledge, this is the first study to assess the influence of physiotherapy on cognitive function. In our clinical practice, we have observed that patients undergoing cardiac surgery evolve better in relation to both pulmonary physiology and neurocognitive function when treated with more frequent physiotherapy sessions, highlighting the dynamic interaction between body and mind. This led us to plan this project in an attempt to verify whether this effect would actually occur.
Sample size is the most important study limitation. But even with a not very large number of patients and relatively simple physiotherapy protocol23, our results confirm the hypothesis that patients undergoing more physiotherapy sessions have a better cognitive restoration until hospital discharge.
We suggest that the greater amount of physiotherapy during hospitalization would increase the number of synapses in the
cortical afferent system and improve neuronal communication, resulting in the minimization or mitigation of neurocognitive disorders caused by cardiac surgery.
ConclusionAs shown in this study, CABG with CPB leads to
alterations of pulmonary and neurocognitive functions in the postoperative period that may hinder the patient’s clinical outcome. Respiratory therapy is a way to minimize the damage to lung function in this population.
Surprisingly, neurocognitive functions showed increased scores in the group undergoing more respiratory physiotherapy sessions per day, with enhanced perioperative levels, suggesting that when patients are more stimulated, they have greater neurocognitive development.
Studies correlating respiratory physiotherapy with neurocognitive function in the postoperative period of cardiac surgery lack. Our results encourage further studies on this theme. This new approach opens a new avenue of exploration, not only to the possibility of decreasing the potential damage related to the neuropsychological sphere secondary to cardiac surgery with CPB, but perhaps as a simple and practical strategy to prevent or minimize such changes.
Author contributionsConception and design of the research: Cavalcante
ES, Conforti CA, Carvalho ACC, Buffolo E, Luna Filho B; Acquisition of data: Cavalcante ES, Magario R; Analysis and interpretation of the data: Cavalcante ES, Magario R, Luna Filho B; Statistical analysis: Luna Filho B; Writing of the manuscript: Cavalcante ES, Cipriano Júnior G, Arena R, Luna Filho B; Critical revision of the manuscript for intellectual content: Cavalcante ES, Conforti CA, Cipriano Júnior G, Carvalho ACC, Buffolo E, Luna Filho B.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis article is part of the thesis of master submitted by
Elder dos Santos Cavalcante, from UNIFESP - Escola Paulista de Medicina.
396
Original Article
Cavalcante et al.Physiotherapy After Coronary Artery Bypass Graft Surgery
Arq Bras Cardiol. 2014; 103(5):391-397
1. van Harten AE, Scheeren, TW, Absalom AR. A review of postoperative cognitive dysfunction and neuroinflammation associated with cardiac surgery and anaesthesia. Anaesthesia. 2012;66(3):280-93.
2. Selnes OA, Gottesman RF, Grega MA, Baumgartner WA, Zeger SL, Mckhann GM. Cognitive and neurologic outcomes after coronary-artery bypass surgery. N Engl J Med. 2012;366(3):250-7.
3. Keenan TD, Abu-Omar Y, Taggart DP. Bypassing the pump: changing practices in coronary artery surgery. Chest. 2005;128(1):363-9.
4. Wynne R, Botti M. Postoperative pulmonary dysfunction in adults after cardiac surgery with cardiopulmonary bypass: clinical significance and implications for practice. Am J Crit Care. 2004;13(5):384-93.
5. Selnes OA, Mckhann GM. Cognitive changes after coronary artery bypass surgery. Curr Opin Psychiatry. 2002;15(3):285-90.
6. Guizilini S, Gomes WJ, Faresin SM, Bolzan DW, Alves FA, Catani R, et al. Avaliaçao da funçao pulmonar em pacientes submetidos à cirurgia de revascularizaçao do miocárdio com e sem circulaçao extracorpórea. Rev Bras Cir Cardiovasc. 2005;20(3):310-6.
7. Ng CS, Wan S, Yim AP, Arifi AA. Pulmonary dysfunction after cardiac surgery. Chest. 2002;121(4):1269-77.
8. Jackson CV. Preoperative pulmonary evaluation. Arch Intern Med. 1988;148(10):2120-7.
9. Hedenstierna G. Mechanism of postoperative pulmonary dysfunction. Acta Chir Scan Suppl. 1988;550:152-8.
10. Newman MF, Blumenthal JA. Longitudinal assessment of neurocognitive function after coronary-artery bypass surgery. N Engl J Med. 2001;344(6):395-402.
11. Renaut JA, Costa-Val R, Rossetti MB. Fisioterapia respiratória na disfunçao pulmonar pós-cirurgia cardíaca. Rev Bras Cir Cardiovasc. 2008;23(4):562-9.
12. American Thoracic Society / European Respiratory Society. ATS/ERS Statement on respiratory muscle testing. Am J Respir Crit Care Med. 2002;166(4):518-624.
13. Spreen O, Strauss E. A compendium of neuropsychological tests. New York: Oxford University Press; 1998. p. 270-9, 533-47.
14. Walsh WB, Nancy EB. Tests and assessment. Englewood Cliffs. New Jersey: Prentice Hall; 1990.
15. Lezak MD, Howieson DB, Loring DW. Neuropsychological assessment. New York: Oxford University Press; 2004.
16. Gao L, Taha R, Gauvin D, Othmen LB, Wang Y, Blaise G. Postoperative cognitive dysfunction after cardiac surgery. Chest. 2005;128(5):3664-70.
17. Martin JF, Melo RO, Sousa LP. Disfunçao cognitiva após cirurgia cardíaca. Rev Bras Cir Cardiovasc. 2008;23(2):245-55.
18. Al-Ruzzeh S, Nakamura K, Athanasiou T, Modine T, Georg S, Yacoub M, et al. Does off-pump coronary artery bypass (OPCAB) surgery improve the outcome in high-risk patients? A comparative study of 1398 high-risk patients. Eur J Cardiothorac Surg. 2003;23(1):50-5.
19. Higgins TL, Estafanous FG, Loop FD, Beck GJ, Blum JM, Paranandi L. Stratification of morbidity and mortality outcome by preoperative risk factors in coronary artery bypass patients: a clinical severity score. JAMA. 1992;267(17):2344-8. Erratum in JAMA. 1992;268(14):1860.
20. Cox CM, Ascione R, Cohen AM, Davies IM, Ryder IG, Angelini GD. Effect of cardiopulmonary bypass on pulmonary gas exchange: a prospective randomized study. Ann Thorac Surg. 2000;69(1):140-5.
21. Stiler K, Montarello J, Wallace M, Daff M, Grant R, Jenkins S, et al. Efficacy of breathing and coughing exercises in the prevention of pulmonary complications after coronary artery surgery. Chest. 1994;105(3):741-7.
22. Kadoi Y, Goto F. Factors associated with postoperative cognitive dysfunction in patients undergoing cardiac surgery. Surg Today. 2006;36(12):1053-7.
23. Matte P, Jacquet L, Van Dyk M, Goenen M. Effects of conventional physiotherapy, continuous positive airway pressure and non-invasive ventilatory support with bilevel positive airway pressure after coronary artery bypass grafting. Acta Anaesthesiol Scand. 2002;44(1):75-81.
References
397

Original Article
Association of Aortic Valve Sclerosis with Previous Coronary Artery Disease and Risk FactorsFilipe Carvalho Marmelo1, Sónia Matilde Fonseca Mateus1,2, Alexandre José Marques Pereira1,3
Escola Superior de Saúde Dr. Lopes Dias1; Hospital do Espírito Santo de Évora2; Centro Hospitalar Cova da Beira3 - Portugal
Mailing Address: Filipe Carvalho Marmelo •Rua da Ponte, 13, Potal Code 6215-439, Paul – Covilha, Castelo Branco – PortugalE-mail: [email protected] received January 11, 2013; manuscript revised July 17, 2014; accepted July 23, 2014.
DOI: 10.5935/abc.20140136
Abstract
Background: Aortic valve sclerosis (AVS) is characterized by increased thickness, calcification and stiffness of the aortic leaflets without fusion of the commissures. Several studies show an association between AVS and presence of coronary artery disease.
Objective: The aim of this study is to investigate the association between presence of AVS with occurrence of previous coronary artery disease and classical risk factors.
Methods: The sample was composed of 2,493 individuals who underwent transthoracic echocardiography between August 2011 and December 2012. The mean age of the cohort was 67.5 ± 15.9 years, and 50.7% were female.
Results: The most frequent clinical indication for Doppler echocardiography was the presence of stroke (28.8%), and the most common risk factor was hypertension (60.8%). The most prevalent pathological findings on Doppler echocardiography were mitral valve sclerosis (37.1%) and AVS (36.7%). There was a statistically significant association between AVS with hypertension (p < 0.001), myocardial infarction (p = 0.007), diabetes (p = 0.006) and compromised left ventricular systolic function (p < 0.001).
Conclusion: Patients with AVS have higher prevalences of hypertension, stroke, hypercholesterolemia, myocardial infarction, diabetes and compromised left ventricular systolic function when compared with patients without AVS. We conclude that there is an association between presence of AVS with previous coronary artery disease and classical risk factors. (Arq Bras Cardiol. 2014; 103(5):398-402)
Keywords: Heart Valve Disease/physopathology; Coronary Artery Disease; Risk Factors; Echocardiography, Doppler.
IntroductionAortic valve sclerosis (AVS) is characterized by increased
thickness, stiffness and calcification of the aortic leaflets without fusion of the commissures. Evaluation of AVS can be performed with Doppler echocardiography, and its presence can result in aortic valve stenosis, which is reflected by increased aortic systolic velocities1-4.
In contrast, acute myocardial infarction (AMI) is one of the main causes of death worldwide. This pathology is characterized by accumulation of lipid layers on the coronary artery walls through a process of atherosclerosis, resulting in limitation of blood flow to the cardiac tissue, which may cause hypoxia of this tissue and, in more critical situations, lead to cardiac muscle death4,5.
The relationship between these two pathologies is explained by a progressive release in AVS of oxidized
low-density lipoprotein that accumulates in the valves and extend through the coronary ostia towards the arteries where they are deposited, leading to coronary disease. This hypothesis is consistent with findings of histologic and immunohistochemistry studies and, even though the mechanism is not yet totally known, AVS can be used as a possible significant marker of obstructive coronary artery disease (CAD). It is also considered that this association may be explained by the involvement of risk factors common to both pathologies, such as age, gender, arterial hypertension (AH), smoking, hyperlipidemia and diabetes mellitus (DM)6.
Even though the etiological mechanisms of the aortic valve disease and the coronary disease have been documented for many years, the relationship between these two pathological entities only started to be more sharply investigated in the beginning of the 90s after observations, conducted mainly with radiological images, of calcification in the coronary vasculature and in the aortic valve7,8.
The main aim of this study is to verify whether there is an association between the presence of AVS and CAD.
MethodsThis is a transversal, retrospective and descriptive study,
based on a convenience sample obtained from a database of
398

Original Article
Marmelo et al.Association of AVS and CAD and risk factors
Arq Bras Cardiol. 2014; 103(5):398-402
the ultrasonography laboratory of Hospital do Espírito Santo de Évora. The study included 2,493 individuals with mean age of 67.5 ± 15.9 years, 50.7% of which were female, who underwent transthoracic Doppler echocardiography between August 2011 and December 2012.
The inclusion criteria for the selection of the sample were all patients undergoing transthoracic Doppler echocardiography during the period mentioned above when the aortic valvular system was evaluated. Exclusion criteria were defined as all individuals undergoing transthoracic Doppler echocardiography outside the period mentioned above, individuals undergoing transesophageal echocardiography and individuals without information regarding this variable.
The diagnoses of the pathologies that served as clinical indications for the exam, such as heart failure, pulmonary disease, AMI and stroke, were conducted by physicians based on clinical history, physical examination and diagnostic tests. Evaluations with bidimensional and Doppler echocardiogram were conducted with two ultrasonography equipments manufactured by Philips®, models IE33 and HD11 XE. AVS was defined as an increase in echogenicity and thickness of the aortic leaflets without restriction in mobility. Left ventricular systolic function was considered compromised when its value, calculated by the Simpson method, was lower than 55% of the ejection fraction. Finally, it was defined as dilatation of the left heart chambers when a left ventricular diastolic diameter was superior to 32 mm/m2 and the increase in left atrial diameter was above 40 mm9.
As for the risk factors, AH was defined as systolic pressure above 140 mmHg, dyastolic pressure above 90 mmHg, or use of medication for treatment of AH. Presence of diabetes was defined as a level of glucose above 125 mg/dl or treatment for diabetes, without distinction between types I and II diabetes. It was defined as smoker an individual with current use of tobacco and as previous smoker, those who had not used tobacco for more than one year. Dyslipidemia was defined as presence of total cholesterol level above 200 mg/dl or use of medications to treat dyslipedemia6.
Statistical analysis of all collected data was computerized with SPSS® (Statistical Package for the Social Science) for Windows®, version 20.0. Initially, a description and characterization of the studied variables was performed in order to establish a general profile of the sample. Later, an analysis of the results was conducted with a descriptive and correlative statistical analysis.
Continuous variables were defined as mean±standard deviation (X±DP) and categorical variables as number (n) and percentage (%).
The chi-square test of independence was conducted to correlate categorical variables, and the chi-square test of goodness of fit was performed to evaluate significant differences between the prevalences observed in our study with those from other studies.
The level of statistical significance used for interpretation of the tests was p ≤ 0.05 for a confidence interval of 95%.
The study was conducted with approval from the Ethics Committee of Escola Superior de Saúde Dr. Lopes Dias and Hospital Espirito Santo de Évora.
The investigation team declares that the study was conducted without external financial sources and with all the expenses paid by the authors.
ResultsThe sample of this study was composed of a total of
2,493 invidivuals with mean age of 67.5 ± 15.9 years (X±DP), of which 50.7% were females (Table 1).
In Table 2, we may observe the frequencies of the main studied variables in patients diagnosed with AVS (only main clinical indications are displayed).
As shown in Table 2, the most frequent clinical indication was stroke with 28.8%. Of the risk factors, the most frequent was AH with 60.8%, followed by hypercolesterolemia with 27%. As for the pathological results of Doppler echocardiography, mitral valve sclerosis (MVS) was the most frequent with 37.1%, followed by AVS with 36.7%.
After dividing the sample into two groups of patients with and without AVS, the chi-square test was conducted as previously described. The group with AVS was composed of 915 individuals, whereas the group without AVS had 1,578 individuals. The variables related to the clinical indications, risk factors and results of Doppler echocardiography were then compared between both groups.
Following statistical analysis and as shown in Table 3, there were important significant associations with the variables AH (p < 0.001), AMI (p = 0.007), compromised left systolic function (p < 0.001) and compromised segmentar mobility (p < 0.001). In contrast, there was no significant association with hypercholesterolemia, stroke and smoking. There was also no significant association with gender, with males showing a prevalence of AVS of 17.3% and females of 19.4%.
It is observed, therefore, a significant relationship between presence of AMI, AH, DM and compromised left systolic vertricular in patients with AVS when compared with patients without AVS.
DiscussionAs already shown in several studies, AVS may be used as a
risk marker for coronary disease. Even though its biochemical mechanism has not been completely clarified, this relationship is already widely known. Inflammatory and degerative processes are thought to affect coronary vases adjacent to this valve system and attack the arteries walls, aggravating pre-existent atherosclerotic processes1-3,6.
In the studied cohort, we could observe a balance between the prevalence of AVS in males and females (17.3% / 19.4%), which is consistent with findings from other studies. Also, the advanced mean age observed (67.5 years) confirms that AVS, as a degenerative pathology, affects mainly older age groups10.
399
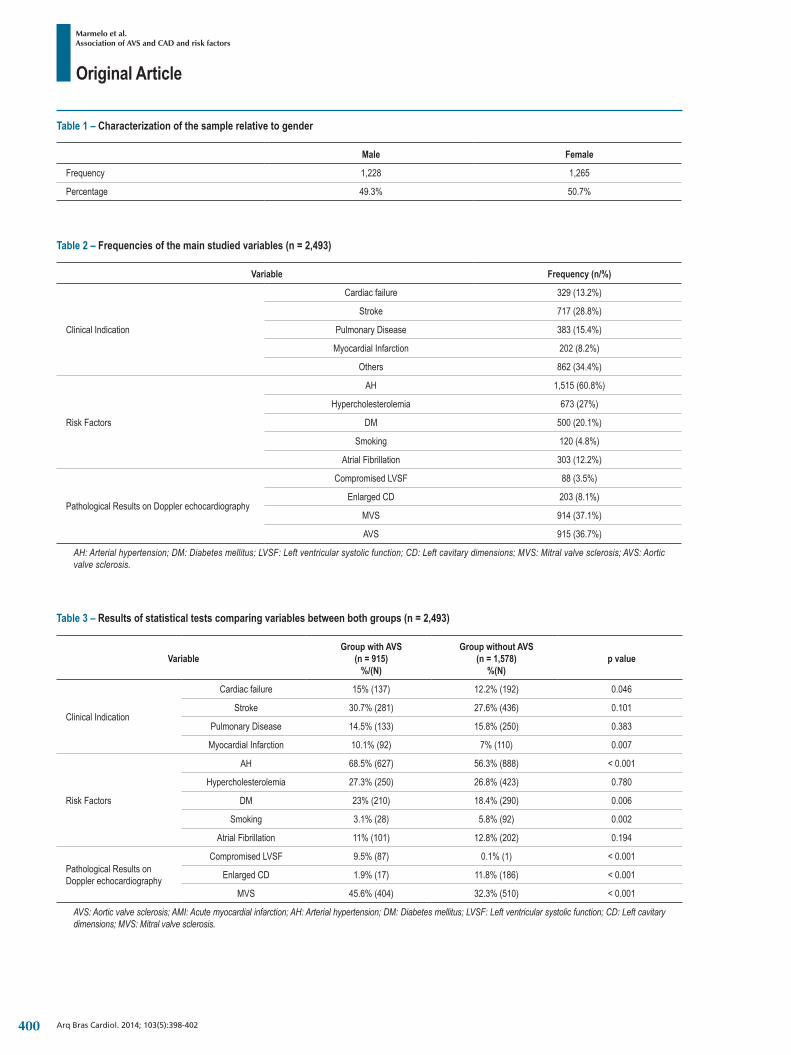
Original Article
Marmelo et al.Association of AVS and CAD and risk factors
Arq Bras Cardiol. 2014; 103(5):398-402
Table 1 – Characterization of the sample relative to gender
Male Female
Frequency 1,228 1,265
Percentage 49.3% 50.7%
Table 2 – Frequencies of the main studied variables (n = 2,493)
Variable Frequency (n/%)
Clinical Indication
Cardiac failure 329 (13.2%)
Stroke 717 (28.8%)
Pulmonary Disease 383 (15.4%)
Myocardial Infarction 202 (8.2%)
Others 862 (34.4%)
Risk Factors
AH 1,515 (60.8%)
Hypercholesterolemia 673 (27%)
DM 500 (20.1%)
Smoking 120 (4.8%)
Atrial Fibrillation 303 (12.2%)
Pathological Results on Doppler echocardiography
Compromised LVSF 88 (3.5%)
Enlarged CD 203 (8.1%)
MVS 914 (37.1%)
AVS 915 (36.7%)
AH: Arterial hypertension; DM: Diabetes mellitus; LVSF: Left ventricular systolic function; CD: Left cavitary dimensions; MVS: Mitral valve sclerosis; AVS: Aortic valve sclerosis.
Table 3 – Results of statistical tests comparing variables between both groups (n = 2,493)
VariableGroup with AVS
(n = 915)%/(N)
Group without AVS (n = 1,578)
%(N)p value
Clinical Indication
Cardiac failure 15% (137) 12.2% (192) 0.046
Stroke 30.7% (281) 27.6% (436) 0.101
Pulmonary Disease 14.5% (133) 15.8% (250) 0.383
Myocardial Infarction 10.1% (92) 7% (110) 0.007
Risk Factors
AH 68.5% (627) 56.3% (888) < 0.001
Hypercholesterolemia 27.3% (250) 26.8% (423) 0.780
DM 23% (210) 18.4% (290) 0.006
Smoking 3.1% (28) 5.8% (92) 0.002
Atrial Fibrillation 11% (101) 12.8% (202) 0.194
Pathological Results on Doppler echocardiography
Compromised LVSF 9.5% (87) 0.1% (1) < 0.001
Enlarged CD 1.9% (17) 11.8% (186) < 0.001
MVS 45.6% (404) 32.3% (510) < 0.001
AVS: Aortic valve sclerosis; AMI: Acute myocardial infarction; AH: Arterial hypertension; DM: Diabetes mellitus; LVSF: Left ventricular systolic function; CD: Left cavitary dimensions; MVS: Mitral valve sclerosis.
400

Original Article
Marmelo et al.Association of AVS and CAD and risk factors
Arq Bras Cardiol. 2014; 103(5):398-402
As for the prevalences found in this study and comparing them with other reference scientific articles regarding AVS, there was a relevant prevalence of stroke in almost one third of the sample (28.8%), which is much higher than the rate found by Otto and cols. (1999) in which the prevalence of stroke in individuals with AVS was 8%. Despite the difference in values from both studies, there was no significance in this study (p = 0.101) in contrast to the study by Otto et al11 (p = 0.003). The prevalence of AMI in that same study was 8.6%, which is almost identical to the prevalence of 8.2% in our cohort. In both studies, there was a statistical significance in comparison with the control group. As already mentioned, the sclerotic process that affects the aortic valve is similar to the aterosclerotic process in which the worsening in aortic degeneration may accelarate the development of atherosclerotic plaques in the coronary arteries located peripherally to the valvular system, thus leading to the ocurrence of symptoms associated with CAD6,11.
In the rates associated with risk factors, AH presented a prevalence of 60.8%, which is slightly inferior to 69% found by Hsu et al7, but superior to 51.7% reported by Otto et al11. As for the statistical significances between the group with and without AVS, Hsu et al7 did not observe a significant association in this variable, in contrast to the ones observed in this study (p < 0.001) and in the study by Otto et al11. The influence of AH in the development of AVS may be explained by the fact that the aortic valve in patients with AH is subjected to higher stress due to the elevated pressure exerted on the aortic leaflets, leading to damage on the endothelium of the leaflets, similar to what occurs in aterosclerotic lesions3,12.
The prevalence of hypercholesterolemia registered in this stduy was 27%, much lower when compared with the prevalence of 45% found in the study by Hsu et al7. In both studies, this variable did not present statistical significance. Comparing with the study by Ottoet al11, the prevalence of DM was 13.1%, without statistical difference when compared with the control group (p = 0.9), whereas the value found in this study was 20.1%, which showed a strong statistical significance when compared with the control group (p = 0.006). The absence of significance in hypercholesterolemia was a surprise, since the presence of cholesterol is an important factor in the process of valvular degeneration. This may have occurred due to the absence of muscular tissue in the aortic valves and to the fact that the deposition of cholesterol occurs differently than that in the coronary arteries. The absence of significance can also be explained by the low number of diagnoses established in the cohort13,14.
In the pathological resul ts found on Doppler echocardiography, a compromised left ventricular systolic function had a prevalence of 9.5%, inferior to that reported by Rosa et al10 who registered a prevalence of 17.2% with a strong statistical significance in both studies (p < 0.001).
Despite the absence of studies associating AVS and MVS, this last had a prevalence of 37.1% with a strong statistical significance. Since the organic tissues that compose the aortic valve are similar to those of the mitral valve, it would be expected that the processes that lead to the development of sclerosis could also occur in both the valves, even though
their repercussion in the coronary disease may be different due to their anatomical situation5 -17.
Finally, the prevalence of AVS was 36.7%, which is superior to 25% observed by Rosa et al10.
Based on the information presented above comparing this and several reference studies, we observe that, with the exception of hypercholesterolemia, AH and compromised left ventricular systolic function, the prevalences found in this study are superior, reinforcing the existing link between AVS with DM, AMI and stroke.
These results suggest that patients with AVS have an increased tendency to develop these clinical conditions. Medical action should focus especially in these patients in order to enhance therapies and improve measures to prevent risk factors.
ConclusionWe conclude, therefore, that there is an association between
the occurrence of AVS and previous occurrence of AMI, DM and compromised left ventricular systolic function. This confirms the main hypothesis of this study of an existing association between the presence of previous CAD and AVS, similar to the main studies in this area. This association may lead to an appreciation of the presence of AVS on ultrasonography exams, which can be considered a risk marker for suspicion of CAD6,18.
A limitation of the study is that the sample was selected in a laboratory that assists mainly a stroke unit and internal medicine inpatients, which may have influenced the prevalence of stroke. Another limitation of the study refers to the absence of multivariate analysis, which did not show significant results. As a suggestion for future studies, we propose to investigate if MVS, like AVS, could influence the occurrence of AMI and if stroke would or would not be an influence. The investigation team suggests that there could be an advantage to perform a longitudinal study about this theme.
Author contributionsConception and design of the research, Analysis and
interpretation of the data, Statistical analysis and Critical revision of the manuscript for intellectual content: Marmelo FC, Mateus SMF, Pereira AJM; Acquisition of data and Obtaining financing: Marmelo FC, Mateus SMF; Writing of the manuscript: Marmelo FC.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis article is part of the degree submitted by Filipe
Carvalho Marmelo, from Escola Superior de Saúde Dr. Lopes Dias.
401

Original Article
Marmelo et al.Association of AVS and CAD and risk factors
Arq Bras Cardiol. 2014; 103(5):398-402
1. Mahabadi AA, Bamberg F, Toepker M, Schlett CL, Rogers SI, Nagurney JT. Association of aortic valve calcification to the presence, extent and composition of coronary artery plaque burden: from the rule out myocardial infraction using computer assisted tomography; Am J Cardiol. 2009;158(4):562-8.
2. Otto C. Calcific aortic valve disease: new concepts. Semin Thoracic Cardiovasc Surg. 2010 Winter; 22(4):276-84.
3. Stewart FB, Siscovick D, Link BK, Gardin IM, Gottdiener JS, Smith VE, et al. Clinical factors associated with calcific aortic valve disease. J Am Coll Cardiol. 1997;29(3):630-4.
4. Pohle K, Maffert R, Ropers D, Moshage W, Stilianakis N, Daniel GW, et al. Progression of aortic valve calcification: association with coronary atherosclerosis and cardiovascular risk factor. Circulation. 2001; 104(16):1927-32.
5. Alexander CM, Landsman PB, Teutsch SM, Haffner SM. NCEP-Defined metabolic syndrome, diabetes anda prevalence of coronary heart disease among NHANES III participants age 50 years and older. Diabetes. 2003; 52(5):1210-4.
6. Conte L, Cicoira M, Bonapace S, Amado EA, Golia G, Zardini P. Aortic valve sclerosis: a maker of significant obstructive coronary artery disease in patients with chest pain?. J Am Soc Echocardiogr. 2007;20(6):703-8.
7. Hsu SY, Hsieh IC, Chang SH, Wen MS, Hung KC. Aortic valve sclerosis is an echocardiographic indicator of significant coronary disease in patients undergoing diagnostic coronary angiography. Int J Clin Pract. 2005; 59(1):72-7.
8. Prasad Y, Bhalodkar N. Aortic sclerosis: a maker of coronary atherosclerosis. Clin Cardiol. 2004;27(4):671-3.
9. Evangelista A, Flachskampf A, Lancellotti P, Bandano L, Aguilar R, Monaghan M, et al. European Association of Echocardiography : recommendation
for standardization of performance, digital storage and reporting of echocardiography studies. Eur J Echocardiogragr. 2008;9(4):438-48 .
10. Rosa EM, Sant’anna JRM, Oppermann LP, Castro I. Prognóstico de esclerose valvar aórtica na mortalidade cardíaca de pacientes atendidos no instituto de cardiologia do Rio Grande do Sul. Arq Bras Cardiol. 2007;88(2):234-9.
11. Otto C, Lind B, Kitzman D, Gersh B, Siscovick D. Association of aortic-valve sclerosis with cardiovascular mortality and morbidity in the elderly. N Engl J Med. 1999;341(13):142-7.
12. Lee JC, Zhao XQ, Otto C. Aortic valve sclerosis. J Echocardiogr. 2005;3(2):51-9.
13. Branch KR, O’Brien KD, Otto C. Aortic valve sclerosis as a marker of active atherosclerosis. Curr Cardiol Rep. 2002;4(2):111-7.
14. Helske S,Miettinen T, Gylling H, Mairanpaa M, Lommi J, Turto H, et al. Accumulation of cholesterol precursors and plant sterols in human stenotic valves. J Lipid Res.2008;49(7):1511-8.
15. Sociedade Brasileira de Cardiologia. Diretriz para indicaçao e utilizaçao da ecocardiografia na prática clinica. Arq Bras Cardiol. 2004;82(2):11-34.
16. Thygesen K, Alpert JS, White HD. Universal definition of myocardial infraction. J Am Coll Cardiol. 2007;50(22):2173-95.
17. Travassos TF, Sousa ACS, Barreto Fo JAS, Teles LD, Andrade FDA, Nascimento Jr A, et al.Isquemia miocárdica investigada com ecocardiografia sob estresse físico em pacientes com incompetência cronotrópica em uso de betabloqueador. Rev bras ecocardiogr imagem cardiovasc. 2010;23(2):22-30.
18. Cacodcar S, Candeias R, Pereira S, Gomes V. Alterações degenerativas na válvula aórtica sao um marcador adicional importante de aterosclerose?. Rev Port Cardiol. 200524(4):559-65.
References
402
Original Article
Prevention of Pazopanib-Induced Prolonged Cardiac Repolarization and Proarrhythmic EffectsTulay Akman1,2, Oytun Erbas3, Levent Akman4,5, Ahmet U. Yilmaz6
Tepecik Education and Research Hospital, Department of Medical Oncology1; Dokuz Eylul University, Institute of Oncology, Department of Basic Oncology2; Ege University Medical School, Department of Physiology3; Ege University Medical School, Department of Obstetrics and Gynecology4; Ege University, Institute of Health Sciences, Department of Stem Cell5; Izmir University, Medical Park Hospital, Department of Medical Oncology6
Mailing Address: Tulay Akman •Gaziler Caddesi, No: 468. Yenisehir. Postal Code 35100. Izmir. TurkeyEmail: [email protected] received April 27, 2014; revised manuscript July 1, 2014; accepted July 4, 2014.
DOI: 10.5935/abc.20140138
AbstractBackground: Pazopanib (PZP) may induce prolonged cardiac repolarization and proarrhythmic effects, similarly to other tyrosine kinase inhibitors.
Objectives: To demonstrate PZP-induced prolonged cardiac repolarization and proarrhythmic electrophysiological effects and to investigate possible preventive effects of metoprolol and diltiazem on ECG changes (prolonged QT) in an experimental rat model.
Methods: Twenty-four Sprague-Dawley adult male rats were randomly assigned to 4 groups (n = 6). The first group (normal group) received 4 mL of tap water and the other groups received 100 mg/kg of PZP (Votrient® tablet) perorally, via orogastric tubes. After 3 hours, the following solutions were intraperitoneally administered to the animals: physiological saline solution (SP), to the normal group and to the second group (control-PZP+SP group); 1 mg/kg metoprolol (Beloc, Ampule, AstraZeneca), to the third group (PZP+metoprolol group); and 1mg/kg diltiazem (Diltiazem, Mustafa Nevzat), to the fourth group (PZP+diltiazem group). One hour after, and under anesthesia, QTc was calculated by recording ECG on lead I.
Results: The mean QTc interval values were as follows: normal group, 99.93 ± 3.62 ms; control-PZP+SP group, 131.23 ± 12.21 ms; PZP+metoprolol group, 89.36 ± 3.61 ms; and PZP+diltiazem group, 88.86 ± 4.04 ms. Both PZP+metoprolol and PZP+diltiazem groups had significantly shorter QTc intervals compared to the control-PZP+SP group (p < 0.001).
Conclusion: Both metoprolol and diltiazem prevented PZP-induced QT interval prolongation. These drugs may provide a promising prophylactic strategy for the prolonged QTc interval associated with tyrosine kinase inhibitor use. (Arq Bras Cardiol. 2014; 103(5):403-409)
Keywords: Arrhythmias, Cardiac / therapy; Pyrimidines / adverse effects; Heart Conduction System / physiology; Heart / physiology.
IntroductionMulti-targeted tyrosine kinase inhibitors (TKI) have
become important for the treatment of several malignancies in the past few years1. Sorafenib is a Raf kinase inhibitor that inhibits vascular endothelial growth factor receptors 1, 2 and 3 (VEGFr-1, -2, and -3, respectively), platelet-derived growth factor receptor b (PDGFr-b), Fms-like tyrosine kinase-3 (Flt-3), and c-kit. Sunitinib inhibits VEGFr-1, -2, and -3, PDGFr-a and -b, c-kit, Flt-3, colony-stimulating factor type 1, and glial cell line-derived neurotrophic factor (GDNF) receptor (RET)2. Pazopanib is a potent multi-targeted TKI targeting VEGFr, PDGFr, and c-kit2,3. There are lots of ongoing trials with pazopanib in
different types of tumors. Pazopanib has shown monotherapy activity in advanced renal cell cancer (RCC) patients and is approved for the treatment of advanced RCC patients4.
While exploring the therapeutic index of TKIs, oncology investigators are confronted with drug adverse effects such as cardiac toxicities5. QT prolongation has drawn attention because of the risk of serious cardiac arrhythmias, such as torsade de pointes, and may be associated with ventricular arrhythmia and sudden cardiac death6.
In several studies, QTc prolongation has been observed with TKIs such as sunitinib7,8, vandetanib7,9,10, dasatinib7, crizotinib11. However there are limited data about QTc prolongation with pazopanib treatment. Metoprolol is a class 2 antiarrhythmic agent according to the Vaughan-Williams classification and a member of the group of drugs called beta-blockers12. Diltiazem is a class 4 antiarrhythmic agent and a member of the non-dihydropyridine group of drugs known as calcium channel blockers12. This study was aimed to demonstrate that pazopanib induced prolonged cardiac repolarization and to investigate the possible corrective effects of metoprolol and diltiazem on electrocardiographic changes in an experimental model.
403

Original Article
Akman et al.Proarrhythmic Effects of Pazopanib
Arq Bras Cardiol. 2014; 103(5):403-409
Table 1 – Detailed description of the groups
Groups Beginning of the study(orogastric tube)
3 hour later(intraperitoneal) 1 hour later
Group 1 (normal group) (n=6) Tap water SP
ECG records are taken
Group 2(control-PZP+SP group) (n=6) PZP SP
Group 3(PZP+metoprolol) (n=6) PZP Metoprolol
Group (PZP+diltiazem) (n=6) PZP Diltiazem
PZP: pazopanib; SP: physiological saline solution.
MethodsAfter receiving the Animal Ethics Committee’s consent, the
experiments performed in this study have been carried out according to the rules in the Guide for the Care and Use of Laboratory Animals adopted by National Institutes of Health (USA). Animals were fed ad libitum and housed in pairs in steel cages, in a temperature-controlled environment (22 ± 2 °C) with 12-h light/dark cycles. The experimental procedures were approved by the Ege University Committee for Animal Research. All animal studies strictly conformed to the animal experiment guidelines of the Committee for Humane Care.
Electrocardiograms (ECG) were recorded on male rats under anesthesia in the prone position. Electrodes consisted of 26-gauge needles placed subcutaneously for 1 cm. Standard limb leads were constructed from electrodes placed at the paws. Rats were anesthetized with a combination of 40 mg/kg of ketamine hydrochloride (Alfamine®, Ege Vet, Alfasan International B.V., Holland) and 4 mg/kg of xylazine hydrochloride (Alfazyne®, Ege Vet, Alfasan International B.V., Holland), intraperitoneally administered. Under anesthesia, ECG was taken in lead I (DI) (Biopac MP 150). Data were evaluated using Biopac Student Lab Pro software, version 3.6.7 (BIOPAC Systems, Inc.), and the parameters were as follows: QT interval, T-wave duration, and heart rate. For the calculation of QTc, Fridericia formula was used.
The rats were randomly assigned to four groups (n = 6). Table 1 shows detailed information about the groups. The first group (normal group) received 4 mL of tap water, while the other groups received 100 mg/kg of pazopanib, perorally, via orogastric tubes. Tablets containing 200 mg of pazopanib (Votrient®, GlaxoSmithKline) were crushed and suspended in tap water to yield a concentration of 10 mg/mL. According to the weight of each rat, suspended drug solution was completed to 4 mL with tap water. Three hours after the oral administration of pazopanib, the animals received intraperitoneally: physiological saline solution (SP), to the normal group and to the second group (control-PZP+SP group); 1 mg/kg of metoprolo l (Beloc, Ampule, AstraZeneca), to the third group (PZP+metoprolol group); and 1 mg/kg of diltiazem (Diltiazem, Mustafa Nevzat), to the fourth group (PZP+diltiazem group). One hour after administering those drugs, and under anesthesia, the QTc
interval was calculated by recording ECG on lead I. The observer (O.E.) who measured the QT intervals was blind to laboratory data. The QT interval was determined from the onset of the QRS complex to the end of the T wave. Six consecutive beats were evaluated, and the arithmetic means of RR and QT were obtained.
Statistical analysisResults were given as mean ± standard error of the
mean (SEM). Shapiro-Wilk test was used for checking normal distributions. All variables had normal distribution. One-Factor Analysis of Variance (ANOVA) was used to assess the groups with normally distributed continuous variables. Bonferroni adjustment for multiple comparisons was performed. Data analyses were performed using the SPSS software, version 15.0, for Windows (Chicago, IL, USA).
A p value < 0.05 was accepted as statistically significant, and a p value < 0.001, as highly statistically significant.
ResultsFigure 1 shows the ECGs of all groups, and Table 2
summarizes the QTc intervals of all groups.The QTc interval was significantly longer in the control-PZP+SP
group then in the normal group (131.23 ± 12.21 ms vs 99.93 ± 3.62 ms, respectively) (p < 0.001).
Both metoprolol and diltiazem treatments significantly shortened the QTc intervals when compared with that of the control-PZP+SP group (89.36 ± 3.61 ms, 88.86 ± 4.04 vs 131.23 ± 12.21 ms, respectively) (p < 0.001).
DiscussionSeveral molecular-targeted therapy drugs, such as
multi-targeted TKIs, histone deacetylase inhibitors, vascular-disrupting agents, farnesyl protein transferase (FTPase) inhibitors, protein kinase C inhibitors, and Src/Abl kinase inhibitors, have been found to have an effect on the QT interval13.
Long QT syndrome (LQTS) is either an inherited (congenital) or acquired disorder of the electrical system of the heart. Congenital LQTS usually results from disorders in the cardiac membrane sodium or potassium
404

Original Article
Akman et al.Proarrhythmic Effects of Pazopanib
Arq Bras Cardiol. 2014; 103(5):403-409
Figure 1 – a) ECG of normal group rats receiving only saline solution without pazopanib (PZP); b, c, d) ECG changes in rats receiving saline solution, metoprolol and diltiazem after 3 hours of PZP administration; b) QT prolongation in control group rats receiving only saline solution after PZP administration; c) QT-interval shortage in the PZP+metoprolol group; and d) QT-interval shortage in the PZP+diltiazem group. QT intervals are shown in the black areas.
405

Original Article
Akman et al.Proarrhythmic Effects of Pazopanib
Arq Bras Cardiol. 2014; 103(5):403-409
ion channels14. The clinical course of patients with LQTS is variable, owing to incomplete penetrance of QT elongation, which may or may not cause arrhythmias. Patients with LQTS may be classified into three main categories of risk for developing life-threatening cardiac events, such as torsade de pointes and cardiac arrest, as follows: very high risk, high risk, and low risk. Patients at low risk may have just QT prolongation, the risk of life-threatening cardiac events being 0,5%15. The major electrolyte imbalances associated with prolonged QT interval are hypocalcemia, hypophosphatemia, hypokalemia, and hypomagnesemia16. Usually the pharmacologic agents that cause significant QT prolongation have potassium channel blocking effects predominantly affecting the delayed rectifier repolarizing current, IK (which is the sum of two kinetically and pharmacologically distinct types of IK current components: a rapid, IKr, and a slow, IKs, component), which has a major role in the electrical activity of cardiac ventricular myocytes. IKr plays a major role in the termination of the plateau phase of the action potential and in driving cell membrane repolarization17,18. Dysfunction of these channels is determined in certain forms of inherited and acquired LQTS19.
In vitro studies have suggested that most QT-prolonging drugs block the IKr component that is encoded by hERG (human ether-a-go-go-related gene) in humans. Although functional IKr current has been found in many species, such as dogs, guinea pigs, and rabbits, there is very little (if any) functional IKr or hERG-like current in the rat ventricle20. Studies with macrolide antibiotics in rats have shown good agreement between QT-interval prolongation assessments based on rat ECG data and the clinical findings of human beings; however, those results should be carefully assessed and the existence of differences between rats and humans should be kept in mind21.
Cancer patients may be particularly prone to QT prolongation, because many of them (16% to 36%) have baseline ECG abnormalities and use concomitant drugs, such as antiemetics, antifungals or antibiotics, that can enlarge the QT interval7,9. In addition, cancer patients often have symptoms such as nausea, vomiting, diarrhea, and decreased oral intake, which may lead to electrolyte disturbances, placing the patient at risk for QT prolongation7,22.
TKIs have played an important role in the treatment of several malignancies in the past few years and provided a significant improvement in patients’ outcome1. The use of small
molecule vascular endothelial growth factor receptor-tyrosine kinase inhibitors (VEGFr-TKIs) has shown to increase the risk and the incidence of fatal adverse events (FAEs) in patients being treated for cancer. Compared with 0.7% for controls, the incidence of FAEs associated with the use of VEGFr-TKI was 1.5%. Cardiotoxicity is the second most common cause of FAEs1. The use of TKIs in the past decade has revealed a new spectrum of pro-arrhythmogenic adverse effects, QT-interval prolongation being one the most important ones7,9. QT-interval prolongation has been observed in several trials with the use of molecular-targeted agents, and QT-interval prolongation has drawn attention because of its risk of malignant cardiac arrhythmia and sudden cardiac death23.
QT-interval prolongation has been associated with several multi-targeted TKIs, such as sunitinib, vandetanib, and nilotinib7,9,10,24. In clinical studies, 2% (11/558) of patients receiving pazopanib have experienced QT-interval prolongation. Torsade de pointes has been reported in less than 1% (2/977) of those receiving pazopanib in monotherapy studies. In a randomized clinical trial, 3 of 290 patients receiving pazopanib have had post-baseline QTc-interval values between 500 and 549 ms. None of the patients receiving placebo have had post-baseline QTc-interval values greater than or equal to 500 msec25. Despite these findings French et al26 have conducted a series of detailed experiments examining the potential cardiotoxicity of sunitinib, sorafenib and pazopanib in rodents under dobutamine challenge, and have found no biochemical, mitochondrial, heart rate, ECG or echocardiographic changes in radial and circumferential strain with 12-hour monitoring. However, in a recent clinical study evaluating the effect of repeated oral doses of pazopanib on cardiac conduction in patients with solid tumors, supratherapeutic concentrations were achieved with pazopanib administration over 8 days, which produced a concentration-dependent decrease in heart rate and a concentration-independent prolongation of the QTc interval27.
Medical therapy with beta-blockers is considered to be first-line prophylactic therapy in LQTS. According to current guidelines, there is a class I indication for beta-blockers treatment among patients with a clinical diagnosis of LQTS28,29.
Different beta-blockers have similar effectiveness in preventing cardiac events in patients with LQTS30. In a different study, the authors have shown that pretreatment with diltiazem and propranolol reduce the epinephrine-induced QTc-interval prolongation31. In an animal study, the authors have put forward the beneficial effects of calcium-channel blockers
Table 2 – The values of QTc intervals of all groups
Groups QTc (ms) Heart rate (beats per minute) T duration (ms) QT duration (ms)
Normal 99.93 ± 3.62 266 ± 21.69 28.33 ± 1.21 60.83 ± 0.98
Control-PZP+SP 131.23 ± 12.21** 231.33 ± 67.95 47 ± 4.09** 85 ± 9.33**
PZP+metoprolol 89.36 ± 3.61†† 164.67 ± 27.04† 29.33 ± 2.73†† 64 ± 0.89††
PZP+diltiazem 88.86 ± 4.04†† 176.67 ± 9.30† 29.67 ± 1.36†† 62 ± 1.78††
PZP: pazopanib; SP: physiological saline solution. ** p < 0.001 control group compared with normal group, † p < 0.05 diltiazem or metoprolol group compared with control group, †† p < 0.001 diltiazem or metoprolol group compared with control group
406

Original Article
Akman et al.Proarrhythmic Effects of Pazopanib
Arq Bras Cardiol. 2014; 103(5):403-409
1. Schutz FA, Je Y, Richards CJ, Choueiri TK. Meta-analysis of randomized controlled trials for the incidence and risk of treatment-related mortality in patients with cancer treated with vascular endothelial growth factor tyrosine kinase inhibitors. J Clin Oncol. 2012;30(8):871-7.
2. Hurwitz HI, Dowlati A, Saini S, Savage S, Suttle AB, Gibson DM, et al. Phase I trial of pazopanib in patients with advanced cancer. Clin Cancer Res. 2009;15(12):4220-7.
3. Hutson TE, Davis ID, Machiels JP, De Souza PL, Rottey S, Hong BF, et al. Efficacy and safety of pazopanib in patients with metastatic renal cell carcinoma. J Clin Oncol. 2010;28(3):475-80.
4. Cook KM, Figg WD. Angiogenesis inhibitors: current strategies and future prospects. CA Cancer J Clin. 2010;60(4):222-43.
5. van Heeckeren WJ, Bhakta S, Ortiz J, Duerk J, Cooney MM, Dowlati A, et al. Promise of new vascular-disrupting agents balanced with cardiac toxicity: is it time for oncologists to get to know their cardiologists? J Clin Oncol. 20061;24(10):1485-8.
6. Haverkamp W, Breithardt G, Camm AJ, Janse MJ, Rosen MR, Antzelevitch C, et al. The potential for QT prolongation and proarrhythmia by non-antiarrhythmic drugs: clinical and regulatory implications. Report on a policy conference of the European Society of Cardiology. Eur Heart J. 2000;21(15):1216-31.
7. Strevel EL, Ing DJ, Siu LL. Molecularly targeted oncology therapeutics and prolongation of the QT interval. J Clin Oncol. 2007;25(22): 3362-71.
References
in cardiac failure and LQTS30. Furthermore, proarrhythmia and QT-interval prolongation have been predominantly demonstrated with class Ia, class Ic, and class III antiarrhythmic agents32,33. Due to the above-mentioned reasons, we selected metoprolol and diltiazem in our study34.
In the present study, we evaluated pazopanib-induced QT-interval prolongation in an experimental rat model. First, we demonstrated QTc-interval prolongation in rats treated with pazopanib alone. Three hours following drug administration, the control-group rats, which had been given pazopanib and saline solution injection intraperitoneally, showed QTc-interval elongation, thus supporting the previous studies that had shown the association of TKIs and ECG abnormalities7,9. Secondly, this study showed that the QT-prolonging effect of pazopanib can be reverted by some drugs. The PZP+metoprolol and PZP+diltiazem groups did not show QTc-interval elongation compared to the control-PZP+SP group. On the other hand, QTc intervals of both groups were significantly shorter than that of the control group, while similar results were obtained in the PZP+metoprolol and PZP+diltiazem groups. Based on the study results, both metoprolol and diltiazem were considered effective in preventing the QT-prolonging effect of pazopanib.
Treatment with QT-prolonging TKIs is frequently necessary for cancer patients. The therapy risks must be weighed against benefits. Treatment must start with withdrawal of the precipitating medication. Underlying risk factors should be assessed, administration of the possible precipitating drug must be ceased and reversible conditions, such as metabolic abnormalities, must be corrected before drug initiation34. Concurrent use of multiple QT-prolonging drugs should be avoided. Patients should be advised about the proarrhythmic risk. Periodic monitoring with ECG and close follow-up are essential for early detection and treatment in high risk patients with a history of QT-interval prolongation, patients taking antiarrhythmics, or individuals with relevant preexisting disease, such as bradycardia and electrolyte imbalances35.
Our study shows some limitations. First, this is an experimental study on rats. The question of whether or not these experimental results are also relevant to humans in the clinical setting and have therapeutic implications needs to
be further investigated. Second, in our study, no ventricular stability test was performed. Because of this limitation, the potential prophylactic effects of the drugs against proarrhythmia cannot be evaluated according to our results. Therefore, different studies with specific models of ventricular stability are needed for the recommendation of these drugs for prophylactic use.
A better knowledge about potential cardiac side effects of pazopanib and the identification of patients at higher risk are required to reduce cardiotoxicity with that agent. In the present study, the preventing effects of metoprolol and di l t iazem on pazopanib-induced QT-interval prolongation were evaluated.
In conclusion, both metoprolol and diltiazem significantly shortened pazopanib-induced QT-interval prolongation. Although metoprolol and diltiazem prevented QT-interval prolongation, long-term studies including ventricular stability test in different models can provide evidence for the prophylactic use of those drugs in high risk patients treated with pazopanib.
Author contributionsConception and design of the research and Obtaining
financing: Akman T, Erbas O, Akman L, Yilmaz AU; Acquisition of data, Analysis and interpretation of the data and Statistical analysis: Akman T, Erbas O, Akman L; Writing of the manuscript and Critical revision of the manuscript for intellectual content: Akman T, Yilmaz AU.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis study is not associated with any thesis or dissertation work.
407

Original Article
Akman et al.Proarrhythmic Effects of Pazopanib
Arq Bras Cardiol. 2014; 103(5):403-409
8. Bello CL, Mulay M, Huang X, Patyna S, Dinolfo M, Levine S, et al. Electrocardiographic characterization of the QTc interval in patients with advanced solid tumors: pharmacokinetic- pharmacodynamic evaluation of sunitinib. Clin Cancer Res. 2009;15(22):7045-52.
9. Ederhy S, Cohen A, Dufaitre G, Izzedine H, Massard C, Meuleman C, et al. QT interval prolongation among patients treated with angiogenesis inhibitors. Target Oncol. 2009;4(2):89-97.
10. Brassard M, Rondeau G. Role of vandetanib in the management of medullary thyroid cancer. Biologics. 2012;6:59-66.
11. Ou SH, Azada M, Dy J, Stiber JA. Asymptomatic profound sinus bradycardia (heart rate ≤ 45) in non-small cell lung cancer patients treated with crizotinib. J Thorac Oncol. 2011;6(12):2135-7.
12. The Sicilian gambit. A new approach to the classification of antiarrhythmic drugs based on their actions on arrhythmogenic mechanisms. Task Force of the Working Group on Arrhythmias of the European Society of Cardiology. Circulation. 1991;84(4):1831-51.
13. Ederhy S, Izzedine H, Massard C, Dufaitre G, Spano JP, Milano G, et al. Cardiac side effects of molecular targeted therapies: towards a better dialogue between oncologists and cardiologists. Crit Rev Oncol Hematol. 2011;80(3):369-79.
14. Neyroud N, Tesson F, Denjoy I, Leibovici M, Donger C, Barhanin J, et al. A novel mutation in the potassium channel gene KVLQT1 causes the Jervell and Lange-Nielsen cardioauditory syndrome. Nat Genet. 1997;15(2):186-9.
15. Goldenberg I, Moss AJ. Long QT syndrome. J Am Coll Cardiol. 2008;51(24):2291-300.
16. Khan IA. Clinical and therapeutic aspects of congenital and acquired long QT syndrome. Am J Med. 2002;112(1):58-66.
17. Priebe L, Beuckelmann DJ. Cell swelling causes the action potential duration to shorten in guinea-pig ventricular myocytes by activating IKATP. Pflugers Arch. 1998;436(6):894-8.
18. Tomaselli GF, Marbán E. Electrophysiological remodeling in hypertrophy and heart failure. Cardiovasc Res. 1999;42(2):270-83.
19. Sanguinetti MC. Dysfunction of delayed rectifier potassium channels in an inherited cardiac arrhythmia. Ann N Y Acad Sci. 1999;868:406-13.
20. McDermott JS, Salmen HJ, Cox BF, Gintant GA. Importance of species selection in arrythmogenic models of Q-T interval prolongation. Antimicrob Agents Chemother. 2002;46(3):938-9.
21. Ohtani H, Taninaka C, Hanada E, Kotaki H, Sato H, Sawada Y, Iga T. Comparative pharmacodynamic analysis of Q-T interval prolongation induced by the macrolides clarithromycin, roxithromycin, and azithromycin in rats. Antimicrob Agents Chemother. 2000;44(10):2630-7.
22. Yusuf SW, Razeghi P, Yeh ET. The diagnosis and management of cardiovascular disease in cancer patients. Curr Probl Cardiol. 2008;33(4):163-96.
23. Haverkamp W, Brei thardt G, Camm AJ, Janse MJ, Rosen MR, Antzelevi tch C, et a l . The potent ia l for QT prolongat ion and pro-arrhythmia by non-anti-arrhythmic drugs: clinical and regulatory implications. Report on a Policy Conference of the European Society of Cardiology. Cardiovasc Res. 2000;47(2):219-33.
24. Rock EP, Goodman V, Jiang JX, Mahjoob K, Verbois SL, Morse D, et al. Food and drug administration drug approval summary: sunitinib malate for the treatment of gastrointestinal stromal tumor and advanced renal cell carcinoma. Oncologist. 2007;12(1):107-13.
25. Highlights of prescribing information. 2009. Votrient US prescribing information. [Cited in 2014 Jan 10]. Available from: http://us.gsk.com/products/assets/us_votrient.pdf
26. French KJ, Coatney RW, Renninger JP, Hu CX, Gales TL, Zhao S, et al. Differences in effects on myocardium and mitochondria by angiogenic inhibitors suggest separate mechanisms of cardiotoxicity. Toxicol Pathol. 2010;38(5):691-702.
27. Heath EI, Infante J, Lewis LD, Luu T, Stephenson J, Tan AR, et al. A randomized, double-blind, placebo-controlled study to evaluate the effect of repeated oral doses of pazopanib on cardiac conduction in pat ients with sol id tumors. Cancer Chemother Pharmacol. 2013;71(3):565-73.
28. Zipes DP, Camm AJ, Borggrefe M, Buxton AE, Chaitman B, Fromer M, et al.; European Heart Rhythm Association; Heart Rhythm Society, American College of Cardiology; American Heart Association Task Force; European Society of Cardiology Committee for Practice Guidelines. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death). J Am Coll Cardiol. 2006;48(5):e247-346.
29. Barsheshet A, Dotsenko O, Goldenberg I. Genotype-specific risk stratification and management of patients with long QT syndrome. Ann Noninvasive Electrocardiol. 2013;18(6):499-509.
30. Schwartz PJ. Pharmacological and non-pharmacological management of the congenital long QT syndrome: the rationale. Pharmacol Ther. 2011;131(1):171-7.
31. Darbar D, Smith M, Mörike K, Roden DM. Epinephrine-induced changes in serum potassium and cardiac repolarization and effects of pretreatment with propranolol and diltiazem. Am J Cardiol. 1996;77(15):1351-5.
32. Redfern WS, Carlsson L, Davis AS, Lynch WG, Mackenzie I, Redfern WS, et al. Relationships between preclinical cardiac electrophysiology, clinical QT-interval prolongation and torsade de pointes for a broad range of drugs: evidence for a provisional safety margin in drug development. Cardiovasc Res. 2003;58(1):32-45.
33. Stanton MS, Prystowsky EN, Fineberg NS, Miles WM, Zipes DP, Heger JJ. Arrhythmogenic effects of antiarrhythmic drugs: a study of 506 patients treated for ventricular tachycardia or fibrillation. J Am Coll Cardiol. 1989;14(1):209-15.
34. Shantsila E, Watson T, Lip GY. Drug-induced QT-interval prolongation and proarrhythmic risk in the treatment of atrial arrhythmias. Europace. 2007;9 Suppl 4:iv37-44.
35. Brana I, Tabernero J. Cardiotoxicity. Ann Oncol. 2010;21 Suppl 7:vii173-9.
408

Original Article
Akman et al.Proarrhythmic Effects of Pazopanib
Arq Bras Cardiol. 2014; 103(5):403-409409

Original Article
Hemodynamic Effects of Noninvasive Ventilation in Patients with Venocapillary Pulmonary HypertensionAndré Moreira Bento, Luiz Francisco Cardoso, Flávio Tarasoutchi, Roney Orismar Sampaio, Luiz Junya Kajita, Pedro Alves Lemos NetoInstituto do Coração do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, São Paulo, SP – Brazil
Mailing Address: André Moreira Bento •Rua Capote Valente, 349, conjunto 125, Pinheiros, Postal Code: 05409-001, Sao Paulo, SP - BrazilE-mail: [email protected] received April 14, 2014; revised manuscript July 14, 2014; accepted July 22, 2014.
DOI: 10.5935/abc.20140147
Abstract
Background: The hemodynamic effects of noninvasive ventilation with positive pressure in patients with pulmonary hypertension without left ventricular dysfunction are not clearly established.
Objectives: Analyze the impact of increasing airway pressure with continuous positive airway pressure on hemodynamic parameters and, in particular, on cardiac output in patients with variable degrees of pulmonary hypertension.
Methods: The study included 38 patients with pulmonary hypertension caused by mitral stenosis without left ventricular dysfunction or other significant valvulopathy. The hemodynamic state of these patients was analyzed in three conditions: baseline, after continuous positive pressure of 7 cmH2O and, finally, after pressure of 14 cmH2O.
Results: The population was composed of predominantly young and female individuals with significant elevation in pulmonary arterial pressure (mean systolic pressure of 57 mmHg). Of all variables analyzed, only the right atrial pressure changed across the analyzed moments (from the baseline condition to the pressure of 14 cmH2O there was a change from 8 ± 4 mmHg to 11 ± 3 mmHg, respectively, p = 0.031). Even though there was no variation in mean cardiac output, increased values in pulmonary artery pressure were associated with increased cardiac output. There was no harmful effect or other clinical instability associated with use application of airway pressure.
Conclusion: In patients with venocapillary pulmonary hypertension without left ventricular dysfunction, cardiac output response was directly associated with the degree of pulmonary hypertension. The application of noninvasive ventilation did not cause complications directly related to the ventilation systems. (Arq Bras Cardiol. 2014; 103(5):410-417)
Keywords: Hypertension, Pulmonary; Heart Failure; Noninvasive Ventilation; Hemodynamics.
IntroductionNoninvasive positive pressure ventilation (CPAP) is a
mode of ventilation commonly applied to a large spectrum of clinical situations. Its use has already been described both in patients in critical conditions such as acute pulmonary congestion, acute respiratory failure in patients with chronic pulmonary disease and during recovery from cardiac and non-cardiac surgeries, and in chronic patients with obstructive sleep apnea.
It is known that, in general, application of airway pressure may benefit the hemodynamic condition of patients with pulmonary congestion and left ventricular systolic dysfunction primarily by increasing cardiac output1-3. This effect has been attributed mainly to an elevation in intrathoracic pressure and
consequent reduction in left ventricular afterload, improving the systolic function of this chamber2,4. The ultimate impact from use of CPAP in the cardiac performance of patients with previous systolic dysfunction is of a complex nature and reflects the interaction between the compromised heart and the intrathoracic vasculature. In fact, this intricate relationship can be even more complex in the presence of venocongestive pulmonary hypertension.
In contrast, in the presence of pulmonary hypertension, invasive mechanical ventilation has been associated with unfavorable hemodynamic effects5. Therefore, patients with pulmonary hypertension due to pulmonary venocapillary congestion may be subject to unpredictable hemodynamic effects during application of airway pressure.
Still today, the hemodynamic effects of CPAP in patients without left ventricular dysfunction have not been entirely described. Particularly in patients with pulmonary hypertension, a subclass of patients often encountered in daily clinical practice, the impact of CPAP has been poorly characterized. Even though its use is widely accepted as benefical in patients with sleep apnea and some elevation in pulmonary pressure, its effects have not yet been completely described in a population with marked pulmonary hypertension6,7.
410

Original Article
Bento et al.Hemodynamic effects of NIV in patients with PH
Arq Bras Cardiol. 2014; 103(5):410-417
The aim of this study, therefore, is to analyse the impact of increasing airway pressure with CPAP on hemodynamic parameters in patients with variable degrees of pulmonary hypertension. In particular, the primary aim is to evaluate the effects of CPAP on the cardiac output of patients with chronic pulmonary hypertension.
Methods
Studied cohort This study included a total of 38 patients with pulmonary
hypertension (resting systolic pulmonary arterial pressure equal to or higher than 30 mmHg) confirmed by cardiac catheterization. In order to homogenize the cohort, the analysis included only patients with pulmonary hypertension caused by mitral stenosis who were selected to undergo balloon catheter mitral valvuloplasty (BCMV). The selection was conducted according to medical history, physical examination and echocardiogram with two-dimensional color Doppler. This last was conducted in all patients up to 3 months before the invasive evaluation. Patients with left ventricular dysfunction, any greater than mild valvular heart disease, and left atrial thrombus were excluded. The consent term was obtained from all patients and the study was approved by the Ethics Committee of our institution.
ProtocolPatients were evaluated in the catheterization laboratory
immediately before BCMV. Analgesia was only performed with local lidocaine infiltration on the puncture site and sedative medications were avoided. Hemodynamic parameters were obtained in the supine position on three moments: 1) at baseline, in ambient air; 2) 5 minutes after CPAP set at 7 cmH2O; and 3) 5 minutes after CPAP set at 14 cmH2O. Noninvasive ventilation was delivered with a CPAP equipment (Solo LX Deluxe, Respironics Inc, USA) and oronasal mask (model Comfortfull, Respironics Inc, USA).
In each of the three conditions, heart rate and rhythm, as well as digital oximetry were measured continuously with a multiparameter monitor. Right atrial pressure, pulmonary arterial pressure and pulmonary capillary pressure were measured with a 7-Fr Swan-Ganz catheter (Edwards Laboratories, Santa Ana, USA), inserted via the right femoral vein. Systemic arterial and left ventricular pressures were measured with a 5-Fr pigtail catheter inserted via the left femoral artery. All measurements were performed at the end of expiration and the pressure transducers were zeroed at the level of the mid-axillary line.
Cardiac output was calculated by thermodilution as a mean of three measurements obtained after injection of 10 mL of 5% dextrose solution randomly performed during the respiratory cycle. If one of the measurements differed in more than 10% of the mean, two other cardiac output measurements were determined and the highest and lowest values were discarded for calculation of the mean. Samples of arterial and venous blood gases were collected from the aorta and the pulmonary artery, respectively. The derived hemodynamic and oxymetric variables were calculated from standard formulas.
Statistical analysisCategorical variables were shown in tables with absolute
(n) and relative (%) frequencies, whereas quantitative variables were presented as mean and standard deviation.
Quantitative variables, measured on each of the three conditions (baseline, CPAP 7 cmH2O and CPAP 14 cmH2O), were presented in tables as means and standard deviations and were evaluated with analysis of variance with repeated measurements. When significant, contrasts of maximum likelihood were conducted to discriminate the differences.
Correlation coefficients were calculated to evaluate the variation in cardiac output with echocardiographic and hemodynamic parameters.
P values < 0.05 were considered statistically significant.Sample size was calculated using the software G Power
3.1 with the formula for calculation of samples of repeated measures. A statistical power of 80%, significance level of 5%, and an effect (f) size of 0.25 were estipulated. This way, the minimum number of individuals was defined as 33.
ResultsThirty-eight patients with mitral stenosis and pulmonary
hypertension followed as outpatients were recruited for this research. The population was composed of individuals predominantly young, females and with significant elevation in pulmonary arterial pressure, with a mean pulmonary arterial pressure of 57 mmHg. Table 1 presents the clinical and echocardiographic characteristics of the cohort, whereas Table 2 presents hemodynamic and blood gases data (Tables 1 and 2).
Variation in cardiac outputTable 2 also shows the stability of the mean value
of the variables that represent left ventricular systolic capacity, cardiac output, cardiac index and systolic volume. Even though the mean cardiac output values of the cohort showed no variation across all three conditions, there was a significant variation among the patients. It was not possible, therefore, to identify the factors that modulated its variation during different moments of the study. The interactions between baseline characteristics and the effect of CPAP on the cardiac output are presented in Table 3. In the analysis of the use of CPAP set at 7 cmH2O, it was not possible to identify at baseline variables associated with the variation in cardiac output. However, in the analysis of the use of CPAP set at 14 cmH2O, the pressures in the pulmonary system and the oxygen saturation were associated with changes in cardiac output. The pressures in the pulmonary system were the main determinants of the changes in cardiac output, with increase in cardiac output in those with increased levels of pulmonary hypertension (Graphs 1 to 3). The arterial oxygen saturation of hemoglobin was also associated with changes in cardiac output across the studied conditions (Graph 4).
There was no association between the variation in cardiac output and the nonparametric variables functional class (p = 0.07 for CPAP 7 cmH2O and p = 0.14 for CPAP 14 cmH2O) and presence of atrial fibrillation (p = 0.77 for CPAP 7cmH2O and p = 0.52 for CPAP 14 cmH2O).
411

Original Article
Bento et al.Hemodynamic effects of NIV in patients with PH
Arq Bras Cardiol. 2014; 103(5):410-417
Table 1 – Demographic and echocardiographic features
Age, years 38.9 ± 11.8
Female gender 33 (87%)
NYHA class II 24 (63%)
NYHA class III or IV 14 (37%)
Chronic atrial fibrillation 4 (10%)
Systemic arterial hypertension 3 (8%)
Mitral valve area, cm2 0.9 ± 0.2
Ejection fraction, % 69 ± 6
Left ventricular end-diastolic diameter, mm 47 ± 4
Left atrial diameter, mm 48 ± 4
Table 2 – Hemodynamic and blood gases data before and after CPAP
Baseline CPAP 7 cmH2O CPAP 14 cmH2O p
Heart rate, beats/min 86 ± 16 85 ± 16 83 ± 16 0.686
Systolic systemic pressure, mmHg 117 ± 15 119 ± 14 120 ± 16 0.710
Diastolic systemic pressure, mmHg 73 ± 10 75 ± 11 76 ± 11 0.542
Systolic pulmonary pressure, mmHg 57 ± 24 58 ± 24 58 ± 24 0.957
Diastolic pulmonary pressure, mmHg 30 ± 14 31 ± 13 32 ± 13 0.883
Pulmonary capillary pressure, mmHg 27 ± 10 27 ± 9 27 ± 9 0.961
Right atrial pressure, mmHg 8 ± 4 9 ± 4 11 ± 3 0.035 *
Cardiac output, l/min 4.6 ± 1.2 4.6 ± 1.1 4.5 ± 1.2 0.877
Cardiac index, l/min/m2 2.7 ± 0.7 2.7 ± 0.6 2.6 ± 0.7 0.838
Indexed systolic volume, ml/beat/m2 32.3 ± 8.1 32.4 ± 8.0 32.1 ± 7.0 0.987
Arterial oxygen saturation, % 95.2 ± 2.9 95.6 ± 2.1 96.0 ± 2.1 0.330
Mixed venous oxygen saturation, % 69.6 ± 7.5 69.6 ± 7.0 69.2 ± 7.2 0.950
* Significant variation only in the comparison between baseline and CPAP set at 14 cmH2O.
Table 3 – Correlation between baseline characteristics and effect of CPAP on cardiac output variation
CPAP 7 cmH2O CPAP 14 cmH2O
Baseline parameters Correlation of Pearson p Correlation of Pearson p
Mitral valve area, cm2 -0.257 0.12 -0.250 0.13
Left ventricular ejection fraction, % 0.000 0.99 0.300 0.07
Left ventricular diastolic diameter, mm 0.200 0.22 0.094 0.83
Left atrial diameter, mm 0.074 0.66 -0,073 0.66
Heart rate, beats/min 0.920 0.58 0.304 0.06
Systolic systemic pressure, mmHg 0.019 0.91 0.279 0.09
Diastolic systemic pressure, mmHg 0.027 0.87 0.192 0.25
Systolic pulmonary pressure, mmHg 0.210 0.20 0.516 0.001
Diastolic pulmonary pressure, mmHg 0.209 0.21 0.509 0.001
Pulmonary capillary pressure, mmHg 0.245 0.14 0.528 0.001
Right atrial pressure, mmHg 0.115 0.49 0.088 0.60
Arterial oxygen saturation, % -0.244 0.14 -0.387 0.02
Mixed venous oxygen saturation, % -0.276 0.09 -0.310 0.06
Variation in hemodynamic parameters across the conditionsAs for hemodynamic modifications during the different
moments of the study, only right atrial pressure showed variation. From baseline to CPAP 14 cmH2O, there was an increase from 8 ± 4 mmHg to 11 ± 3 mmHg, respectively (p = 0.031). In contrast, compared with baseline, the increase with CPAP 7 cmH2O was not significant (p = 0.993). Despite a trend towards an increase, there was no expressive variation in values of systemic arterial and pulmonary arterial pressures. Other clinically relevant parameters, such as heart rate and oxygen saturation, also did not show modifications along the study.
It is important to highlight that no harmful effect was observed. There was no occurrence of clinical instability associated with use of CPAP. In addition, all patients, after
412

Original Article
Bento et al.Hemodynamic effects of NIV in patients with PH
Arq Bras Cardiol. 2014; 103(5):410-417
a brief explanation about the use of CPAP, tolerated its application satisfactorily during the study.
DiscussionThe main result of this study was the association of the
pressures in the pulmonary system as the main determinants of the variation in cardiac output with CPAP use in a population of patients with pulmonary hypertension. As expected, the hemodynamic changes were more evident with application of higher levels of airway pressure. In the analysis during CPAP set at 7 cmH2O, none of the variables correlated with changes in cardiac output. Following that, the evaluation during CPAP set at 14 cmH2O showed the importance of the pulmonary hypertension in cardiac output response. Higher values of systolic, diastolic and occlusion pulmonary arterial pressures were associated with increased cardiac output.
The association between higher values of pulmonary artery occlusion pressure (PAOP) and positive response to use of CPAP has been previously documented by other authors in a population with a very distinct hemodynamic profile. Baratz et al1, during a study with patients with idiopathic myocardiopathy after use of CPAP set at 5 cmH2O, identified two groups of patients. The first group, with PAOP equal to or higher than 12 mmHg, responded with an increase of 17% in cardiac output. The second group of patients with PAOP below 12 mmHg, presented a reduction of 8% in cardiac output. Bradley et al3 confirmed this concept, observing that the use of CPAP set at 5 to 10 cmH2O caused an elevation in cardiac output proportional to the level of pressure offered in patients with cardiac failure and elevated PAOP. These studies have in common with the present study the association between higher PAOP values and positive response to use of CPAP. However, only patients with left ventricular dysfunction were included, which was a condition excluded in the current study. It is known that the reduction in left ventricular afterload imposed by CPAP may be particularly advantageous in the presence of systolic dysfunction. In contrast, in patients with pulmonary hypertension and respiratory failure, it is known that mechanical ventilation with positive pressure can impose negative hemodynamic effects. The increase in pulmonary volume and decrease in functional residual capacity can increase the pulmonary vascular resistance and, consequently, the right ventricular output impedance, mainly in patients with pre-existent right ventricular failure5. The acute effects of noninvasive ventilation in patients with extreme pulmonary hypertension are not well described. Even though the use of CPAP has been extensively studied in patients with sleep apnea syndrome, this condition is usually associated with a more mild pulmonary hypertension than that observed in the current study6,7. In a study that included 20 patients without cardiac or pulmonary pathologies, only five of these patients fulfilled the criteria of pulmonary hypertension. In this study, the mean pulmonary artery pressure of the group was 16.8 mmHg6. In 40 patients with obstructive sleep apnea and pulmonary hypertension studied by Laks et al8, the pulmonary artery systolic pressure estimated by ecochardiogram ranged from 20 to 52 mmHg and the mean was only 29 mmHg8. A study with only nine
patients with respiratory failure due to decompensation of chronic obstructive pulmonary disease were studied with hemodynamic monitoring during application of noninvasive ventilation with pressure support and positive end-expiratory pressure (PEEP)9. There was a significant decrease in cardiac output associated with use of PEEP set at 5 cmH2O. However, even though all patients presented at least moderate pulmonary hypertension, the mean pulmonary artery pressure was 27 mmHg, which was much below the value found in our study.
Up to where an extensive review of the literature allows us to consider, the evaluation of the acute hemodynamic effects of noninvasive ventilation in patients with such marked pulmonary hypertension had not yet been conducted. Although our sample, composed of patients with severe mitral stenosis, may represent a profile of patients with preserved left ventricular systolic performance associated with venocapillary pulmonary hypertension, it is not possible to determine whether other etiologies of pulmonary hypertension without left ventricular dysfunction would respond similarly to use of CPAP.
Another important result of this study was that use of CPAP was safe in the conditions applied in the current study, similarly to what has been described by other authors. Only right atrial pressure presented a significant variation during application of airway pressure. In the conditions evaluated in this study, there were no significant variations in relevant clinical parameters, such as heart rate, systemic arterial pressure, cardiac output, pulmonary arterial pressure and arterial oxygen saturation. After the researchers explained the procedures to the patients, including details of aspects related to noninvasive ventilation, use of CPAP was well tolerated, even at a pressure of 14 cmH2O. There were no cases in which noninvasive ventilation had to be removed by request from the patient. It should also be highlighted that there was no register of complication related directly to the use of pressurized ventilation systems.
The use of noninvasive ventilation has been shown capable to reduce the need for intubation, length of stay and ICU mortality in patients with hypoxemic acute respiratory failure. This is due to its effects on the hemodynamic status and pulmonary mechanics. With respect to the respiratory system, its application has as main physiological benefits the decrease in respiratory work, in addition to an improve in oxygenation. As for the clinical applicability of the current study, considering that the respiratory benefits of CPAP would be maintained, the small variation in relevant hemodynamic parameters favors use of CPAP in patients with hypoxemic respiratory failure and hemodynamic profile similar to that in this study.
Study limitationsThe main limitation of the study was the fact that the
patients were clinically stable during the study procedures. Usually, the application of noninvasive ventilation is indicated in patients with respiratory failure. Therefore, with regard to the best scientific methodology, the ideal would be to evaluate the hemodynamic conditions of patients with pulmonary congestion before any treatment and during noninvasive ventilation. However, this approach
413
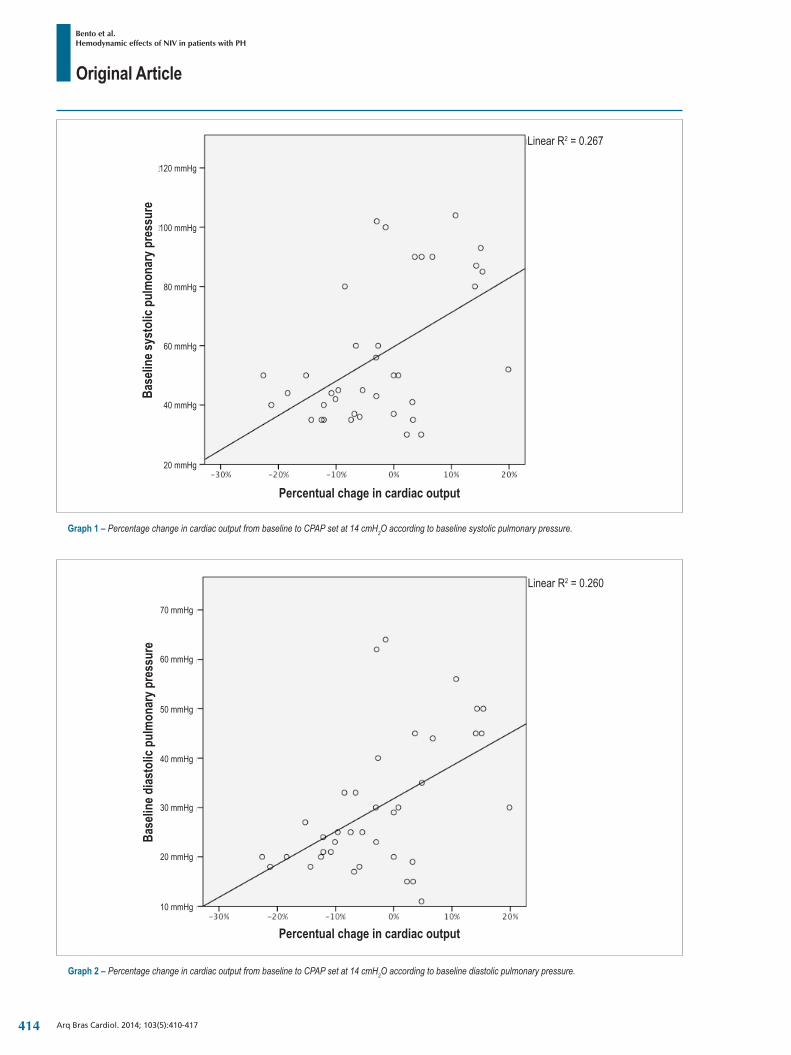
Original Article
Bento et al.Hemodynamic effects of NIV in patients with PH
Arq Bras Cardiol. 2014; 103(5):410-417
Graph 1 – Percentage change in cardiac output from baseline to CPAP set at 14 cmH2O according to baseline systolic pulmonary pressure.
Linear R2 = 0.267
Percentual chage in cardiac output
Base
line s
ysto
lic p
ulm
onar
y pre
ssur
e120 mmHg
100 mmHg
80 mmHg
60 mmHg
40 mmHg
20 mmHg
Graph 2 – Percentage change in cardiac output from baseline to CPAP set at 14 cmH2O according to baseline diastolic pulmonary pressure.
Linear R2 = 0.260
Base
line d
iasto
lic p
ulm
onar
y pre
ssur
e
Percentual chage in cardiac output
70 mmHg
10 mmHg
20 mmHg
30 mmHg
40 mmHg
50 mmHg
60 mmHg
414
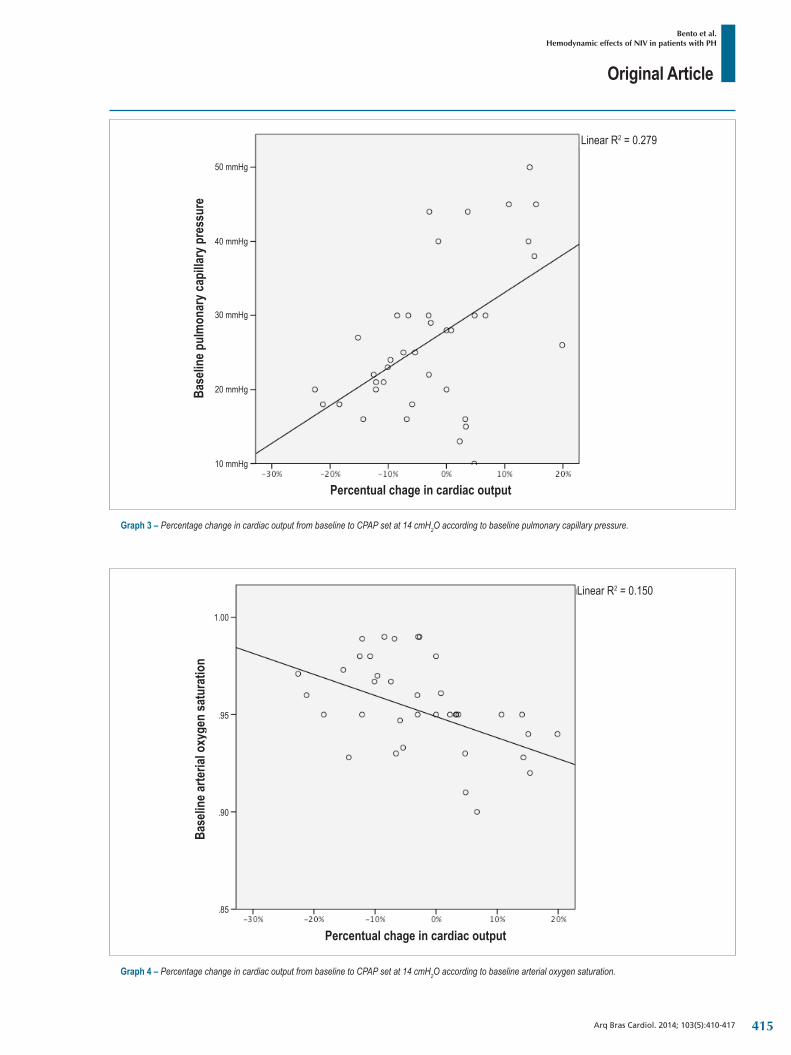
Original Article
Bento et al.Hemodynamic effects of NIV in patients with PH
Arq Bras Cardiol. 2014; 103(5):410-417
Graph 3 – Percentage change in cardiac output from baseline to CPAP set at 14 cmH2O according to baseline pulmonary capillary pressure.
Linear R2 = 0.279
Base
line p
ulm
onar
y cap
illary
pre
ssur
e
Percentual chage in cardiac output
50 mmHg
10 mmHg
20 mmHg
30 mmHg
40 mmHg
Graph 4 – Percentage change in cardiac output from baseline to CPAP set at 14 cmH2O according to baseline arterial oxygen saturation.
Linear R2 = 0.150
Base
line a
rteria
l oxy
gen
satu
ratio
n
Percentual chage in cardiac output
.85
1.00
.95
.90
415

Original Article
Bento et al.Hemodynamic effects of NIV in patients with PH
Arq Bras Cardiol. 2014; 103(5):410-417
1. Baratz DM, Westbrook PR, Shah PK, Mohsenifar Z. Effect of nasal continuous positive pressure on cardiac output and oxygen delivery in patients with congestive heart failure. Chest. 1992;102(5):1397-401.
2. Naughton MT, Rahman MA, Hara K, Floras JS, Bradley TD. Effect of continuous positive airway pressure on intrathoracic and left ventricular transmural pressures in patients with congestive heart failure. Circulation. 1995;91(6):1725-31.
3. Bradley TD, Holloway RM, McLaughlin PR, Ross BL, Walters J, Liu PP. Cardiac output response to continuous positive airway pressure in congestive heart failure. Am Rev Respir Dis. 1992;145(2 Pt 1):377-82.
4. Buda AJ, Pinsky MR, Ingeis NB, Daughters GJ, Stinson EB, Alderman EL. Effect of intrathoracic pressure on left ventricular performance. N Engl J Med. 1979;301(9):453-9.
5. Zamanian RT, Haddad F, Doyle RL, Weinacker AB. Management strategies for patients with pulmonary hypertension in the intensive care unit. Crit Care Med. 2007;35(9):2037-50.
6. Sajkov D, Cowie RJ, Thornton AT, Espinoza HA, McEvoy RD. Pulmonary hypertension and hypoxemia in obstructive sleep apnea syndrome. Am J Respir Crit Care Med. 1994;149(2 Pt 1):416-22.
7. Arias MA, Garcia-Rio F, Alonso-Fernandez A, Martinez I, Villamor J. Pulmonary hypertension in obstructive sleep apnoea: effects of continuous positive airway pressure: a randomized, controlled cross-over study. Eur Heart J. 2006;27(9):1106-13.
8. Laks L, Lehrhaft B, Grunstein RR, Sullivan CE. Pulmonary hypertension in obstructive sleep apnea. Eur Respir J. 1995;8(4):537-41.
9. Ambrosino N, Nava S, Torbick A, Riccardi G, Fracchia C, Opasich C, et al. Haemodynamic effects of pressure support and PEEP ventilation by nasal route in patients with stable chronic obstructive pulmonary disease. Thorax. 1993;48(5):523-8.
References
was not possible due to a series of factors. First, it would be risky to keep a patients with pulmonary congestion without adequate treatment while invasive monitoring is provided. Second, the great majority of the patients with pulmonary congestion and/or acute pulmonary edema do not require invasive monitoring as part of the therapy. Monitoring is related to a number of complications that would increase the risk to the patient and would, therefore, imply in a questionable ethical judgment. Finally, this strategy would limit substantially the number of selectable patients, jeopardizing the viability of the study. It is also worth mentioning that even though the study was not performed in patients with clinical instability, nothing prevents its value to be extended to this situation.
ConclusionIn patients with mitral stenosis, venocapillary pulmonary
hypertension and without left ventricular dysfunction, the cardiac output response to use of CPAP was directly associated with the degree of pulmonary hypertension. The application of CPAP did not incur in complications directly related to the ventilation systems.
Author contributionsConception and design of the research: Bento AM, Cardoso
LF, Tarasoutchi F, Sampaio RO, Kajita LJ; Acquisition of data: Bento AM, Cardoso LF, Sampaio RO, Kajita LJ; Analysis and interpretation of the data and Statistical analysis: Bento AM, Cardoso LF, Lemos Neto PA; Writing of the manuscript: Bento AM, Cardoso LF; Critical revision of the manuscript for intellectual content: Bento AM, Tarasoutchi F, Sampaio RO, Lemos Neto PA.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis article is part of the thesis of Doctoral submitted by
André Moreira Bento, from Instituto do Coraçao do Hospital das Clínicas da Universidade de Sao Paulo.
416

Original Article
Bento et al.Hemodynamic effects of NIV in patients with PH
Arq Bras Cardiol. 2014; 103(5):410-417 417

Original Article
Physical Stress Echocardiography: Prediction of Mortality and Cardiac Events in Patients with Exercise Test showing IschemiaAna Carla Pereira de Araujo 1, Bruno F. de Oliveira Santos1, Flavia Ricci Calasans1, Ibraim M. Francisco Pinto2, Daniel Pio de Oliveira2, Luiza Dantas Melo1, Stephanie Macedo Andrade1, Irlaneide da Silva Tavares1, Antonio Carlos Sobral Sousa1,3, Joselina Luzia Menezes Oliveira1, 2, 3
Universidade Federal de Sergipe (UFS)1, Aracaju, SE; Instituto Dante Pazzanese de Cardiologia2, São Paulo, SP; Hospital São Lucas3, Aracaju, SE - Brazil
Abstract
Background: Studies have demonstrated the diagnostic accuracy and prognostic value of physical stress echocardiography in coronary artery disease. However, the prediction of mortality and major cardiac events in patients with exercise test positive for myocardial ischemia is limited.
Objective: To evaluate the effectiveness of physical stress echocardiography in the prediction of mortality and major cardiac events in patients with exercise test positive for myocardial ischemia.
Methods: This is a retrospective cohort in which 866 consecutive patients with exercise test positive for myocardial ischemia, and who underwent physical stress echocardiography were studied. Patients were divided into two groups: with physical stress echocardiography negative (G1) or positive (G2) for myocardial ischemia. The endpoints analyzed were all-cause mortality and major cardiac events, defined as cardiac death and non-fatal acute myocardial infarction.
Results: G2 comprised 205 patients (23.7%). During the mean 85.6 ± 15.0-month follow-up, there were 26 deaths, of which six were cardiac deaths, and 25 non-fatal myocardial infarction cases. The independent predictors of mortality were: age, diabetes mellitus, and positive physical stress echocardiography (hazard ratio: 2.69; 95% confidence interval: 1.20 – 6.01; p = 0.016). The independent predictors of major cardiac events were: age, previous coronary artery disease, positive physical stress echocardiography (hazard ratio: 2.75; 95% confidence interval: 1.15 – 6.53; p = 0.022) and absence of a 10% increase in ejection fraction. All-cause mortality and the incidence of major cardiac events were significantly higher in G2 (p < 0. 001 and p = 0.001, respectively).
Conclusion: Physical stress echocardiography provides additional prognostic information in patients with exercise test positive for myocardial ischemia. (Arq Bras Cardiol. 2014; 103(5):418-425)
Keywords: Echocardiography, Stress/mortality; Exercise Test; Physical Exertion; Coronary Artery Disease; Myocardial Ischemia.
IntroductionCoronary artery disease (CAD) is the major cause of morbidity
and mortality in Western countries1. In Brazil, cardiovascular diseases account for more than 30% of deaths2. Since new effective therapeutic options are now available, the identification of patients at a higher risk for cardiovascular events is mandatory3. Although coronary angiography remains the gold-standard for the diagnosis of CAD4, non-invasive techniques play a key role in the diagnosis and in the indication of invasive procedures.
Myocardial ischemia and infarction occur as a result of sequential changes known as “ischemic cascade”. Perfusion
abnormalities are followed by metabolic changes, left ventricular (LV) diastolic dysfunction, regional contraction deficit, electrocardiographic abnormalities and chest pain5. The ischemic cascade may be understood as a spectrum throughout which different markers of myocardial ischemia may show different sensitivity6,7.
Exercise test (ET) is the noninvasive test initially recommended for the diagnosis and risk stratification of patients with suspected CAD8-10. However, the use of ET is limited in several situations such as in the presence of left bundle branch block (LBBB) or of ST-segment abnormalities in resting electrocardiogram (ECG)10, thus requiring the association of imaging methods to improve the diagnostic accuracy11.
Physical stress echocardiography (PSE) has high sensitivity and specificity, and is more accurate than ECG, ET and resting echocardiography in the detection of CAD12,13. LV wall motion abnormalities (WMA) detected by PSE occur earlier than angina or ST-segment abnormalities14. Additionally, PSE also has an additional value in the location and quantification of myocardial ischemia as well as in the prediction of adverse events in patients with established CAD15.
Mailing Address: Irlaneide da Silva Tavares •R-15, N 08, Residencial Parque dos Coqueiros, Inácio Barbosa. Postal Code 49040-293, Aracaju, SE – BrazilE-mail: [email protected] Manuscript received November 03, 2013; revised manuscript received March 25, 2014; accepted June 02, 2014.
DOI: 10.5935/abc.20140144
418

Original Article
Araújo et al.Mortality and cardiac events on stress-echo
Arq Bras Cardiol. 2014; 103(5):418-425
The objective of this study was to analyze the effectiveness of PSE in predicting mortality and major cardiac events (MCE) in patients with ET showing ischemia.
Methods
PatientsA total of 866 consecutive patients referred for PSE in
the Laboratory of Echocardiography of Sao Lucas Hospital, Aracaju (SE), after their respective physicians had detected electrocardiographic signs of myocardial ischemia on ET, were included between January 2001 and June 2010. The exclusion criteria were: ET negative for myocardial ischemia; presence of LBBB; failure to confirm ischemia by ET (repeated as PSE protocol); patient refusal to participate in the study; and failure to establish phone contact during the follow-up period.
The protocol consisted of complete clinical assessment with investigation of previous symptoms such as chest pain or shortness of breath, as well as risk factors for CAD, followed by ECG and resting echocardiography. Then, the patients underwent physical exertion on a treadmill and new echocardiographic images were acquired. Clinical and demographic data, as well as the results of the stress tests were recorded in the database. The individuals were divided into two groups according to the absence (G1) or presence (G2) of myocardial ischemia on PSE.
Exercise testAfter a light meal, the patients were examined and advised
not to practice any excessive physical activity on the day the test was performed. The study was performed with the individuals breathing spontaneously in room air, at a constant temperature (20 to 24°C). The Bruce protocol was used to perform ET. During the test, the individuals were continuously monitored by three-lead ECG, and were encouraged to reach their peak physical exertion. ET was considered as positive for myocardial ischemia whenever ST-segment elevation or horizontal or downsloping ST-segment depression ≥ 1 mm was detected for at least 60 to 80 ms of J point10.
Physical stress echocardiographyEchocardiographic studies were performed using
Packard/Phill ips Hewlett SONOS 5500 equipment according to the technical specifications described by Schiller et al16. Two-dimensional echocardiographic images were obtained with the patient in the left lateral position, in the parasternal and apical acoustic windows, at rest and immediately after exercise, with simultaneous electrocardiographic recording in videocassette or digital video, and assessed by an experienced echocardiographer (level III), as recommended by the American Society of Echocardiography17. In cases of doubt, the images were analyzed by a second, equally experienced, examiner.
Wall motion was scored from 1 to 4 (1 if normal, 2 if hypokinesia, 3 if akinesia, and 4 if dyskinesia), according to a 16-segment model. The wall motion index (WMI)
was determined at rest and at peak exercise as the sum of segmental scores divided by the number of segments visualized. Left ventricular systolic function was quantified, based on WMI, as: 1 if normal; 1.1 to 1.6 if mild ventricular dysfunction; 1.61 to 2 if moderate ventricular dysfunction; and > 2 if severe ventricular dysfunction16. The difference between exercise and resting WMI was named ΔWMI; it was considered normal when equal to zero, and abnormal when different from zero. Any result showing the development of new motion abnormalities induced by exercise or worsening of a preexisting contractile deficit, that is, every ΔWMI different from zero was considered as myocardial ischemia on PSE; absence of myocardial ischemia was defined as the absence of the criteria described above, that is, ΔWMI equal to zero.
Follow-up and endpointsPatients were followed-up by means of telephone
interviews, contact with the assisting physician, or medical record review. All-cause death and MCE were considered as study endpoints; MCE were defined as cardiac death and non-fatal acute myocardial infarction (AMI).
Statistical analysisCategorical variables were described as percentages
and compared between groups using the chi-square or Fisher’s exact test. Continuous variables were described as mean and standard deviation (SD), and the differences between groups were analyzed using the Student’s t test or Mann-Whitney test, as appropriate. The cumulative events curves were estimated using the Kaplan-Meier method and compared using the log-rank test. To evaluate the risk factors for MCE and death, Cox regression was used, considering univariate and multivariate analyses. The variables included in the multivariate model were those with p < 0.1 in the univariate analysis. Differences were considered significant when p < 0.05. The statistical analyses were carried out using the Statistical Package for the Social Sciences (SPSS) program, version 17.0 (Chicago, IL).
The study was carried out in compliance with the ethical principles for human experimentation and the patients gave written informed consent. The study was approved by the Research and Ethics Committee of Federal University of Sergipe (CAAE 1818.0.000.107-06).
Results
Clinical characteristics of the study populationThe population comprised 866 patients with ST-segment
abnormalities during ET, and who underwent PSE. The patients were divided into two groups, one with 661 (76.3%) patients without ischemia on PSE (ΔWMI = 0) (G1), and the other with 205 (23.7%) patients with ischemia (ΔWMI ≠ 0) (G2). In G1, the mean age of patients was 55.97 ± 11 years, and 298 (45.1%) were men; in G2, the mean age was 58.96 ± 9.83 years, and 87 (42.4%) were men. G2 patients had significantly higher BMI (p = 0.002), age (p < 0.001), and presence of suggestive chest pain
419

Original Article
Araújo et al.Mortality and cardiac events on stress-echo
Arq Bras Cardiol. 2014; 103(5):418-425
Table 1 – Clinical characteristics of patients with and without myocardial ischemia on physical stress echocardiography
Variables G1n = 661 (76.3%)
G2n = 205 (23.7%) p value
Male gender, n (%) 298 (45.1) 87 (42.4) 0.506
Age, years 55.97 ± 10.58 58.96 ± 9.83 0.001
BMI, kg/m2 27.13 ± 4.05 28.14 ± 4.30 0.002
Suggestive chest pain, n (%) 25 (3.8) 53 (26.0) 0.001
Non-suggestive chest pain, n (%) 391 (59.3) 98 (48.0) 0.004
Obesity, n (%) 137 (21.2) 53 (26.1) 0.141
Hypertension, n (%) 341 (51.7) 129 (63.2) 0.004
Diabetes mellitus, n (%) 76 (11.5) 42 (20.6) 0.001
Dyslipidemia, n (%) 428 (64.8) 152 (74.5) 0.001
Smoker, n (%) 34 (5.2) 15 (7.4) 0.235
Family history of CAD, n (%) 361 (54.7) 133 (65.2) 0.008
Previous diagnosis of CAD, n (%) 75 (11.3) 31 (15.1) 0.150
Use of betablocker, n (%) 121 (18.4) 49 (23.9) 0.081
Use of calcium antagonist, n (%) 34 (5.2) 16 (7.8) 0.152
G1: Patients without myocardial ischemia; G2: Patients with myocardial ischemia; BMI: body mass index; CAD: coronary artery disease.
(p < 0.001) in relation to G1; non-suggestive chest pain was more frequent in G1 (p = 0.004). Additionally, there were significantly more patients with hypertension (p = 0.004), diabetes mellitus (p = 0.001), dyslipidemia (p = 0.01), and family history of CAD (p = 0.008) in G2. No other significant differences were observed between the groups regarding their clinical characteristics (Table 1).
Three out of four positive ET did not show ischemia on PSE, i.e., approximately 75% of the study patients were better analyzed.
Hemodynamic and echocardiographic measurementsG2 showed a significantly lower peak heart rate (HR)
(p < 0.001), higher resting WMA (p = 0.036), higher exercise WMI and higher ΔWMI (p < 0.001). In relation to the other hemodynamic and echocardiographic parameters, there were no significant differences between G1 and G2 (Table 2).
Follow-up and endpointsDuring the mean 85.6 ± 15.0-month follow-up, there
were 26 all-cause death, of which seven in G1 (sudden death, sepsis, stroke, airway obstruction and neoplasia), and 19 in G2 (kidney failure, sepsis, pancreatitis and neoplasia); additionally, there were 31 MCE (one cardiac death and five AMI in G1, and five cardiac deaths and 20 AMI in G2). As regards overall mortality, in the univariate analysis the significant variables were: age ≥ 60 years (p < 0.001), diabetes mellitus (p = 0.001), resting WMA (p = 0.003), positive PSE (p = 0.001) and left ventricular mass index (LVMI; p < 0.001).
As regards MCE, the significant variables in univariate analysis were: male gender (p = 0.044), age ≥ 60 years (p < 0.001), typical chest pain (p = 0.030), atypical chest pain (p = 0.017),
diabetes mellitus (p = 0.005), dyslipidemia (p = 0.019), previous CAD (p < 0.001), resting WMA (p < 0.001), positive PSE (p < 0.001), LV ejection fraction (LVEF; p < 0.001), LVMI (p = 0.006) and ΔWMI (p = 0.042). (Table 3). In the multivariate analysis, the independent predictors of mortality were age ≥ 60 years, and positive PSE. The independent predictors of MCE were age ≥ 60 years, previous CAD, positive PSE, and absence of a 10% increase in EF (Tables 4 and 5).
For MCE, there was a significant difference between groups G1 vs. G2, with p = 0.022. For overall mortality, there was also a significant difference between groups G1 vs. G2, with p = 0.016.
Mortality and MCE curves are shown in Figures 1 and 2, respectively.
DiscussionThis study has demonstrated that PSE is an independent
predictor of death and MCE in patients with ET showing ischemia. The independent predictors of mortality after multivariate analysis were: age ≥ 60 years, diabetes mellitus, and positive PSE. Predictors of MCE were age ≥ 60 years and previous CAD. Several studies have demonstrated the clinical characteristics described above as well-established risk factors for CAD18-21 and as predictors of adverse events in patients with stable or suspected angina or established CAD22-24. Our results corroborate these previous findings.
Echocardiographic findings have the ability to demonstrate pathophysiological changes resulting from myocardial ischemia in earlier phases and are, therefore, more sensitive than clinical results and ECG changes25. In this study, we found an important association of suggestive pain in patients with myocardial ischemia on PSE and on MCE.
420
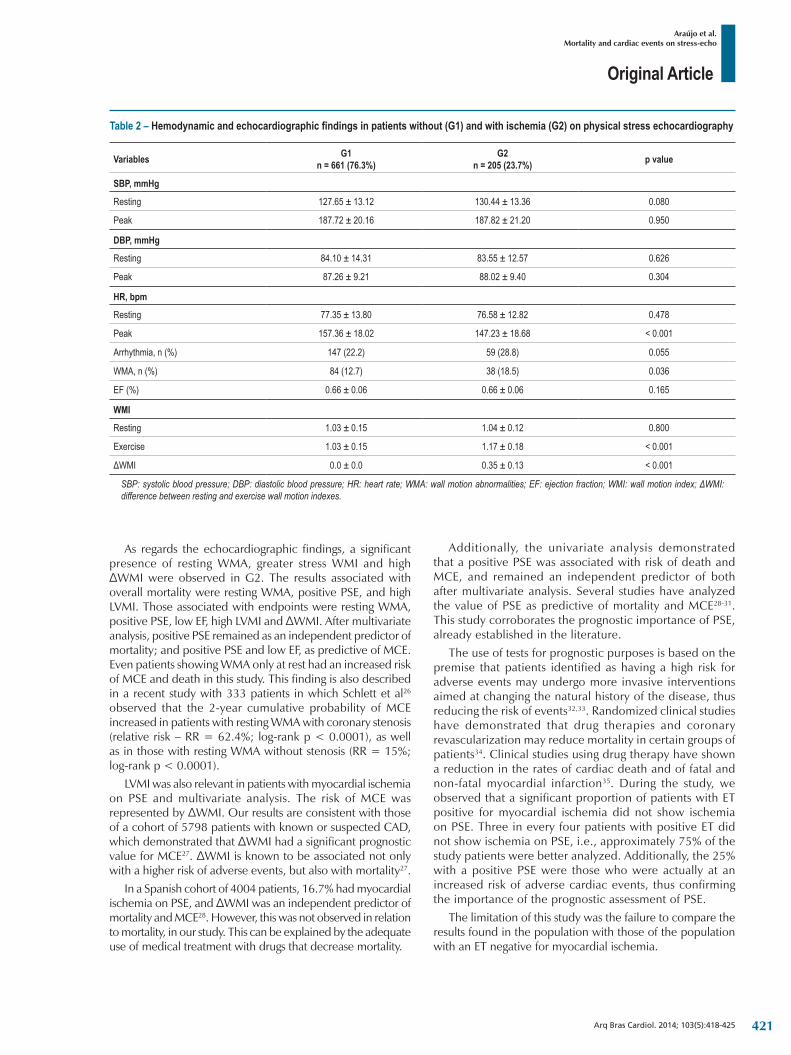
Original Article
Araújo et al.Mortality and cardiac events on stress-echo
Arq Bras Cardiol. 2014; 103(5):418-425
Table 2 – Hemodynamic and echocardiographic findings in patients without (G1) and with ischemia (G2) on physical stress echocardiography
Variables G1n = 661 (76.3%)
G2n = 205 (23.7%) p value
SBP, mmHg
Resting 127.65 ± 13.12 130.44 ± 13.36 0.080
Peak 187.72 ± 20.16 187.82 ± 21.20 0.950
DBP, mmHg
Resting 84.10 ± 14.31 83.55 ± 12.57 0.626
Peak 87.26 ± 9.21 88.02 ± 9.40 0.304
HR, bpm
Resting 77.35 ± 13.80 76.58 ± 12.82 0.478
Peak 157.36 ± 18.02 147.23 ± 18.68 < 0.001
Arrhythmia, n (%) 147 (22.2) 59 (28.8) 0.055
WMA, n (%) 84 (12.7) 38 (18.5) 0.036
EF (%) 0.66 ± 0.06 0.66 ± 0.06 0.165
WMI
Resting 1.03 ± 0.15 1.04 ± 0.12 0.800
Exercise 1.03 ± 0.15 1.17 ± 0.18 < 0.001
ΔWMI 0.0 ± 0.0 0.35 ± 0.13 < 0.001
SBP: systolic blood pressure; DBP: diastolic blood pressure; HR: heart rate; WMA: wall motion abnormalities; EF: ejection fraction; WMI: wall motion index; ΔWMI: difference between resting and exercise wall motion indexes.
As regards the echocardiographic findings, a significant presence of resting WMA, greater stress WMI and high ΔWMI were observed in G2. The results associated with overall mortality were resting WMA, positive PSE, and high LVMI. Those associated with endpoints were resting WMA, positive PSE, low EF, high LVMI and ΔWMI. After multivariate analysis, positive PSE remained as an independent predictor of mortality; and positive PSE and low EF, as predictive of MCE. Even patients showing WMA only at rest had an increased risk of MCE and death in this study. This finding is also described in a recent study with 333 patients in which Schlett et al26 observed that the 2-year cumulative probability of MCE increased in patients with resting WMA with coronary stenosis (relative risk – RR = 62.4%; log-rank p < 0.0001), as well as in those with resting WMA without stenosis (RR = 15%; log-rank p < 0.0001).
LVMI was also relevant in patients with myocardial ischemia on PSE and multivariate analysis. The risk of MCE was represented by ΔWMI. Our results are consistent with those of a cohort of 5798 patients with known or suspected CAD, which demonstrated that ΔWMI had a significant prognostic value for MCE27. ΔWMI is known to be associated not only with a higher risk of adverse events, but also with mortality27.
In a Spanish cohort of 4004 patients, 16.7% had myocardial ischemia on PSE, and ΔWMI was an independent predictor of mortality and MCE28. However, this was not observed in relation to mortality, in our study. This can be explained by the adequate use of medical treatment with drugs that decrease mortality.
Additionally, the univariate analysis demonstrated that a positive PSE was associated with risk of death and MCE, and remained an independent predictor of both after multivariate analysis. Several studies have analyzed the value of PSE as predictive of mortality and MCE28-31. This study corroborates the prognostic importance of PSE, already established in the literature.
The use of tests for prognostic purposes is based on the premise that patients identified as having a high risk for adverse events may undergo more invasive interventions aimed at changing the natural history of the disease, thus reducing the risk of events32,33. Randomized clinical studies have demonstrated that drug therapies and coronary revascularization may reduce mortality in certain groups of patients34. Clinical studies using drug therapy have shown a reduction in the rates of cardiac death and of fatal and non-fatal myocardial infarction35. During the study, we observed that a significant proportion of patients with ET positive for myocardial ischemia did not show ischemia on PSE. Three in every four patients with positive ET did not show ischemia on PSE, i.e., approximately 75% of the study patients were better analyzed. Additionally, the 25% with a positive PSE were those who were actually at an increased risk of adverse cardiac events, thus confirming the importance of the prognostic assessment of PSE.
The limitation of this study was the failure to compare the results found in the population with those of the population with an ET negative for myocardial ischemia.
421
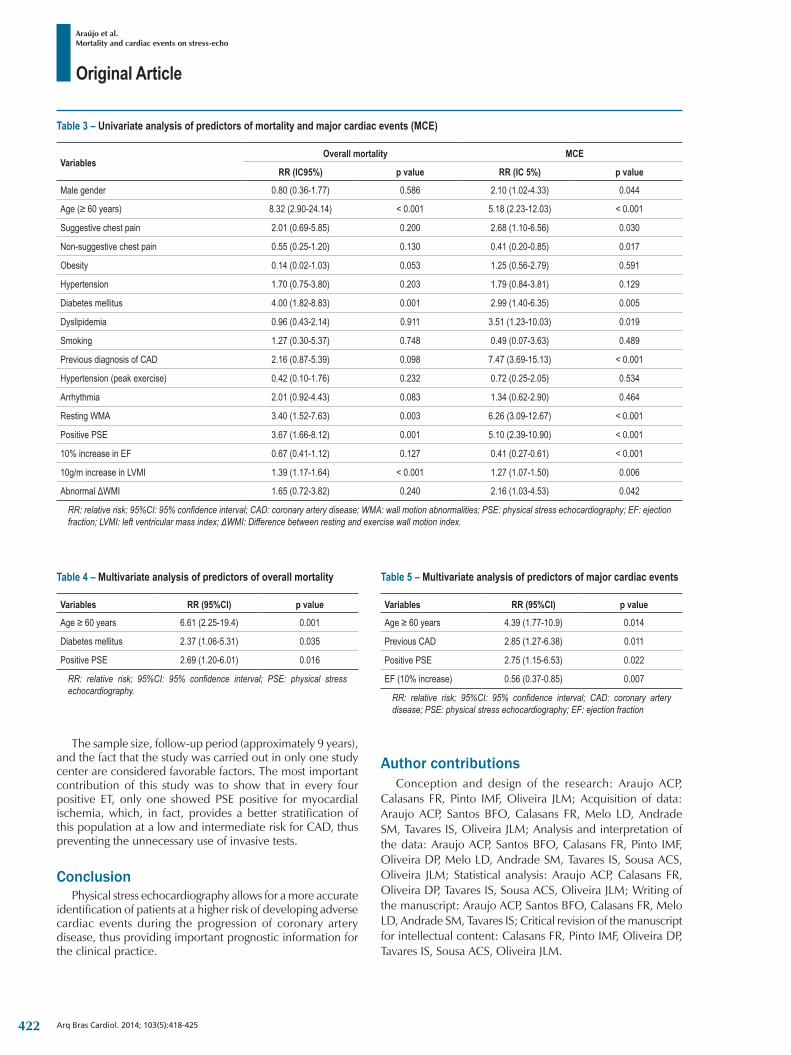
Original Article
Araújo et al.Mortality and cardiac events on stress-echo
Arq Bras Cardiol. 2014; 103(5):418-425
Table 3 – Univariate analysis of predictors of mortality and major cardiac events (MCE)
VariablesOverall mortality MCE
RR (IC95%) p value RR (IC 5%) p value
Male gender 0.80 (0.36-1.77) 0.586 2.10 (1.02-4.33) 0.044
Age (≥ 60 years) 8.32 (2.90-24.14) < 0.001 5.18 (2.23-12.03) < 0.001
Suggestive chest pain 2.01 (0.69-5.85) 0.200 2.68 (1.10-6.56) 0.030
Non-suggestive chest pain 0.55 (0.25-1.20) 0.130 0.41 (0.20-0.85) 0.017
Obesity 0.14 (0.02-1.03) 0.053 1.25 (0.56-2.79) 0.591
Hypertension 1.70 (0.75-3.80) 0.203 1.79 (0.84-3.81) 0.129
Diabetes mellitus 4.00 (1.82-8.83) 0.001 2.99 (1.40-6.35) 0.005
Dyslipidemia 0.96 (0.43-2.14) 0.911 3.51 (1.23-10.03) 0.019
Smoking 1.27 (0.30-5.37) 0.748 0.49 (0.07-3.63) 0.489
Previous diagnosis of CAD 2.16 (0.87-5.39) 0.098 7.47 (3.69-15.13) < 0.001
Hypertension (peak exercise) 0.42 (0.10-1.76) 0.232 0.72 (0.25-2.05) 0.534
Arrhythmia 2.01 (0.92-4.43) 0.083 1.34 (0.62-2.90) 0.464
Resting WMA 3.40 (1.52-7.63) 0.003 6.26 (3.09-12.67) < 0.001
Positive PSE 3.67 (1.66-8.12) 0.001 5.10 (2.39-10.90) < 0.001
10% increase in EF 0.67 (0.41-1.12) 0.127 0.41 (0.27-0.61) < 0.001
10g/m increase in LVMI 1.39 (1.17-1.64) < 0.001 1.27 (1.07-1.50) 0.006
Abnormal ΔWMI 1.65 (0.72-3.82) 0.240 2.16 (1.03-4.53) 0.042
RR: relative risk; 95%CI: 95% confidence interval; CAD: coronary artery disease; WMA: wall motion abnormalities; PSE: physical stress echocardiography; EF: ejection fraction; LVMI: left ventricular mass index; ΔWMI: Difference between resting and exercise wall motion index.
Table 4 – Multivariate analysis of predictors of overall mortality
Variables RR (95%CI) p value
Age ≥ 60 years 6.61 (2.25-19.4) 0.001
Diabetes mellitus 2.37 (1.06-5.31) 0.035
Positive PSE 2.69 (1.20-6.01) 0.016
RR: relative risk; 95%CI: 95% confidence interval; PSE: physical stress echocardiography.
Table 5 – Multivariate analysis of predictors of major cardiac events
Variables RR (95%CI) p value
Age ≥ 60 years 4.39 (1.77-10.9) 0.014
Previous CAD 2.85 (1.27-6.38) 0.011
Positive PSE 2.75 (1.15-6.53) 0.022
EF (10% increase) 0.56 (0.37-0.85) 0.007
RR: relative risk; 95%CI: 95% confidence interval; CAD: coronary artery disease; PSE: physical stress echocardiography; EF: ejection fraction
The sample size, follow-up period (approximately 9 years), and the fact that the study was carried out in only one study center are considered favorable factors. The most important contribution of this study was to show that in every four positive ET, only one showed PSE positive for myocardial ischemia, which, in fact, provides a better stratification of this population at a low and intermediate risk for CAD, thus preventing the unnecessary use of invasive tests.
ConclusionPhysical stress echocardiography allows for a more accurate
identification of patients at a higher risk of developing adverse cardiac events during the progression of coronary artery disease, thus providing important prognostic information for the clinical practice.
Author contributionsConception and design of the research: Araujo ACP,
Calasans FR, Pinto IMF, Oliveira JLM; Acquisition of data: Araujo ACP, Santos BFO, Calasans FR, Melo LD, Andrade SM, Tavares IS, Oliveira JLM; Analysis and interpretation of the data: Araujo ACP, Santos BFO, Calasans FR, Pinto IMF, Oliveira DP, Melo LD, Andrade SM, Tavares IS, Sousa ACS, Oliveira JLM; Statistical analysis: Araujo ACP, Calasans FR, Oliveira DP, Tavares IS, Sousa ACS, Oliveira JLM; Writing of the manuscript: Araujo ACP, Santos BFO, Calasans FR, Melo LD, Andrade SM, Tavares IS; Critical revision of the manuscript for intellectual content: Calasans FR, Pinto IMF, Oliveira DP, Tavares IS, Sousa ACS, Oliveira JLM.
422

Original Article
Araújo et al.Mortality and cardiac events on stress-echo
Arq Bras Cardiol. 2014; 103(5):418-425
Figure 1 – Relative risk for major cardiac events of 5.0 (95% confidence interval: 2.37-10.78).
120
p < 0.0010.12
0.10
0.08
0.06
0.04
0.02
0.00
0 20 40 60 80 100 120
Follow-up period in months
Majo
r car
diac
even
ts
Figure 2 – All-cause death. Relative risk of death of 3.6 (95% confidence interval: 1.65 – 8.06).
120
0.10
0 20 40 60 80 100 120
0.08
0.06
0.04
0.02
0.00
Over
all m
orta
lity
p = 0.001
Follow-up period in months
423

Original Article
Araújo et al.Mortality and cardiac events on stress-echo
Arq Bras Cardiol. 2014; 103(5):418-425
1. Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics - 2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119(3):480-6. Circulation. 2009;119(3):e182.
2. Ministério da Saúde. Datasus : informações sobre mortalidade e informações demográficas. [citado 2005 ago 10]. Disponível em: http://tabnet.datasus.gov.br/cgi/tabcgi.
3. Jahnke C, Nagel E, Gebker R, Kokocinski T, Kelle S, Manka R, et al. Prognostic value of cardiac magnetic resonance stress tests: adenosine stress perfusion and dobutamine stress wall motion imaging. Circulation. 2007;115(13): 1769-76.
4. Scanlon PJ, Faxon DP, Audet AM, Carabello B, Dehmer GJ, Eagle KA, et al. ACC/AHA guidelines for coronary angiography. A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Coronary Angiography). Developed in collaboration with the Society for Cardiac Angiography and Interventions. J Am Coll Cardiol. 1999;33(6):1756-824.
5. Heyndrickx GR, Baig H, Nellens P, Leusen I, Fishbein MC, Vatner SF. Depression of regional blood flow and wall thickening after brief coronary occlusions. Am J Physiol. 1978;234(6):H653-9.
6. Geft MC, Fishbein K, Ninomiya J, Hashida E, Chaux J, Yano J, et al. Intermittent brief periods of ischemia have a cumulative effect and may cause myocardial necrosis. Circulation. 1982;66(6):1150-3.
7. Gottlieb SO, Weisfeldt ML, Ouyang P, Mellits ED, Gerstenblith G. Silent ischemia as a marker for early unfavorable outcomes in patients with unstable angina. N Engl J Med. 1986;314(19):1214-9.
8. Roger VL, Jacobsen SJ, Pellikka PA, Miller TD, Bailey KR, Gersh BJ. Prognostic value of treadmill exercise testing: a population-based study in Olmsted County, Minnesota. Circulation. 1998;98(25):2836-41.
9. Goraya TY, Jacobsen SJ, Pellikka PA, Miller TD, Khan A, Weston SA, et al. Prognostic value of treadmill exercise testing in elderly persons. Ann Intern Med. 2000;132(11):862-70.
10. Gibbons RJ, Balady GJ, Bricker JT, Chaitman BR, Fletcher GF, Froelicher VF, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Committee to Update the 1997 Exercise Testing Guidelines. ACC/AHA 2002 guideline update for exercise testing: summary article. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). J Am Coll Cardiol. 2002;40(8):1531-40. Erratum in J Am Coll Cardiol. 2006;48(8):1731.
11. DePuey EG, Guertler-Krawczynska E, Perkins JV, Robbins WL, Whelchel JD, Clements SD. Alterations in myocardial thallium-201 distribution in patients with chronic systemic hypertension undergoing single photon emission computed tomography”. Am J Cardiol. 1988;62(4):234-8.
12. Kowatsch I. Acurácia diagnóstica da ecocardiografia sob estresse associada ao estudo da perfusao miocárdica com contraste na avaliaçao da isquemia miocárdica: estudo comparativo entre adenosina e dobutamina. [Tese]. Sao Paulo (SP): Faculdade de Medicina . Universidade de Sao Paulo ; 2005.
13. Cheitlin MD, Armstrong WF, Aurigemma GP, Beller GA, Bierman FZ, Davis JL, et al. ACC/AHA/ASE 2003 Guideline Update for the Clinical Application of Echocardiography: summary article. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASE Committee to Update the 1997 Guidelines for the Clinical Application of Echocardiography). J Am Soc Echocardiogr. 2003;16(10):1091-110.
14. Picano E; American College of Cadiology; American Heart Association. Stress echocardiography for the diagnosis of coronary artery disease. Indian Heart J. 2003;55(3):223-7.
15. Barbosa MM, Nunes MCP, Campos Filho O, Camarozano A, Rabischoffsky A, Maciel BC, et al. Sociedade Brasileira de Cardiologia. Diretrizes das indicações da ecocardiografia. Arq Bras Cardiol. 2009;93(6 supl.3):e265-e302.
16. Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R, Feigenbaum H, et al. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J Am Soc Echocardiogr. 1989;2(5):358-67.
17. Picard MH, Adams D, Bierig SM, Dent JM, Douglas PS, Gillam LD, et al; American Society of Echocardiography. American Society of Echocardiography Recommendations for quality echocardiography laboratory operations. J Am Soc Echocardiogr. 2011;24(1):1-10.
18. Sartorelli DS, Franco LJ. Tendências do diabetes mellitus no Brasil: o papel da transiçao nutricional. Cad Saúde Pública. 2003;19(1):S29-36.
19. Mota E, Moriguchi E. Dislipidemia em idosos: devemos tratar? Dislipidemia Today. 2001;1:3-10.
20. Wilhelmesen L, Rosengren A, Eriksson H, Lappas G. Heart failure in the general population of men: morbidity, risk factors and prognosis. J Intern Med. 2001;249(3):253-61.
21. Zanchetti A. The hipertensive patients with multiple risk factors. Is treatment really so difficult? Am J Hypertens. 1997;10(10 Pt 2):223S-9S.
22. Phillips AN, Shaper AG, Pocock SJ, Walker M, Macfarlane PW. The role of risk factors in heart attacks occurring in men with pre-existing ischaemic heart disease. Br Heart J. 1988;60(5):404-10.
23. Brewer HB Jr. Hypertriglyceridemia: changes in the plasma lipoproteins associated with an increased risk of cardiovascular disease. Am J Cardiol. 1999;83(9B):3F-12F.
24. Anderson JL, Muhlestein JB, Horne BD, Carlquist JF, Bair TL, Madsen TE, et al. Plasma homocysteine predicts mortality independently of traditional risk factors and C-reactive protein in patients with angiographically defined coronary artery disease. Circulation. 2000;102(11):1227-32.
25. Lewis WR. Echocardiography in the evaluation of patients in chest pain units. Cardiol Clin. 2005;23(4):531-9.
26. Schlett CL, Banerji D, Siegel E, Bamberg F, Lehman SJ, Ferencik M, et al. Prognostic value of CT angiography for major adverse cardiac events in patients with acute chest pain from the emergency department: 2-year outcomes of the ROMICAT trial. JACC Cardiovasc Imaging. 2011;4(5):481-91.
References
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This study is not associated with any thesis or dissertation work.
424

Original Article
Araújo et al.Mortality and cardiac events on stress-echo
Arq Bras Cardiol. 2014; 103(5):418-425
27. Arruda-Olson AM, Juracan EM, Mahoney DW, McCully RB, Roger VL, Pellikka PA. Prognostic value of exercise echocardiography in 5,798 patients: is there a gender difference? J Am Coll Cardiol. 2002;39(4):625-31.
28. Elhendy A, Mahoney DW, Burger KN, McCully RB, Pellikka PA. Prognostic value of exercise echocardiography in patients with classic angina pectoris. Am J Cardiol. 2004;94(5):559-63.
29. Arruda AM, Das MK, Roger VL, Klarich KW, Mahoney DW, Pellikka PA. Prognostic value of exercise echocardiography in 2,632 patients > or = 65 years of age. J Am Coll Cardiol. 2001;37(4):1036-41.
30. Oliveira JL, Barreto-Filho JA, Oliveira CR, Santana TA, Anjos-Andrade FD, Alves EO, et al. Prognostic value of exercise echocardiography in diabetic patients. Cardiovasc Ultrasound. 2009;7:24.
31. Yao S, Bangalore S, Ahuja A, Chaudhry FA. Stress echocardiography: risk stratification, prognosis, patient outcomes and cost-effectiveness. Minerva Cardioangiol. 2009;57(3):315-31.
32. Bouzas-Mosquera A, Peteiro J, Alvarez-Garcia N, Broullon FJ, Mosquera VX, Garcia-Bueno L, et al. Prediction of mortality and major cardiac events by exercise echocardiography in patients with normal exercise electrocardiographic testing. J Am Coll Cardiol. 2009;53(21):1981-90.
33. Elhendy A, Mahoney DW, Khandheria BK, Paterick TE, Burger KN, Pellikka PA. Prognostic significance of the location of wall motion abnormalities during exercise echocardiography. J Am Coll Cardiol. 2002;40(9):1623-9.
34. Alderman EL, Bourassa MG, Cohen LS, Davis KB, Kaiser GG, Killip T, et al. Ten-year follow-up of survival and myocardial infarction in the randomized Coronary Artery Surgery Study. Circulation. 1990;82(5):1629-46.
35. Jong P, Yusuf S, Rousseau MF, Ahn SA, Bangdiwala SI. Effect of enalapril on 12-year survival and life expectancy in patients with left ventricular systolic dysfunction: a follow-up study. Lancet. 2003;361(9372):1843-8.
425

Original Article
Determinants of Functional and Structural Properties of Large Arteries in Healthy IndividualsElaine Cristina Tolezani, Valéria Costa-Hong, Gustavo Correia, Alfredo José Mansur, Luciano Ferreira Drager, Luiz Aparecido BortolottoInstituto do Coração, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo, SP – Brazil
Mailing Address: Valéria Costa-Hong •Avenida Dr. Eneias de Carvalho Aguiar, Cerqueira Cesar. Postal Code 05403-000, São Paulo, SP − BrazilE-mail: [email protected] received October 23, 2013; revised manuscript February 26, 2014; accepted May 05, 2014.
DOI: 10.5935/abc.20140124
Abstract
Background: Changes in the properties of large arteries correlate with higher cardiovascular risk. Recent guidelines have included the assessment of those properties to detect subclinical disease. Establishing reference values for the assessment methods as well as determinants of the arterial parameters and their correlations in healthy individuals is important to stratify patients.
Objective: To assess, in healthy adults, the distribution of the values of pulse wave velocity, diameter, intima-media thickness and relative distensibility of the carotid artery, in addition to assessing the demographic and clinical determinants of those parameters and their correlations.
Methods: This study evaluated 210 individuals (54% women; mean age, 44 ± 13 years) with no evidence of cardiovascular disease. The carotid-femoral pulse wave velocity was measured with a Complior® device. The functional and structural properties of the carotid artery were assessed by using radiofrequency ultrasound.
Results: The means of the following parameters were: pulse wave velocity, 8.7 ± 1.5 m/s; diameter, 6,707.9 ± 861.6 µm; intima-media thickness, 601 ± 131 µm; relative distensibility, 5.3 ± 2.1%. No significant difference related to sex or ethnicity was observed. On multiple linear logistic regression, the factors independently related to the vascular parameters were: pulse wave velocity, to age (p < 0.01) and triglycerides (p = 0.02); intima-media thickness, to age (p < 0.01); diameter, to creatinine (p = 0.03) and age (p = 0.02); relative distensibility, to age (p < 0.01) and systolic and diastolic blood pressures (p = 0.02 and p = 0.01, respectively). Pulse wave velocity showed a positive correlation with intima-media thickness (p < 0.01) and with relative distensibility (p < 0.01), while diameter showed a positive correlation with distensibility (p = 0.03).
Conclusion: In healthy individuals, age was the major factor related to aortic stiffness, while age and diastolic blood pressure related to the carotid functional measure. The carotid artery structure was directly related to aortic stiffness, which was inversely related to the carotid artery functional property. (Arq Bras Cardiol. 2014; 103(5):426-432)
Keywords: Arteries; Arterial Pressure; Vascular Stiffness; Pulse Wave Analysis; Carotid Intima-Media Thickness.
IntroductionThe importance of arterial stiffness to the development
of cardiovascular diseases has been emphasized in past years. Changes in the functional and structural properties of large arteries have been correlated with greater cardiovascular risk in different populations1-4, and, although considered to be intrinsic to the vascular aging process3,5,6, they are influenced by other diseases and risk factors7,8, such as sex, dyslipidemia, diabetes, increased heart rate (HR), smoking9, arterial hypertension, chronic renal disease and obesity10-12.
New and accessible methods enable the non-invasive assessment of functional and structural properties of large arteries. The European guidelines of arterial hypertension13 and the VI Brazilian Guidelines on Hypertension14 include measurements of aortic stiffness and carotid artery intima-media thickness (IMT) as methods to assess the possible subclinical cardiovascular disease of hypertensive patients.
Aortic stiffness and carotid artery IMT are important parameters for cardiovascular risk assessment, being currently used for the detection of subclinical disease, minimizing poorer prognoses. To assess arterial stiffness, pulse wave velocity (PWV) measurement is gold-standard, because of the method reproducibility and reliability, in addition to its association with cardiovascular risk in different populations, independently of the risk factors related15,16.
To establish a reference pattern for the functional and structural assessment methods of arterial properties is required so that the measurement of arterial stiffness and other arterial properties can express the presence of subclinical cardiovascular disease. In addition, the major
426

Original Article
Tolezani et al.Arterial properties in healthy individuals
Arq Bras Cardiol. 2014; 103(5):426-432
Table 1 – Research projects used as data bank
Approval protocol number Project’s name
2431/04/51 Impact of Obstructive Sleep Apnea Syndrome on the Structural and Functional Properties of Large Arteries
721/04 Influence of the polymorphism of alpha2-1, alpha2-c and beta1 adrenergic receptor genes on the cardiovascular regulation of children of hypertensives
2403/04/23 Determinants of arterial stiffness and carotid intima-media thickness in familial hypercholesterolemia
852/03 Chest-BR
clinical and demographic determinants of the parameters obtained with those methods and their correlations need to be established.
In Brazil, a reference pattern for those methods and for assessing the major determinants of the function and structure of large arteries is yet to be studied, that being the purpose of this study.
This study aimed at assessing the following in healthy adults: (1) the distribution of aortic PWV values, as well as the diameter, IMT and relative distensibility of the carotid artery, to define the reference values for the methods applied; (2) the major demographic and clinical determinants of the parameters obtained by using those methods; and (3) the correlations between the arterial parameters obtained by using the different methods.
MethodsThis study included 210 asymptomatic adults of both
sexes (age range, 18 to 80 years), with no evidence of current cardiovascular disease after clinical and laboratory assessment, and not using any medication. They had participated as control groups in research projects duly approved by the Ethics Committee of the Sao Paulo University Medical School (Table 1).
For sample calculation, a minimum number of 30 patients per age group was considered, based on the power to detect changes in PWV measurements, according to the reproducibility and sensitivity of the test observed at our service. The method had intraobserver and interobserver reproducibility coefficients of 0.935 and 0.890, respectively. That minimum number per age group was calculated by using the JMP statistical software. Thus, subdividing the population into seven age groups, from 18 to 80 years, 210 individuals were obtained. However, because of the difficulty of getting individuals older than 70 years with no comorbidity, the same number of individuals initially calculated was maintained, distributed according to a population curve, predominating ages between 41 and 50 years.
Written informed consents were provided in the respective projects. The Chest-BR project, assessing individuals with no clinical cardiovascular disease, involved 143 patients. All underwent complete clinical assessment, laboratory tests, cardiopulmonary exercise test, and echocardiography, and no change in any of those assessments was evidenced.
The clinical assessment included careful anamnesis for data collection, such as age, sex, race and presence or lack of exclusion criteria. Ethnicity was recorded according
to the individuals’ self-reports and classified as white, black, mixed and yellow. To make the result presentation clearer, the population studied was divided into white and non-white. A Filizola scale, Personal model, was used to measure the weight and height of barefoot individuals wearing light clothes. The body mass index (BMI) was determined with the following formula: body weight (kg)/height² (m²). Brachial systolic and diastolic blood pressures (SBP and DBP, respectively), as well as HR, were measured by using the automated Omron HEM 705-CP device, duly validated, according to the international protocol of the British Hypertension Society (BHS)17 and the Association for Advancement of Medical Instrumentation (AAMI)18. The device was used on the right arm, with the individual sitting and after a 5-minute rest, according to the recommendations of the VI Brazilian Guidelines on Hypertension14. Pulse pressure (PP) was determined by using the formula: SBP – DBP.
Laboratory tests were performed at the laboratory of the institution after a 12-hour fasting period.
Individuals with any of the following clinical conditions were excluded from the study: chronic renal failure (creatinine > 1.4 mg/dL); hepatic failure; systemic arterial hypertension [blood pressure (BP) > 140/90 mmHg or patient on anti-hypertensive medication]; inflammatory diseases; neoplasias; endocrine disorders; hematologic diseases; peripheral vascular diseases; hypercholesterolemia (total cholesterol > 240 mg/dL or patient on lipid-lowering medication); cardiomyopathies; valvular heart diseases; congenital diseases; and obesity (BMI > 30).
Methods to assess the arterial parametersThe PWV is automatically measured by recording
simultaneous pulse waves captured by external sensors on two known points of the arterial tree (carotid and femoral arteries), being calculated as the propagation distance between those two points divided by the time necessary to travel between them, provided by the software of the device. That measurement was obtained with the Complior® device (Gonesse, France), already validated and used in several studies at our laboratory19-22. The PWV was assessed on the carotid-femoral arterial segment, and represented the measure of the pulse wave propagation along the aorta. To obtain PWV of each patient, ten good-quality curves were selected, and the mean calculated. The curves were acquired with the individuals placed in the dorsal decubitus position.
427

Original Article
Tolezani et al.Arterial properties in healthy individuals
Arq Bras Cardiol. 2014; 103(5):426-432
Table 2 – Clinical, laboratory and demographic characteristics of the participants, n = 210
Variables Sample (210)
Age, years 44 ± 13
Female sex, n (%) 109 (54)
White, n (%) 141 (76)
Body mass index, kg/m² 25 ± 3
Systolic blood pressure, mmHg 118 ± 13
Diastolic blood pressure, mmHg 75 ± 10
Creatinine, mg/dL 0.9 ± 0.2
Total cholesterol, mg/dL 191 ± 32
Triglycerides, mg/dL 100 ± 32
LDL-cholesterol, mg/dL 120 ± 28
HDL-cholesterol, mg/dL 39 ± 6
Hematocrit, % 42 ± 3
Glycemia, mg/dL 92 ± 7
The functional and anatomical properties of the right carotid artery were assessed by using an ultrasound device consisting of a vessel wall echo-tracking system (Wall-Track System, Pie Medical, Maastricht, The Netherlands), that analyses the radiofrequency signals, and was developed to measure wall movements of superficial large arteries based on location by use of B-mode conventional vascular ultrasound. The method has been validated and used in clinical studies23-26. The accuracy of that system is 30 μm for measuring the diastolic diameter and lower than 1 μm for the pulsatile diameter variation (difference between the systolic and diastolic diameters). The right common carotid artery was assessed 2 cm bellow the carotid bifurcation, and the following measurements were taken: carotid artery IMT and diameter; beat-to-beat carotid systolic-diastolic variation; and percentage of that systolic-diastolic variation7,23.
Statistical analysisThe Kolmogorov-Smirnov test was used to assess the
distribution of continuous variables. The variables were expressed as mean ± standard deviation (SD), median [25 – 75 percentiles] or percentage, as appropriate.
The correlation coefficient (r) between clinical, anthropometric, biochemical data, PWV and carotid parameters was obtained by use of the Pearson method for normally distributed variables, and the Spearman method for nonparametric distributed variables.
Analysis of variance (ANOVA) was used to compare between variables of different groups, the differences being confirmed by using the Tukey-Kramer test.
Factors independently associated with functional and structural vascular changes were assessed by using different linear regression models (uni- and multivariate), considering the PWV and carotid arterial parameters (diameter, distensibility or IMT) as dependent variables. For multivariate analysis, the following variables were considered independent: age, sex, ethnicity, smoking, weight, height, BMI, SBP, DBP, PP, glycemia, total cholesterol, LDL-cholesterol, HDL-cholesterol, triglycerides and C-reactive protein. For each model, the estimated parameters, SD, descriptive significance level (p) and correlation coefficient (r) were presented.
The JMP statistical software, version 5.0, was used and p values < 0.05 were considered statistically significant.
ResultsTable 2 shows the major clinical, laboratory and
demographic characteristics of the participants.
Measurements of arterial propertiesThe following means were obtained: PWV, 8.7 ± 1.5 m/s;
carotid artery diameter, 6,707.9 ± 861.6 μm; carotid IMT, 601±131 μm; and relative distensibility of the carotid artery, 5.3 ± 2.1%.
Correlation with demographic parametersNo significant difference in the vascular parameters was
observed regarding sex and ethnicity.
Correlation with ageAge had a significant and positive correlation with
PWV (r = 0.50; p ≤ 0.01), diameter (r = 0.18; p ≤ 0.01) and carotid artery IMT (r = 0.28; p ≤ 0.01), and negative correlation with relative distensibility of the carotid artery (r = -0.33; p ≤ 0.01).
Table 3 shows the distribution of PWV values, carotid artery diameter, IMT and relative distensibility according to different age group. A progressive increase in PWV, carotid artery diameter and IMT, in addition to a decrease in the relative distensibility of the carotid artery according to category were observed.
Correlation with anthropometric variablesThe relative distensibility of the carotid artery had a significant
and negative correlation with BMI (r = -0.21; p = 0.03), while the carotid artery diameter had a significant and positive correlation with BMI (r = 0.22; p = 0.002). The PWV showed no correlation with the anthropometric parameters in that population.
Correlation with blood pressure and heart rateThe PWV had a significant and positive correlation with
SBP (r = 0.24; p ≤ 0.01), DBP (r = 0.26; p ≤ 0.01) and PP (r = 0.17; p = 0.01), while the carotid artery diameter had a significant and positive correlation with SBP (r = 0.17; p = 0.01) and DBP (r = 0.2; p = 0.004). The relative distensibility of the carotid artery had a significant and inverse correlation with SBP (r = -0.19; p = 0.01), DBP (r = -0.32; p ≤ 0.01) and HR (r = -0.18; p = 0.01). The carotid artery IMT had a significant and positive correlation with SBP (r = 0.15; p = 0.03), PP (r = 0.18; p = 0.01) and HR (r = 0.16; p = 0.03).
The individuals were classified according to the VI Brazilian Guidelines on Hypertension14 aiming at categorizing the values of aortic PWV, carotid artery IMT, diameter,
428
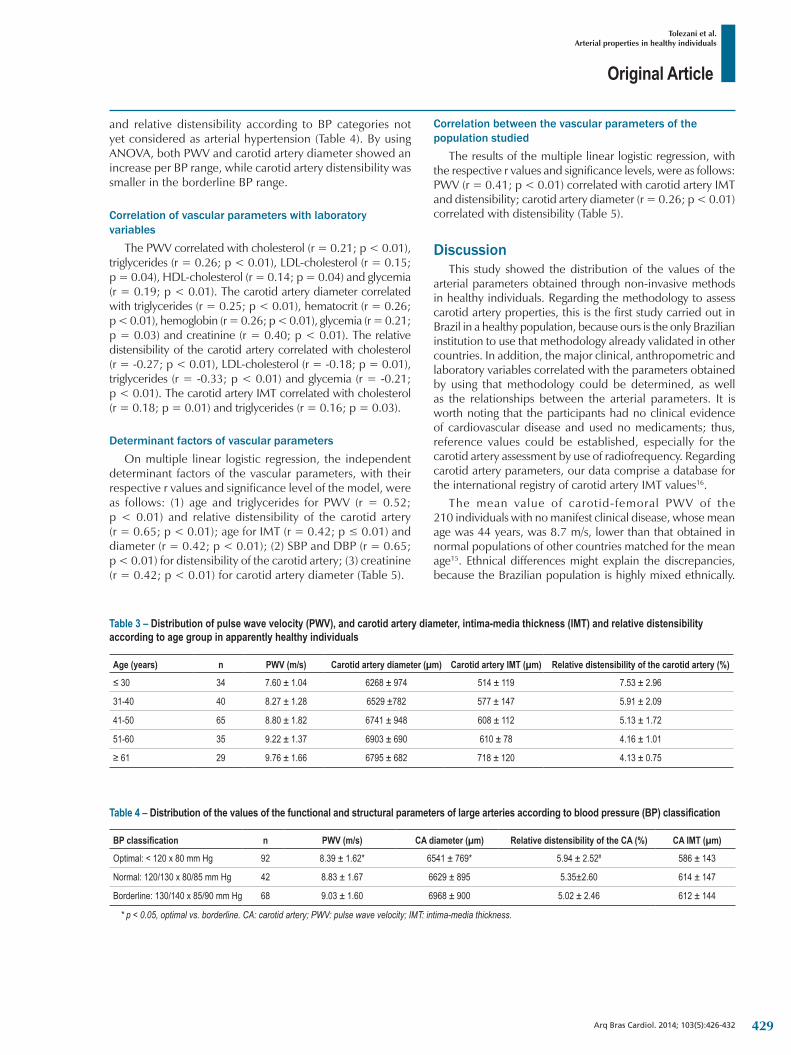
Original Article
Tolezani et al.Arterial properties in healthy individuals
Arq Bras Cardiol. 2014; 103(5):426-432
Table 3 – Distribution of pulse wave velocity (PWV), and carotid artery diameter, intima-media thickness (IMT) and relative distensibility according to age group in apparently healthy individuals
Age (years) n PWV (m/s) Carotid artery diameter (µm) Carotid artery IMT (µm) Relative distensibility of the carotid artery (%)
≤ 30 34 7.60 ± 1.04 6268 ± 974 514 ± 119 7.53 ± 2.96
31-40 40 8.27 ± 1.28 6529 ±782 577 ± 147 5.91 ± 2.09
41-50 65 8.80 ± 1.82 6741 ± 948 608 ± 112 5.13 ± 1.72
51-60 35 9.22 ± 1.37 6903 ± 690 610 ± 78 4.16 ± 1.01
≥ 61 29 9.76 ± 1.66 6795 ± 682 718 ± 120 4.13 ± 0.75
and relative distensibility according to BP categories not yet considered as arterial hypertension (Table 4). By using ANOVA, both PWV and carotid artery diameter showed an increase per BP range, while carotid artery distensibility was smaller in the borderline BP range.
Correlation of vascular parameters with laboratory variables
The PWV correlated with cholesterol (r = 0.21; p < 0.01), triglycerides (r = 0.26; p < 0.01), LDL-cholesterol (r = 0.15; p = 0.04), HDL-cholesterol (r = 0.14; p = 0.04) and glycemia (r = 0.19; p < 0.01). The carotid artery diameter correlated with triglycerides (r = 0.25; p < 0.01), hematocrit (r = 0.26; p < 0.01), hemoglobin (r = 0.26; p < 0.01), glycemia (r = 0.21; p = 0.03) and creatinine (r = 0.40; p < 0.01). The relative distensibility of the carotid artery correlated with cholesterol (r = -0.27; p < 0.01), LDL-cholesterol (r = -0.18; p = 0.01), triglycerides (r = -0.33; p < 0.01) and glycemia (r = -0.21; p < 0.01). The carotid artery IMT correlated with cholesterol (r = 0.18; p = 0.01) and triglycerides (r = 0.16; p = 0.03).
Determinant factors of vascular parametersOn multiple linear logistic regression, the independent
determinant factors of the vascular parameters, with their respective r values and significance level of the model, were as follows: (1) age and triglycerides for PWV (r = 0.52; p < 0.01) and relative distensibility of the carotid artery (r = 0.65; p < 0.01); age for IMT (r = 0.42; p ≤ 0.01) and diameter (r = 0.42; p < 0.01); (2) SBP and DBP (r = 0.65; p < 0.01) for distensibility of the carotid artery; (3) creatinine (r = 0.42; p < 0.01) for carotid artery diameter (Table 5).
Correlation between the vascular parameters of the population studied
The results of the multiple linear logistic regression, with the respective r values and significance levels, were as follows: PWV (r = 0.41; p < 0.01) correlated with carotid artery IMT and distensibility; carotid artery diameter (r = 0.26; p < 0.01) correlated with distensibility (Table 5).
DiscussionThis study showed the distribution of the values of the
arterial parameters obtained through non-invasive methods in healthy individuals. Regarding the methodology to assess carotid artery properties, this is the first study carried out in Brazil in a healthy population, because ours is the only Brazilian institution to use that methodology already validated in other countries. In addition, the major clinical, anthropometric and laboratory variables correlated with the parameters obtained by using that methodology could be determined, as well as the relationships between the arterial parameters. It is worth noting that the participants had no clinical evidence of cardiovascular disease and used no medicaments; thus, reference values could be established, especially for the carotid artery assessment by use of radiofrequency. Regarding carotid artery parameters, our data comprise a database for the international registry of carotid artery IMT values16.
The mean value of carotid-femoral PWV of the 210 individuals with no manifest clinical disease, whose mean age was 44 years, was 8.7 m/s, lower than that obtained in normal populations of other countries matched for the mean age15. Ethnical differences might explain the discrepancies, because the Brazilian population is highly mixed ethnically.
Table 4 – Distribution of the values of the functional and structural parameters of large arteries according to blood pressure (BP) classification
BP classification n PWV (m/s) CA diameter (µm) Relative distensibility of the CA (%) CA IMT (µm)
Optimal: < 120 x 80 mm Hg 92 8.39 ± 1.62* 6541 ± 769* 5.94 ± 2.52# 586 ± 143
Normal: 120/130 x 80/85 mm Hg 42 8.83 ± 1.67 6629 ± 895 5.35±2.60 614 ± 147
Borderline: 130/140 x 85/90 mm Hg 68 9.03 ± 1.60 6968 ± 900 5.02 ± 2.46 612 ± 144
* p < 0.05, optimal vs. borderline. CA: carotid artery; PWV: pulse wave velocity; IMT: intima-media thickness.
429
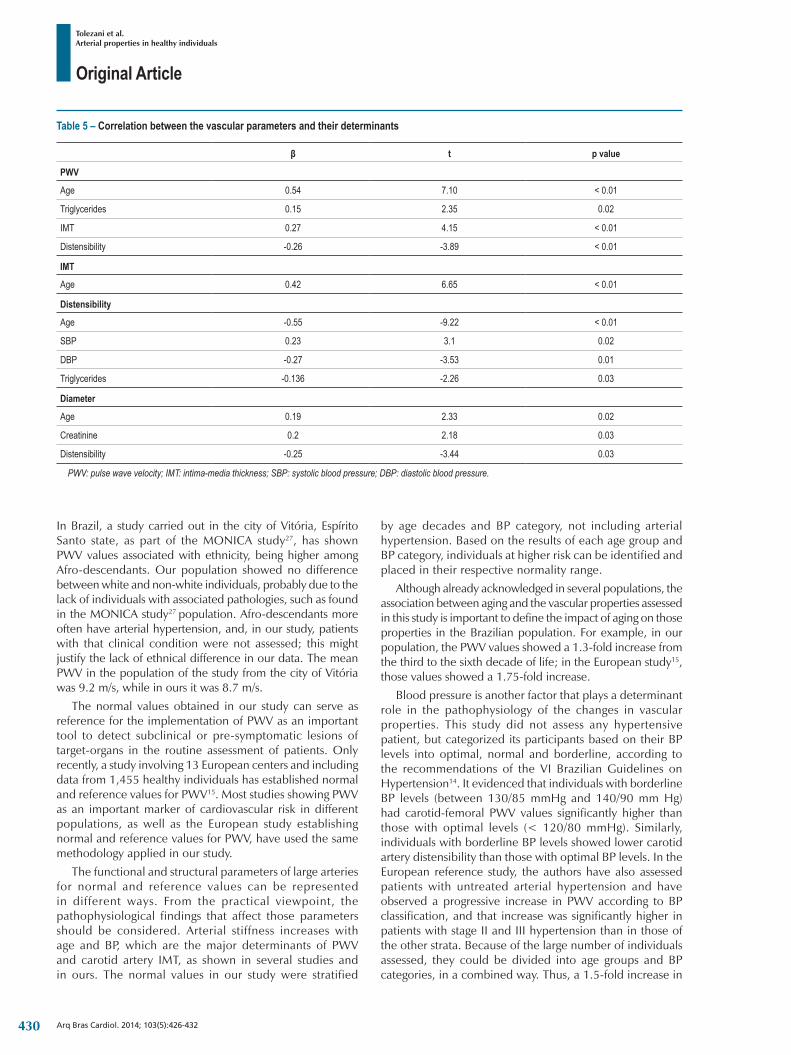
Original Article
Tolezani et al.Arterial properties in healthy individuals
Arq Bras Cardiol. 2014; 103(5):426-432
Table 5 – Correlation between the vascular parameters and their determinants
β t p value
PWV
Age 0.54 7.10 < 0.01
Triglycerides 0.15 2.35 0.02
IMT 0.27 4.15 < 0.01
Distensibility -0.26 -3.89 < 0.01
IMT
Age 0.42 6.65 < 0.01
Distensibility
Age -0.55 -9.22 < 0.01
SBP 0.23 3.1 0.02
DBP -0.27 -3.53 0.01
Triglycerides -0.136 -2.26 0.03
Diameter
Age 0.19 2.33 0.02
Creatinine 0.2 2.18 0.03
Distensibility -0.25 -3.44 0.03
PWV: pulse wave velocity; IMT: intima-media thickness; SBP: systolic blood pressure; DBP: diastolic blood pressure.
In Brazil, a study carried out in the city of Vitória, Espírito Santo state, as part of the MONICA study27, has shown PWV values associated with ethnicity, being higher among Afro-descendants. Our population showed no difference between white and non-white individuals, probably due to the lack of individuals with associated pathologies, such as found in the MONICA study27 population. Afro-descendants more often have arterial hypertension, and, in our study, patients with that clinical condition were not assessed; this might justify the lack of ethnical difference in our data. The mean PWV in the population of the study from the city of Vitória was 9.2 m/s, while in ours it was 8.7 m/s.
The normal values obtained in our study can serve as reference for the implementation of PWV as an important tool to detect subclinical or pre-symptomatic lesions of target-organs in the routine assessment of patients. Only recently, a study involving 13 European centers and including data from 1,455 healthy individuals has established normal and reference values for PWV15. Most studies showing PWV as an important marker of cardiovascular risk in different populations, as well as the European study establishing normal and reference values for PWV, have used the same methodology applied in our study.
The functional and structural parameters of large arteries for normal and reference values can be represented in different ways. From the practical viewpoint, the pathophysiological findings that affect those parameters should be considered. Arterial stiffness increases with age and BP, which are the major determinants of PWV and carotid artery IMT, as shown in several studies and in ours. The normal values in our study were stratified
by age decades and BP category, not including arterial hypertension. Based on the results of each age group and BP category, individuals at higher risk can be identified and placed in their respective normality range.
Although already acknowledged in several populations, the association between aging and the vascular properties assessed in this study is important to define the impact of aging on those properties in the Brazilian population. For example, in our population, the PWV values showed a 1.3-fold increase from the third to the sixth decade of life; in the European study15, those values showed a 1.75-fold increase.
Blood pressure is another factor that plays a determinant role in the pathophysiology of the changes in vascular properties. This study did not assess any hypertensive patient, but categorized its participants based on their BP levels into optimal, normal and borderline, according to the recommendations of the VI Brazilian Guidelines on Hypertension14. It evidenced that individuals with borderline BP levels (between 130/85 mmHg and 140/90 mm Hg) had carotid-femoral PWV values significantly higher than those with optimal levels (< 120/80 mmHg). Similarly, individuals with borderline BP levels showed lower carotid artery distensibility than those with optimal BP levels. In the European reference study, the authors have also assessed patients with untreated arterial hypertension and have observed a progressive increase in PWV according to BP classification, and that increase was significantly higher in patients with stage II and III hypertension than in those of the other strata. Because of the large number of individuals assessed, they could be divided into age groups and BP categories, in a combined way. Thus, a 1.5-fold increase in
430

Original Article
Tolezani et al.Arterial properties in healthy individuals
Arq Bras Cardiol. 2014; 103(5):426-432
PWV could be observed in younger individuals with optimal BP levels and in the hypertensive elderly. Because of the smaller number of individuals in our study, that analysis could not be performed, but the same type of correlation might exist. Although the relationship between BP and PWV has been well known for almost one century, both our results and those of the European study suggest that the increase in PWV with BP is not merely attributable to the BP increase with age, but that the age effect is incremented by higher BP.
The lipid profile, especially triglyceride levels, has been related to both functional and structural parameters of large arteries. The role played by lipids in the properties of large arteries is still controversial. Based on our previous experience with patients with familial hypercholesterolemia, triglyceride levels were important determinants for both PWV and carotid artery distensibility17,28.
Another important and unpublished finding of our study relates to the associations of the parameters obtained with the two methodologies for arterial assessment. The PWV measure was directly related to carotid artery IMT, showing a close correlation between a functional systemic change and a more localized structural change. In addition, an inverse and significant correlation was observed between carotid-femoral PWV and the relative distensibility of the carotid artery. That association of PWV and IMT had already been reported in a study with 564 individuals29, half of whom were hypertensive, but, after correcting for other risk factors, that association disappeared, persisting only that between PWV and the presence of atherosclerotic plaques. In our study, the association remained significant even after correction for the major cardiovascular risk factors, and the presence of plaques was not assessed. In another study including 2,000 Finnish individuals30, using different methodologies to assess PWV and IMT, the former was not significantly correlated with the second in the general population, only in older individuals. However, similarly to our study, PWV was inversely related to carotid artery distensibility, emphasizing the importance of the relationship between aortic stiffness and carotid functional properties. These data are important to show that two methods assessing similar functional properties, but in different ways, show equivalent results in a healthy population.
Study limitationsComparing to other population studies, ours had a smaller
number of individuals, which limited the establishment of criteria of normality. Part of those individuals did not undergo complete clinical and laboratory assessment, being excluded from the analysis. However, because most individuals
underwent complete clinical and laboratory assessment for cardiovascular disease, that became a well-selected population with no evidence of associated disease; thus, the data originated from that population can be used as reference for comparison with populations with different pathologies.
ConclusionIn individuals without clinically manifest cardiovascular
disease, aorta stiffness measured by using PWV increases with age, while the local functional parameters of the carotid artery are independently related to age and DBP. In that same population, the functional and structural vascular parameters are also associated, so that the carotid artery structure assessed by using IMT is directly related to aortic stiffness, while the latter is inversely related to the carotid artery functional property.
Those findings help to understand the factors related to the functional and structural measures of large vessels and how they correlate in the absence of manifest cardiovascular disease. Establishing those relationships is important for the clinical application of the methodology to assess vascular parameters in the presence of clinical diseases, contributing to use the method in our population.
Author contributionsConception and design of the research: Tolezani EC,
Mansur AJ, Bortolotto LA, Drager LF; Acquisition of data: Tolezani EC, Costa-Hong V; Analysis and interpretation of the data and Critical revision of the manuscript for intellectual content: Tolezani EC, Costa-Hong V, Bortolotto LA, Drager LF; Statistical analysis: Tolezani EC, Costa-Hong V, Bortolotto LA; Writing of the manuscript: Tolezani EC, Bortolotto LA; Capture patient: Correia G, Mansur AJ.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis article is part of the thesis of Doctoral submitted by
Elaine Cristina Tolezani, from Faculdade de Medicina da Universidade de Sao Paulo.
1. Laurent S, Boutouyrie P, Asmar R, Gautier I, Laloux B, Guize L, et al. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension. 2001;37(5):1236-41.
2. NajjarSS, Scuteri A, Lakatta EG. Arterial aging: is it an immutable cardiovascular risk factor? Hypertension. 2005;46(3):454-62.
3. Cohn JN. Arterial stiffness, vascular disease, and risk of cardiovascular events. Circulation. 2006;113(5):601-3.
4. Sutton-Tyrrell K, Najjar SS, Boudreau RM, Venkitachalam L, Kupelian V, Simonsick EM, et al. Elevated aortic pulse wave velocity, a marker of arterial stiffness, predicts cardiovascular events in well-functioning older adults. Circulation. 2005;111(25):3384-90.
References
431

Original Article
Tolezani et al.Arterial properties in healthy individuals
Arq Bras Cardiol. 2014; 103(5):426-432
5. Liao D, Arnett DK, Tyroler HA, Riley WA, Chambless LE, Szklo M, et al. Arterial stiffness and the development of hypertension. The ARIC study. Hypertension. 1999;34(2):201-6.
6. Hashimoto J, Chonan K, Aoki Y, Nishimura T, Ohkubo T, Hozawa A, et al. Pulse wave velocity and the second derivative of the finger photoplethysmogram in treated hypertensive patients: their relationship and associating factors. J Hypertens. 2002;20(12):2415-22.
7. Safar ME, Levy BI, Struijker-Boudier H. Current perspectives on arterial stiffness and pulse pressure in hypertension and cardiovascular diseases. Circulation. 2003;107(22):2864-9.
8. Paini A, Boutouyrie P, Calvet D, Tropeano AI, Laloux B, Laurent S. Carotid and aortic stiffness: determinants of discrepancies. Hypertension. 2006;47(3):371-6.
9. Benetos A, Adamopoulos C, Bureau JM, Temmar M, Labat C, Bean K, et al. Determinants of accelerated progression of arterial stiffness in normotensive subjects and in treated hypertensive subjects over a 6-year period. Circulation. 2002;105(10):1202-7.
10. Weber T, Auer J, O’Rourke MF, Kvas E, Lassnig E, Berent R, et al. Arterial stiffness, wave reflections, and the risk of coronary artery disease. Circulation. 2004;109(2):184-9.
11. Bortolotto LA, Blacher J, Kondo T, Takazawa K, Safar ME. Assessment of vascular aging and atherosclerosis in hypertensive subjects: second derivative of photoplethysmogram versus pulse wave velocity. Am J Hypertens. 2000;13(2):165-71.
12. Bulpitt CJ, Rajkumar C, Cameron JD. Vascular compliance as a measure of biological age. J Am Geriatr Soc. 1999;47(6):657-63.
13. 2003 European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension. Guidelines Committee. J Hypertens. 2003;21(6):1011-53.
14. Sociedade Brasileira de Cardiologia; Sociedade Brasileira de Hipertensao; Sociedade Brasileira de Nefrologia. VI Diretrizes brasileiras de hipertensao. Arq Bras Cardiol. 2010;95(1 supl.1):1-51.
15. Determinants of pulse wave velocity in healthy people and in the presence of cardiovascular risk factors: ‘establishing normal and reference values’. The Reference Values for Arterial Stiffness’ Collaboration. Eur Heart J. 2010;31(19):2338-50.
16. Engelen L, Ferreira I, Stehouwer CD, Boutouyrie P, Laurent S, on behalf of the Reference Values for Arterial Measurements Collaboration. Reference intervals for common carotid intima-media thickness measured with echotracking: relation with risk factors. Eur Heart J. 2012;34(30):2368-80.
17. O´Brien E, Petrie J, Littler W, de Swiet M, Padfield PL, Altman DG, et al. Short report: an outline of the revised British. Hypertension Society protocol for the evaluation of blood pressure measuring devices. J Hypertens. 1993;11(6):677-9.
18. O´Brien E, Mee F, Atkins N, Thomas M. Evaluation of three devices for self-measurementof blood pressure according to the revised British Hypertension SocietyProtocol: the Omron HEM-705CP, Philips HP 5332, and Nissei DS-175. Blood Press Monit. 1996;1(1):55-61.
19. Martinez LR, Miname MH, Bortolotto LA, Chacra AP, Rochitte CE, Sposito AC, et al. No correlation and low agreement of imaging and inflammatory atherosclerosis’ markers in familial hypercholesterolemia. Atherosclerosis. 2008;200(1):83-8.
20. Guimaraes GV, Ciolac EG, Carvalho VO, D’Avila VM, Bortolotto LA, Bocchi EA. Effects of continuous vs. interval exercise training on blood pressure and arterial stiffness in treated hypertension. Hypertens Res. 2010;33(6):627-32.
21. Drager LF, Bortolotto LA, Figueiredo AC, Silva BC, Krieger EM, Lorenzi-Filho G. Obstructive sleep apnea, hypertension, and their interaction on arterial stiffness and heart remodeling. Chest. 2007;131(5):1379-86.
22. Silva RC, Brunorio L, Giribela CR, Bortolotto LA, Wolosker N, Consolim-Colombo FM. Distances walked in the six-minute walk test: suggestion of defining characteristic for the nursing diagnosis Ineffective Peripheral Tissue Perfusion. Rev Lat Am Enfermagem. 2012;20(2):251-8.
23. Laurent S, Caviezel B, Beck L, Girerd X, Billaud E, Boutouyrie P, et al. Carotid artery distensibility and distending pressure in hypertensive humans. Hypertension. 1994;23(6 Pt 2):878-83.
24. Hoeks AP, Brands PJ, Smeets FA, Reneman RS. Assessment of the distensibility of superficial arteries. Ultrasound Med Biol. 1990;16(2):121-8.
25. Hoeks AP, Willekes C, Boutouyrie P, Brands PJ, Willigers JM, Reneman RS. Automated detection of local artery wall thickness based on M-line signal processing. Ultrasound Med Biol. 1997;23(7):1017-23.
26. Boutouyrie P, Bussy C, Lacolley P, Girerd X, Laloux B, Laurent S. Association between local pulse pressure, mean blood pressure, and large-artery remodeling. Circulation. 1999;100(13):1387-93.
27. Santos PC, Alvim Rde O, Ferreira NE, de Sá Cunha R, Krieger JE, Mill JG, et al. Ethnicity and arterial stiffness in Brazil. Am J Hypertens. 2011;24(3):278-84.
28. Miname MH, Ribeiro MS, Parga Filho J, Avila LF, Bortolotto LA, Martinez LR, et al. Evaluation of subclinical atherosclerosis by computed tomography coronary angiography and its association with risk factors in familial hypercholesterolemia. Atherosclerosis. 2010;213(2):486-91.
29. Zureik M, Temmar M, Adamopoulos C, Bureau JM, Courbon D, Thomas F, et al. Carotid plaques, but not common carotid intima-media thickness, are independently associated with aortic stiffness. J Hypertens. 2002;20(1):85-93.
30. Koivistoinen T, Virtanen M, Hutri-Kähönen N, Lehtimäki T, Jula A, Juonala M, et al. Arterial pulse wave velocity in relation to carotid intima-media thickness brachial flow-mediated dilation and carotid artery distensibility: the Cardiovascular Risk in Young Finns Study and the Health 2000 Survey. Atherosclerosis. 2012;220(2):387-93.
432

Review Article
Effects of Yoga in Patients with Chronic Heart Failure: A Meta-AnalysisMansueto Gomes-Neto1, Erenaldo Sousa Rodrigues-Jr1, Walderi Monteiro Silva-Jr2, Vitor Oliveira Carvalho2
Universidade Federal da Bahia1, Salvado, BA; Universidade Federal de Sergipe2, Aracaju, SE - Brazil
KeywordsYoga; Heart Failure; Complementary Therapies/utilization;
Exercise Therapy; Meta-Analysis.Mailing Address: Mansueto Gomes Neto •Av Reitor Miguel Calmon, s/n, Vale do Canela. Postal Code 40.110-100, Salvador, BA – BrazilEmail: [email protected]; [email protected] received February 20, 2014; revised manuscript June 30, 2014; accepted July 28, 2014.
DOI: 10.5935/abc.20140149
AbstractThe use of yoga as an effective cardiac rehabilitation in
patients with chronic heart failure (CHF) remains controversial. We performed a meta-analysis to examine the effects
of yoga on exercise capacity and health-related quality of life (HRQOL) in patients with CHF. Methods: We searched MEDLINE, Cochrane Central Register of Controlled Trials, Excerpta Medica database, LILACS, Physiotherapy Evidence Database, The Scientific Electronic Library Online, and Cumulative Index to Nursing and Allied Health (from the earliest date available to December 2013) for randomized controlled trials (RCTs) examining the effects of yoga versus exercise and/or of yoga versus control on exercise capacity (peakVO2) and quality-of-life (HRQOL) in CHF. Two reviewers selected studies independently. Weighted mean differences (WMDs) and 95% confidence intervals (CIs) were calculated, and heterogeneity was assessed using the I2 test.
Two studies met the selection criteria (total: 30 yoga and 29 control patients). The results suggested that yoga compared with control had a positive impact on peak VO2 and HRQOL. Peak VO2, WMD (3.87 95% CI: 1.95 to 5.80), and global HRQOL standardized mean differences (−12.46 95% CI: −22.49 to −2.43) improved in the yoga group compared to the control group.
Yoga enhances peak VO2 and HRQOL in patients with CHF and could be considered for inclusion in cardiac rehabilitation programs. Larger RCTs are required to further investigate the effects of yoga in patients with CHF.
IntroductionChronic heart failure (CHF) can be considered the end stage
of heart disease. This syndrome is clinically characterized by poor exercise capacity and quality of life. In context, exercise training is widely recognized as non-pharmacological intervention to improve patient's exercise tolerance and quality of life1.
Despite the well-known benefits of exercise training in patients with CHF, such as improvements in peak
oxygen consumption (peak VO2) and health-related quality of life (HRQOL) and reduced heart failure-related hospitalizations2, there is no consensus regarding which method of exercise is the most efficient. On the other hand, cardiac rehabilitation teams employ non-conventional methods of exercise training according to patient preference and availability, such as hydrotherapy3, dance4, and yoga5.
Yoga is a relaxation and meditation technique based on postures, exercises, and breathing techniques that have various medical benefits in the treatment of anxiety6, depression7, breast cancer8, chronic low back pain9, and hypertension10. A systematic review on yoga in patients with heart diseases was recently published11. It clarified many clinical aspects of yoga; however, the main outcome measures were mortality, non-fatal cardiac events, exercise capacity, HRQOL, and modifiable cardiac risk factors.
Meta-analyses have never been performed to investigate the outcomes of yoga in patients with CHF. It is known that meta-analysis technique minimizes subjectivity by standardizing treatment implications of relevant studies into effect sizes, pooling the data, and then analyzing it to draw conclusions. The aim of this systematic review was to meta-analyze published randomized controlled trials (RCTs) that investigated the effects of yoga in peakVO2 and HRQOL in patients with CHF.
Methods
Eligibility Criteria
Types of studiesThis meta-analysis included RCTs that examined the
impact of any type of yoga in patients with CHF. Studies were considered for inclusion regardless of their publication status, language, or size.
Types of participantsTrials enrolling patients with systolic or diastolic CHF
were included in this meta-analysis. To be eligible, a trial required patients with CHF randomized to at least one group of any type of yoga. The studies that enrolled patients with any kind of respiratory diseases were excluded from this systematic review.
Types of outcome measuresThe main outcomes of interest were peak oxygen
consumption (mL/kg/min) measured by gas analysis and HRQOL (measured by any questionnaire).
433

Review Article
Gomes-Neto et al.Yoga and heart failure
Arq Bras Cardiol. 2014; 103(5):433-439
Search methods for identification of studies
Electronic searchesWe searched for references on MEDLINE via PubMed,
LILACS, Excerpta Medica database (EMBASE), The Scientific Electronic Library Online, Cumulative Index to Nursing and Allied Health, Physiotherapy Evidence Database (PEDro), and Cochrane Central Register of Controlled Trials up to December 2013, without language restrictions. A standard protocol for this search was developed and whenever possible, controlled vocabulary (medical subject heading term for MEDLINE and Cochrane, and Emtree (a life science thesaurus) for EMBASE) were used. Keywords and their synonyms were used to sensitize the search. Table 1 presents the search strategy for MEDLINE via PubMed.
For the identification of RCTs in PubMed/MEDLINE, the optimal sensitive strategy developed by the Cochrane Collaboration was used10. To identify the RCTs in EMBASE, a search strategy using similar terms was adopted. In the search strategy, there were four groups of keywords: study design, participants, interventions, and outcome measures. All eligible articles for this meta-analysis had their references analyzed in order to detect other potentially eligible studies. For ongoing studies or when the confirmation of any data or additional information was needed, the authors were contacted by e-mail.
Data collection and analysis
Assessment of study eligibilityThe previously described search strategy was used to
obtain titles and abstracts of studies that might be relevant for this review. Each abstract identified in the research was independently evaluated by two authors. If at least one of the authors considered one reference eligible, the full text was obtained for complete assessment.
In a similar fashion, two authors independently evaluated full-text articles for eligibility and filled inclusion and exclusion criteria in a standard form. A standardized data extraction form was used for the inclusion and exclusion criteria. In case of any disagreement, the authors discussed the reasons for their decisions and a final decision was made by consensus.
Data extractionTwo authors independently extracted data from the
published reports using standard data extraction forms adapted from the Cochrane Collaboration's12 model for data extraction, considering 1) aspects of the study population, such as the average age and sex; 2) aspects of the intervention performed (sample size, type of yoga performed, presence of supervision, frequency, and duration of each session); 3) follow-up; 4) loss to follow-up; 5) outcome measures; and 6) presented results. Disagreements were resolved by one of the authors. Any further information required from the original author was requested by e-mail.
Risk of bias of included studiesThe risk of bias of included studies was assessed independently
by two authors using the Cochrane Collaboration’s Risk of Bias tool12. The following criteria were assessed: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, intention-to-treat analysis, and completeness of follow-up.
Quality of meta-analysis evidenceThe quality of evidence generated by this meta-analysis
was classified using the PEDro scale. There are several scales for assessing the quality of RCTs. The PEDro scale assesses the methodological quality of a study based on important criteria, such as concealed allocation, intention-to-treat analysis, and the adequacy of follow-up. These characteristics make the PEDro scale a useful tool for assessing the quality of physical therapy and rehabilitation trials13.
Methodological quality was independently assessed by two researchers. Studies were scored on the PEDro scale based on the Delphi list, which consisted of 11 items. One item on the PEDro scale (eligibility criteria) is related to external validity and is generally not used to calculate the method score, leaving a score range of 0 to 10. Any disagreements were resolved by a third rater14,15.
Statistical assessmentPooled effect estimates were obtained by comparing the
least square mean percentage change from baseline to study end for each group, and were expressed as the weighted mean difference (WMD) between groups. Calculations were performed using a fixed effects model. One comparison was made: yoga versus control group. An α value of 0.05 was considered statistically significant. Statistical heterogeneity of the treatment effect among studies was assessed using Cochran's Q test and the inconsistency I2 test, in which values above 25% and 50% were considered indicative of moderate and high heterogeneity, respectively16. All analyses were conducted using Review Manager version 5.0 (Cochrane Collaboration)17.
Results
Description of selected studiesThe initial search led to the identification of 10 abstracts,
from which 4 studies were considered as potentially relevant and were retrieved for detailed analysis. After a complete reading of four articles, two were excluded because although yoga was used as a treatment, the sample had patients with other cardiac diseases. Only two papers18,19 met the eligibility criteria. Figure 1 shows the PRISMA20 flow diagram of studies in this review.
The remaining two articles were fully analyzed and approved by both reviewers and data were extracted from each RCT. Table 2 individually displays the results of the assessment of the PEDro scale. The studies failed to provide sufficient detail for us to assess the potential risk of bias. Information regarding the generation and concealment of the random allocation sequence was not reported. The two
434

Review Article
Gomes-Neto et al.Yoga and heart failure
Arq Bras Cardiol. 2014; 103(5):433-439
Table 1 – Search strategy for MEDLINE via PubMed for yoga and heart failure trials
1. Randomized controlled trials/
2. Random allocation/
3. Controlled clinical Trials/
4. Control groups/
5. Clinical trials OR clinical trials, phase I OR clinical trials, phase II OR clinical trials, phase III OR clinical trials, phase IV/
6. Clinical trials data monitoring committees/
7. Double-blind method/
8. Single-blind method/
9. Placebos/
10. Placebo effect/
11. Cross-over studies/
12. Multicenter Studies/
13. 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR 9 OR 10 OR 11 OR 12
14. Heart failure/
15. Cardiomyopathy, dilated/
16. Heart failure, diastolic/
17. Heart failure, systolic
18. Cardiac output, low/
19. 14 OR 15 OR 16 OR 17 OR 18
20. Yoga
21. Yogic/
22. Asana/
23. Pranayama/
24. 20 OR 21 OR 22 OR 23
25. 13 AND 19 AND 24
studies presented objective evidence of balance in baseline characteristics and stated that they took measures to blind those involved in assessments.
Study characteristicsThe final sample size ranged from 1918 to 4019, and
the mean age of participants ranged from 51 to 54 years. The two studies included patients of both genders, but there was a predominance of males. All studies analyzed in this review included out-patients with documented heart failure New York Heart Association class I–III. One study included patients with systolic and diastolic CHF17, and the other just systolic CHF18. Furthermore, one study reported the race of the patients (95% were African American)19.
Outcomes of included studies
Peak VO2
In both studies, peak VO2 was assessed by a cardiopulmonary exercise test and a treadmill was used for the graded exercise test18,19.
HRQOLThe Minnesota Living with Heart Failure Questionnaire was
used in both studies18,19. Table 3 presents summary data from the two RCTs eligible for this systematic review.
Characteristics of intervention programsThe characteristics of the intervention (yoga) were
reported in the studies. The duration of the yoga program ranged from 819 to 1018 weeks. Regarding the time of the session, there was a variation from 6018 to 7019 min. In the study by Pullen et al18, during each session, subjects completed the following: a 10-min warm-up phase, a 40-min period of standing or seated yoga postures (asana), and finally a 20-min relaxation phase including breathing exercises (pranayama), and meditation. A 5-min warm-up phase including breathing exercises (pranayama), a 40-min period of standing and/or seated yoga postures (asana), and finally, a 15-min relaxation phase were used in the other study19. Both studies used hatha yoga intervention.
The frequency of sessions was two times a week in both studies18,19. Yoga sessions were conducted by a registered yoga teacher (Yoga Alliance) certified by the American College of Sports Medicine.
The analyzed studies reported that both treatment groups (yoga and control) received an educational program and a brochure with instructions for following a home walk program (standard medical treatment). Both groups were followed by blinded researchers from the beginning to the end of the study.
Peak VO2
Both studies assessed peak VO2 as an outcome18,19. The meta-analyses showed (Figure 2) a significant improvement in peak VO2 of 3.87 mL·kg−1·min−1 (95% confidence interval (CI): 1.95, 5.80, N = 59) for participants in the yoga group compared with controls.
Quality of lifeBoth studies assessed HRQOL18,19. Significant enhancements
were found among patients in the yoga group compared to the control group. Due to the difference between the instruments used in the measurement of quality of life, we performed a meta-analysis with a standardized mean difference. The meta-analyses showed (Figure 3) significant improvement in HRQOL of −12.46 (95% CI: −22.49, −2.43, n = 59) for participants in the yoga group in comparison to controls.
DiscussionIn the present systematic review, a meta-analysis of
two studies demonstrated augmentations in peak VO2 and HRQOL in patients with CHF after yoga sessions when compared to controls.
Yoga is an emerging therapy for the rehabilitation of chronic diseases. However, to date, no meta-analysis examined the impact of yoga in patients with CHF. This review is important because it analyzes yoga as a potential modality in cardiovascular rehabilitation.
435
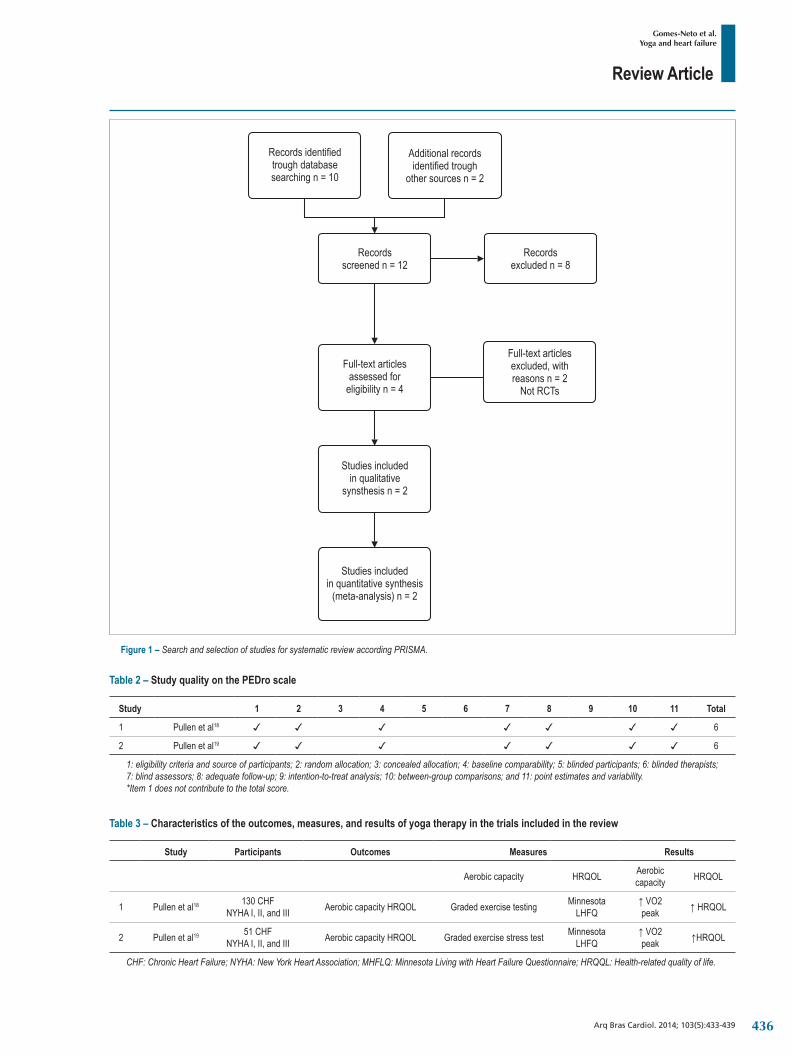
Review Article
Gomes-Neto et al.Yoga and heart failure
Arq Bras Cardiol. 2014; 103(5):433-439
Figure 1 – Search and selection of studies for systematic review according PRISMA.
Records identifiedtrough databasesearching n = 10
Additional recordsidentified trough
other sources n = 2
Recordsscreened n = 12
Recordsexcluded n = 8
Full-text articlesassessed for
eligibility n = 4
Full-text articlesexcluded, withreasons n = 2
Not RCTs
Studies includedin qualitative
synsthesis n = 2
Studies includedin quantitative synthesis
(meta-analysis) n = 2
Table 2 – Study quality on the PEDro scale
Study 1 2 3 4 5 6 7 8 9 10 11 Total
1 Pullen et al18 ✓ ✓ ✓ ✓ ✓ ✓ ✓ 6
2 Pullen et al19 ✓ ✓ ✓ ✓ ✓ ✓ ✓ 6
1: eligibility criteria and source of participants; 2: random allocation; 3: concealed allocation; 4: baseline comparability; 5: blinded participants; 6: blinded therapists; 7: blind assessors; 8: adequate follow-up; 9: intention-to-treat analysis; 10: between-group comparisons; and 11: point estimates and variability.*Item 1 does not contribute to the total score.
Table 3 – Characteristics of the outcomes, measures, and results of yoga therapy in the trials included in the review
Study Participants Outcomes Measures Results
Aerobic capacity HRQOL Aerobic capacity HRQOL
1 Pullen et al18 130 CHFNYHA I, II, and III Aerobic capacity HRQOL Graded exercise testing Minnesota
LHFQ↑ VO2 peak ↑ HRQOL
2 Pullen et al19 51 CHFNYHA I, II, and III Aerobic capacity HRQOL Graded exercise stress test Minnesota
LHFQ↑ VO2 peak ↑HRQOL
CHF: Chronic Heart Failure; NYHA: New York Heart Association; MHFLQ: Minnesota Living with Heart Failure Questionnaire; HRQQL: Health-related quality of life.
436

Review Article
Gomes-Neto et al.Yoga and heart failure
Arq Bras Cardiol. 2014; 103(5):433-439
Figure 2 – Yoga versus controls: VO2 Peak. Review Manager (version 5.2; the Cochrane Collaboration, 2013). SD: standard deviation; CI = Confidence intervals
Study or SubgroupYoga
Mean SD Total Mean SD Total Weight IV, Fixed, 95% ClControl Mean Difference Mean Difference
IV, Fixed, 95% ClPullen et al 2008Pullen et al 2010
Total (95% Cl)
3.33.11
53.04
921
-1.1-0.65
5.23.73
1019
17.6%82.4%
4,40 (-0.19, 8.99)3,76 (1.64, 5.88)
29 100.0% 3,87 (1.95, 5.80)30Heterogeneity: Chi = 0.06, df = 1 (p = 0.80); I = 0%2 2
Z = 3.94 (p < 0.0001)Teste for overall effect:-20 -10 0 10 20
Favours (Control) Favours (Yoga)
Figure 3 – Yoga versus controls: Quality of Life. Review Manager (version 5.2; the Cochrane Collaboration, 2013). SD: standard deviation; CI: Confidence intervals.
Study or SubgroupYoga
Mean SD Total Mean SD Total Weight IV, Fixed, 95% ClControl Mean Difference Mean Difference
IV, Fixed, 95% Cl
Pullen et al 2008Pullen et al 2010
Total (95% Cl)
-6.9-11.56
16.819.18
921
1.31.93
32.116.87
1019
19.5%80.5%
-8.20 (-30.92, 14.52)-13.49 (-24.66, -2.32)
29 100.0% -12.46 (-22.49, -2.43)30Heterogeneity: Chi = 0.17, df = 1 (p = 0.68); I = 0%2 2
Z = 2.44 (p < 0.01)Test for overall effect: -20 -10 0 10 20Favours (Control)Favours (Yoga)
Our meta-analysis showed 22.0% improvement in peak VO2 in the yoga group. The mean peak VO2 in the two studies analyzed was 15.85 mL·kg−1·min−1 at baseline and 19.05 mL·kg−1 ·min−1 at the end of the intervention. Specifically, the WMD in peak VO2 peak was 3.97 mL·kg−1 ·min−1 from baseline to post-intervention. The magnitude of change is similar to a previous meta-analysis that evaluated the effect of different modalities of exercise in patients with CHF21,22.
Another important factor to be described is the extent of the improvement and the peak VO2 of 19.05 mL·kg−1 ·min−1 achieved after the intervention. A minimum peak VO2 of 15 mL·kg−1 ·min−1 in women and 18 mL·kg−1 ·min−1 in men aged 85 years has been demonstrated to be necessary for full and independent living (e.g., garden activities, walking up stairs, etc.)23. Thus, yoga patients with CHF improve their medical condition, so they can productively carry out everyday activities.
In this study, yoga is shown to be effective in the rehabilitation of patients with CHF. Considering peak VO2, it is well known that improvements above 10% after a cardiovascular rehabilitation program are satisfactory and represents a good prognosis in patients with CHF24.
The assessment of the HRQOL is an essential outcome in the rehabilitation process. It is recognized that HRQOL is also associated with mental and physical status. Yoga is reported to improve important mental endpoints, such as anxiety and depression. In addition, yoga has been found to be critical for the enhancement of patients' exercise capacity.
In regards to HRQOL, our meta-analysis showed a 24.1% increase in the yoga group. The mean of MLFHQ of both studies analyzed was 37.5 at baseline and 28.45 at the end of the intervention, demonstrating an improvement of nine points on the scale. The study by Arnold et al25 showed that the minimal clinically important difference for the MLFHQ is five points. The WMD in the MLFHQ was −12.46 from baseline to post-intervention. The magnitude of change is similar to that reported in a previous meta-analysis study that included six RCTs about exercise in CHF25.
Our results are similar to the ones found in previous studies concerning exercise training21,22,26. The adherence of patients with CHF to exercise training is low; therefore, the investigation of new strategies is important in the context of rehabilitation. Despite the best method to improve exercise capacity and/or HRQOL, the first point that should be considered is patient preference. Taking this into account, the number of subjects that drop out of cardiovascular rehabilitation programs could possibly be decreased.
This review is limited because we did not consider the strict description of the criteria used by the authors to diagnose CHF, which can compromise the reliability of the results. It is not possible to consistently recommend yoga in patients with CHF. Our search strategy only found two RCTs with small samples and low duration of intervention. Furthermore, different variables may influence the effects of yoga as a therapy, such
437

Review Article
Gomes-Neto et al.Yoga and heart failure
Arq Bras Cardiol. 2014; 103(5):433-439
1. Piepoli MF, Conraads V, Corrà U, Dickstein K, Francis DP, Jaarsma T, et al. Exercise training in heart failure: from theory to practice: a consensus document of the Heart Failure Association and the European Association for Cardiovascular Prevention and Rehabilitation. Eur J Heart Fail. 2001;13(4):347-57.
2. Davies EJ, Moxham T, Rees K, Singh S, Coats AJ, Ebrahim S, et al. Exercise training for systolic heart failure: Cochrane systematic review and meta-analysis. Eur J Heart Fail. 2010;12(7):706-15.
3. Cider A, Schaufelberger M, Sunnerhagen KS, Andersson B. Hydrotherapy--a new approach to improve function in the older patient with chronic heart failure. Eur J Heart Fail. 2003;5(4):527-35.
4. Belardinelli R, Lacalaprice F, Ventrella C, Volpe L, Faccenda E. Waltz dancing in patients with chronic heart failure: new form of exercise training. Circ Heart Fail. 2008;1(2):107-14.
5. Howie-Esquivel J, Lee J, Collier G, Mehling W, Fleischmann K.Yoga in heart failure patients: a pilot study. J Cardiac Fail. 2010;16(9):742-9.
6. Kirkwood G, Rampes H, Tuffrey V, Richardson J, Pilkington K. Yoga for anxiety: a systematic review of the research evidence. Br J Sports Med. 2005;39(12):884-91.
7. Cramer H, Lauche R, Langhorst J, Dobos G. Yoga for depression: a systematic review and meta-analysis. Depress Anxiety. 2013;30(11):1068-83.
8. Zhang J, Yang KH, Tian JH, Wang CM. Effects of yoga on psychologic function and quality of life in women with breast cancer: a meta-analysis of randomized controlled trials. J Altern Complement Med. 2012;18(11):994-1002.
9. Holtzman S, Beggs RT. Yoga for chronic low back pain: a meta-analysis of randomized controlled trials. Pain Res Manag. 2013;18(5):267-72.
10. Hagins M, States R, Selfe T, Innes K. Effectiveness of yoga for hypertension: systematic review and meta-analysis. Evid Based Complement Alternat Med. 2013;2013:649836.
11. Cramer H, Lauche R, Haller H, Gustav Dobos G, Michalsen A. A systematic review of yoga for heart disease . Eur J Prev Cardiol. 2014;3:1-12 .
12. Higgins JPT, Green S (eds.) The Cochrane Handbook for Systematic Reviews of Interventions 4.2.6 [updated Sept.2006]. In: The Cochrane Library, Issue 4, 2006. Chichester (UK): John Wiley & Sons, Ltd.; 2006.
13. Olivo SA, Macedo LG, Gadotti IN, Fuentes J, Stanton T, Magee DJ. Scales to assess the quality of randomized controlled trials: a systematic review. PhysTher. 2008;88(2):156–75.
14. Verhagen AP, de Vet HCW, de Bie RA, Kessels AGH, Boers M, Bouter LM, et al. The Delphi List: a criteria list for quality assessment of randomized clinical
trials for conducting systematic reviews developed by Delphi Consensus. J Clin Epidemiol. 1998;51(12):1235–41.
15. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating of quality randomized controlled trials. Phys Ther. 2003;83(8):713–21.
16. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327(7414):557–60.
17. The Cochrane Collaboration. [Internet]. [Cited in 2013 Feb 12]. Available from: http://www.cochrane.org/handbook
18. Pullen PR, Nagamia SH, Mehta PK, Thompson WR, Benardon D, Hammoud R, et al. Effects of yoga on inflammation and exercise capacity in patients with chronic heart failure. J Cardiac Fail. 2008;14(5):407-13.
19. Pullen PP, Thompson WR, Benardon D, Brandon J, Mehta PK, Rifai L, et al. Benefits of yoga for African American Heart Failure Patients. Med Sci Sports Exerc. 2010; 42(4): 651–7.
20. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA GROUP. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009; 339: b2535.
21. Haykowsky MJ, Liang Y, Pechter D, Jones LW, McAlister FA, Clark AM. A meta-analysis of the effect of exercise training on left ventricular remodeling in heart failure patients: the benefit depends on the type of training performed. J Am Coll Cardiol. 2007;49(24):2329-36.
22. Haykowsky MJ, Timmons MP, Kruger C, McNeely M, Taylor DA, Clark AM. Meta-analysis of aerobic interval training on exercise capacity and systolic function in patients with heart failure and reduced ejection fractions. Am J Cardiol. 2013;111(10):1466-9.
23. Paterson DH, Cunningham DA, Koval JJ, St Croix CM. Aerobic fitness in a population of independently living men and women aged 55–86 years. Med Sci Sports Exerc.1999;31(12):1813–20.
24. Frankenstein L, Nelles M, Hallerbach M, Dukic D, Fluegel A, Schellberg D, et al. Prognostic impact of peakVO2-changes in stable CHF on chronic beta-blocker treatment. Int J Cardiol. 2007; 122(2):125-30.
25. Arnold M, Rajda M, Ignaszewski A, Howlett J, Leblanc M-H. Changes in the Minnesota living with heart failure questionnaire score and clinical outcomes in a large contemporary population of ambulatory heart failure patients in the Canadian Heart Failure Network. J Card Fail. 2012;18 (8 Supplement):S79.
26. Davies EJ, Moxham T, Rees K, Singh S, Coats AJS, Ebrahim S. Exercise training for systolic heart failure: Cochrane systematic review and meta-analysis. Eur J Heart Fail. 2010; 12 (7): 706-15.
References
as personal approach and culture. Despite this, yoga appears to be an interesting means of cardiac rehabilitation and deserves further investigation with better-controlled RCTs.
ConclusionConsidering the available data, our meta-analysis showed
that yoga improved peak VO2 and HRQOL in patients with CHF. Yoga should be considered as an alternative method of exercise training in patients with CHF.
Author contributionsConception and design of the research and Writing of
the manuscript: Gomes-Neto M, Rodrigeus-Jr ES, Carvalho VO; Acquisition of data: Rodrigeus-Jr ES, Carvalho VO;
Analysis and interpretation of the data and Statistical analysis: Gomes-Neto M, Silva-Jr WM; Critical revision of the manuscript for intellectual content: Gomes-Neto M, Silva-Jr WM, Carvalho VO.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis study is not associated with any thesis or dissertation work.
438

Review Article
Gomes-Neto et al.Yoga and heart failure
Arq Bras Cardiol. 2014; 103(5):433-439439

Letter to the Editor
ACE I/D Gene Polymorphism in Children with Family History of Premature Coronary DiseaseDilek Yý lmaz Çiftdoð anÝ zmir Tepecik Training and Research Hospital, Turquia
Mailing Address: Dilek Yý lmaz Çiftdoð an •Ý zmir Tepecik Training and Research Hospital, Department of Pediatrics, Ý zmir. Postal Code: 35100, Ý Zmir - TurquiaEmail: [email protected] received July 22, 2014, revised manuscript August 28, 2014; accepted August 28, 2014.
KeywordsPolymorfism, Genetic; Peptidyl-Dipeptidase A; Coronary
Artery Disease; Child.
DOI: 10.5935/abc.20140182
Letter to the editor regarding the article by de Albuquerque et al: Angiotensin-converting enzyme genetic polymorphism: its impact on cardiac remodeling.
I read with interest the recent review article by de Albuquerque et al1 published in the Arquivos Brasileiros de Cardiologia entitled “Angiotensin-converting enzyme genetic polymorphism: its impact on cardiac remodeling.” They showed that the DD genotype of Angiotensin-converting enzyme (ACE) gene polymorphism was independently associated with worse echocardiographic outcome, while the DI genotype, with the best echocardiographic profile1.
Atherosclerosis, the major cause of CAD, manifests clinically in adulthood. However, this disease begins very early in life, often during childhood. Genetic and environmental factors, gene–environment interaction effects also come into play in the development of atherosclerosis. Family history is the most significant independent risk factor for CAD.
In our study, we included a total of 140 children, 72 males and 68 females between the ages of 4.9 and 15.7 years. Among these children, 73 had a parental history of premature CAD (parents have been diagnosed with the CAD by coronary angiographic study, ages below 55 for men and 65 for women) and the rest of 67 belonged to our control group (parents have shown normal coronary angiographic study). The participants were screened for the mutations ACE I/D gene polymorphisms.
The genotypes of ACE I/D were significantly different between the study and control groups (p = 0.01). The frequency of D/D genotype was significantly higher in the study group than the control group (respectively, 20/73 vs. 3/67, p = 0.01) (Table 1). The frequency of the D allele was slightly higher in study group (0.52) than in control group (0.27) (p = 0.005).
The angiotensin converting enzyme is a key factor in the production of angiotensin II and in the degradation of bradykinin. Chronic exposure to high levels of circulating and tissue ACE predispose to vascular wall thickening and atherosclerosis. The ACE insertion/deletion (I/D)
polymorphism results from the absence or presence of an alu repeat located in intron 16 of the ACE gene. The D allele of an insertion/deletion (I/D) polymorphism of the gene encoding ACE is associated with higher plasma ACE concentrations2. Many studies have investigated the association between the DD genotype of ACE gene I/D polymorphic variant and CAD3,4. However, these outcomes have not been supported by the other studies5. In present study, the frequencies of D/D genotype and D allel of ACE gene considerably higher in children with parental history of premature CAD than control group.
We showed that the frequencies of the DD genotype and the D allel of ACE I/D gene polymorphism are higher in children with parental history of premature CAD. This results may be associated with an increased risk for development of atherosclerosis. It may be contribute to the detection of the risk of children with a parental history of CAD. Thus, further large population studies must be done to confirm this results.
The study protocol was approved by the Local Ethical Committee of Celal Bayar University, and informed written consent was obtained from all participants. This study was funded by Celal Bayar University.
Additional information:In addition to ACE I/D gene polymorphism, glycoprotein
IIIa, factor V G1691A, factor V H1299R, prothrombin G20210A and apolipoprotein E polymorphism had been investigated in the same study group. These results were published in various journals.
* Ciftdoğan DY. Glycoprotein IIIa gene polymorphism in children with a family history of premature coronary artery disease. Acta Cardiol. 2010 Dec;65(6):695; author reply 695-6.
** Ciftdoğan DY, Coşkun S, Ulman C, Tikiz H. The factor V G1691A, factor V H1299R, prothrombin G20210A polymorphisms in children with family history of premature coronary artery disease. Coron Artery Dis. 2009 Nov;20(7):435-9. doi: 10.1097/MCA.0b013e32832bdb8c.
*** Ciftdoğan DY, Coskun S, Ulman C, Tıkız H. The association of apolipoprotein E polymorphism and lipid levels in children with a family history of premature coronary artery disease. J Clin Lipidol. 2012 Jan-Feb;6(1):81-7. doi: 10.1016/j.jacl.2011.06.017. Epub 2011 Jul 30.
440

Letter to the Editor
DilekACE I/D Gene Polymorphism in Children
Arq Bras Cardiol. 2014; 103(5):440-442
1. de Albuquerque FN, Brandao AA, da Silva DA, Mourilhe-Rocha R, Duque GS, Gondar AF, et al. Angiotensin-converting enzyme genetic polymorphism: its impact on cardiac remodeling. Arq Bras Cardiol. 2014;102(1):70-9.
2. Sobti RC, Maithil N, Thakur H, Sharma Y, Talwar KK. Association of ACE and Factor VII gene variability with the risk of coronary heart disease in north Indian population. Mol Cell Biochem. 2010;341(1-2):87-98.
3. Beohar N, Damaraju S, Prather A, Yu QT, Raizner A, Kleiman NS, et al. Angiotensin-I converting enzyme genotype DD is a risk factor for coronary artery disease. J Investig Med. 1995;43(3):275-80.
4. Cambien F, Poirier O, Lecerf L, Evans A, Cambou JP, Arveiler D, et al. Deletion polymorphism in the gene for angiotensin-converting enzyme is a potent risk factor for myocardial infarction. Nature. 1992;359(6396):641-4.
5. Shafiee SM, Firoozrai M, Salimi S, Zand H, Hesabi B, Mohebbi A. Angiotensin converting enzyme DD genotype not associated with increased risk of coronary artery disease in the Iranian population. Pathophysiology. 2010;17(3):163-7.
References
Table 1 – The frequencies of the ACE I/D gene polymorphisms in study group and control group, and the odds ratios with 95% CI
Genetic polymorphismStudy group
(Children whose parents with premature CAD) n (%)
Control group(Children whose parents without
premature CAD) n (%)p Value Odds Ratios (CI 95%)
ACE
D/D 20 (27.4%) 3 (4.4%)
0.01 2.98 (1.12 – 6.82)1D/I 37 (50.6%) 30 (44.6%)
I/I 16 (21.9%) 34 (50.0%)1 : D/D versus I/D and I/I.
ReplyThe insertion1/deletion (I/D) polymorphism in the gene
for angiotensin converting enzyme (ACE) has been studied in different clinical scenarios beyond heart failure (HF), which is described in this article, such as hypertension1, atrial fibrillation (AF)2, and coronary heart disease (CHD)3. In all these scenarios, there appears to be a relationship between the DD genotype and poor clinical outcome, albeit with some controversy due to the small number of patients.
Typically, the outcomes used in these small studies are surrogate markers such as echocardiographic parameters (original article) or left ventricular hypertrophy1, for example. In other works, it is only possible to detect the relationship between genotypes and incidence of the disease studied2.
In the case of atherosclerosis, because of the prevalence and importance of CHD, there are a greater number of publications such as those presented in letters to the editor on the various types of atherosclerosis: subclinical or clinical. Our work4, in particular, focused only on patients with nonischemic HF, and it was possible to observe the association between poor Echo profile and the DD genotype.
More recently, it has been described tha HF physiopathology and Renin Angiotensin activity is actually linked to a polygenic
heritage. The simultaneous study of multiple genetic polymorphisms (GPs) in the same population has identified that only combinations of genotypes have been associated with clinical and/or echocardiographic outcomes5,6.
Therefore, it is likely that a panel of genetic markers would be more efficient in detecting more severely ill individuals than isolated GPs. Since then, our group has been focusing on this kind of analysis, and preliminary data suggest an association between a genetic panel, which included polymorphisms of the angiotensin-converting enzyme, beta adrenergic receptor type 1, nitric oxide synthetase, and Angiotensin II, and clinical outcomes. The continuation of this study, which is already underway, with more patients may help clarify this issue.
Sincerely,
Felipe Neves de Albuquerque, Andréa Araujo Brandao, Dayse Aparecida da Silva, Ricardo Mourilhe-
Rocha, Gustavo Salgado Duque, Alyne Freitas Pereira Gondar, Luiza Maceira de Almeida Neves, Marcelo
Imbroinise Bittencourt, Roberto Pozzan, Denilson Campos de Albuquerque
441

Letter to the Editor
DilekACE I/D Gene Polymorphism in Children
Arq Bras Cardiol. 2014; 103(5):440-442
1. Pontremoli R, Sofia A, Tirotta A, Ravera M, Nicolella C, Viazzi F, et al. The deletion polymorphism of the angiotensin I-converting enzyme gene is associated with target organ damage in essential hypertension. Am Soc Nephrol. 1996;7(12):2550-8.
2. Topal NP, Ozben B, Hancer VS, Tanrikulu AM, Diz-Kucukkaya R, Fak AS, et al. Polymorphisms of the angiotensin-converting enzyme and angiotensinogen gene in patients with atrial fibrillation. J Renin Angiotensin Aldosterone Syst. 2911;12(4):549-56.
3. Mutthumala A, Montgomery H, Palmen J, Cooper JA, Humphries SE. Angiotensin-converting enzyme genotype interacts with systolic blood pressure to determine coronary heart disease risk in healthy middle-aged men. Hypertension. 2007;50(2):348-53.
4. Albuquerque FN de, Brandao AA, Silva DAD, Mourilhe-Rocha R, Duque GS, Gondar AF, et al. Angiotensin-converting enzyme genetic polymorphism: its impact on cardiac remodeling. Arq Bras Cardiol. 2014;102(1):70-9.
5. Zakrzewski-Jakubiak M, de Denus S, Dubé M-P, Bélanger F, White M, Turgeon J. Ten renin-angiotensin system-related gene polymorphisms in maximally treated Canadian Caucasian patients with heart failure. Br J Clin Pharmacol. 2006;5(5):742-51.
6. Kitsios G, Zintzaras E. Genetic variation associated with ischemic heart failure: a huge review and meta-analysis. Am J Epidemiol. 2007;116(6):619-33.
References
442

Erratum
DOI: 10.5935/abc.2014S001e
Edition of March 2014, vol. 102 (3), Supl. 1, pg. 1-61
The “Brazilian Society of Cardiology Guidelines on Unstable Angina and Non-ST-Segment Elevation Myocardial Infarction (2nd Edition, 2007) – 2013 Updating”, published as supplement number 3 of the March 2014 edition of the Arquivos Brasileiros de Cardiologia [Arq Bras Cardiol. 2014;102(3Supl.1):1-61], has undergone the following corrections:
On page 46, item “Lipid Approach – Summary of Recommendations and Evidence”, sub-item “Class 1 recommendations”, the following text has been considered second topic:
For patients with unstable myocardial ischemic syndromes with no ST-segment elevation and LDL-C ≥ 100 mg/dL, statins should be used if no contraindications apply, aiming at LDL-C < 70 mg/dL (level of evidence: A). If tolerated, statin should be maintained indefinitely.
On page 46, item “Lipid Approach – Summary of Recommendations and Evidence”, sub-item “Class 1 recommendations”, the third topic has been inserted:
If the patient is already on statin, the drug should not be suspended regardless of the LDL-C level (level of evidence: B).On page 46, item “Lipid Approach – Summary of Recommendations and Evidence”, sub-item “Class 2 recommendations”
has been removed.
443

Anatomopathological Session
Case 5/2014 - 41-Year-Old Woman with Rheumatic Disease and Previous Mitral Valve Repair with Pulmonary Embolism and Cardiogenic and Septic ShockEduardo Gomes Lima, Ricardo D’Oliveira Vieira, Paula Bombonati, Jussara Bianchi CastelliInstituto do Coração (InCor) HC-FMUSP, São Paulo, SP - Brazil
Mailing Address: Vera Demarchi Aiello •Av. Dr. Enéas de Carvalho Aguiar, 44, subsolo, bloco I, Cerqueira César. Postal Code 05403-000, São Paulo, SP - BrazilE-mail: [email protected], [email protected]
KeywordsMitral Valve Stenosis / serugery; Pulmonary Embolism;
Acinetobacter Infections; Shock, Cardiogenic; Shock, Septic.
Editor da Seção: Alfredo José Mansur ([email protected])
Editores Associados: Desidério Favarato ([email protected])
Vera Demarchi Aiello ([email protected])
DOI: 10.5935/abc.20140180
intraventricular stimulus conduction disturbance, of the right branch type and decreased left ventricular potential, suggesting right ventricular overload (Figure 1).
The patient was admitted for treatment. She remained in the emergency unit for five days and was admitted (on October 15, 2005). She received furosemide 120 mg intravenously, 40 mg of enalapril, 0.25 mg of digoxin, 50 mg of hydrochlorothiazide and 120 mg of enoxaparin daily by subcutaneous route, as well as dobutamine 10 µg/kg.min intravenously.
At hospitalization she had hypotension, increased edema and creatinine elevation (Table 1). After three days, the patient developed anuria, anasarca and finally shock with hypotension with 60 mmHg despite the use of 15 µg/kg.min of dobutamine.
The laboratory tests (10/20/2005) showed creatinine 3.2 mg/dL and then 5.9 mg / dL, Urea 75 mg / dL and, during evolution, 115 mg / dL (Table 1).
At physical examination (10/20/2005) the patient was in poor general condition, with blood pressure of 80/50 mmHg, heart rate 90 bpm, crackles in both lungs, arrhythmic heart sounds (atrial fibrillation), systolic murmur + / 4 + in the mitral area, ascites and edema ++++ / 4+.
The electrocardiogram (20/10/2005) showed atrial fibrillation, heart rate of 100 bpm, low QRS voltage, intraventricular conduction disturbance of the right bundle branch block type stimulus, decreased left ventricular strength (Figure 2).
The echocardiogram (on October 21) showed normal left ventricle, dilated and hypokinetic right ventricle, mitral valve calcification, commissural fusion, moderate stenosis and moderate tricuspid regurgitation (Table 2). Transesophageal echocardiogram (on October 21) showed pulmonary artery dilation with a large thrombus image (10 × 5.0 cm) extending to its left branch and the presence of autocontrast in the left atrium.
The diagnosis of pulmonary thromboembolism was made and 100 mg of r-TPA was administered intravenously in two hours. The patient went into shock, which required vasoactive drugs. Intravenous norepinephrine was administered, associated with ceftriaxone and metronidazole, as well as vancomycin for empiric treatment of the systemic infection. Mechanical ventilation was initiated with tracheal intubation for ventilatory support.
Pulmonary arteriography (on October 24) showed pulmonary artery pressures of 30/15/22 (systolic/diastolic/mean) mmHg. No images suggestive of pulmonary thromboembolism were identified.
A 41-year-old female sought medical care due to severe dyspnea. The patient had had acute rheumatic disease in childhood. During evolution, she developed mitral stenosis. The symptoms became incapacitating and she underwent mitral commissurotomy at 36 years. She progressed well for a few years until dyspnea recurred and she was once again submitted to surgery, at 41 years, when she underwent mitral valve plasty (03/16/2005).
After the last surgery, she had dyspnea on great exertion for about three months, when it progressed and started to be triggered by middle, and finally by mild exertion, and at three days before hospitalization (10/10/2005), it had become present even at rest. The patient attributed the recent worsening to current medication discontinuation: captopril 25 mg, furosemide 80 mg, 0.25 mg digoxin and warfarin 2.5 mg daily.
Physical examination (10/10/2005) showed the patient was in good general health, dyspneic, with a marked increase in jugular venous pressure, pulse rate of 92 bpm, blood pressure of 100/60 mmHg. Lung examination was normal. Cardiac auscultation showed irregular rhythm without additional heart sounds. Systolic murmur +/4+ was diagnosed in the mitral valve area. There were no alterations at the abdominal examination, but slight edema of the lower limbs.
Laboratory tests (10/10/2005) showed hemoglobin 11.7 g/dL, hematocrit 35%, WBC, 3,900/ mm³, platelets, 12.9000 /mm³, creatinine 1.3 mg / dL, urea 31 mg / dL, sodium 135 mEq/L, potassium 3.6 mEq/L, INR 1.19 and activated partial thromboplastin time (patient / control) 1.09.
The electrocardiogram (10/10/2005) showed frequency of 90 bpm, atrial fibrillation, low voltage QRS complex, undetermined QRS axis in the frontal plane and presence of
e57

Anatomopathological Session
Lima et alAnatomopathological Session
Arq Bras Cardiol. 2014; 103(5):e57-e67
Table 1- Laboratory assessment
17 Oct 20 Oct 26 Oct
Urea (mg/dL) 75 115 97
Creatinine (mg/dL) 3.2 5.9 5.8
Sodium (mEq/L) 135 136 142
Potassium (mEq/L) 3.6 4.5 4.3
Hemoglobin % 12.2 11.3 8
Hematocrit (g/dL) 37 33 27
MCV (µm³) 97 97 108
Leukocytes/mm³ 4.400 6.200 13.400
Neutrophils (%) 67 74 82
Eosinophils (%) 5 3 0
Basophils (%) 1 1 0
Lymphocytes (%) 11 8 13
Monocytes (%) 16 14 5
Platelets/mm³ 186.000 17.500 22.8000
PT (INR) 1.1 2.41
aPPT (rel) 1.27 Incoagulable
Uric acid (mg/dL) 12.1
AST (IU/L) 12
ALT (IU/L) 12
FAALP (N <120 U/L)) 170
Gama GT IUL (N <28) 55
Phosphorus (mg/dL) 8.4
Figure 1 – Atrial Fibrillation, low voltage QRS complexes, right bundle branch block, low voltage of left QRS complexes, right ventricle hypertrophy.
e58
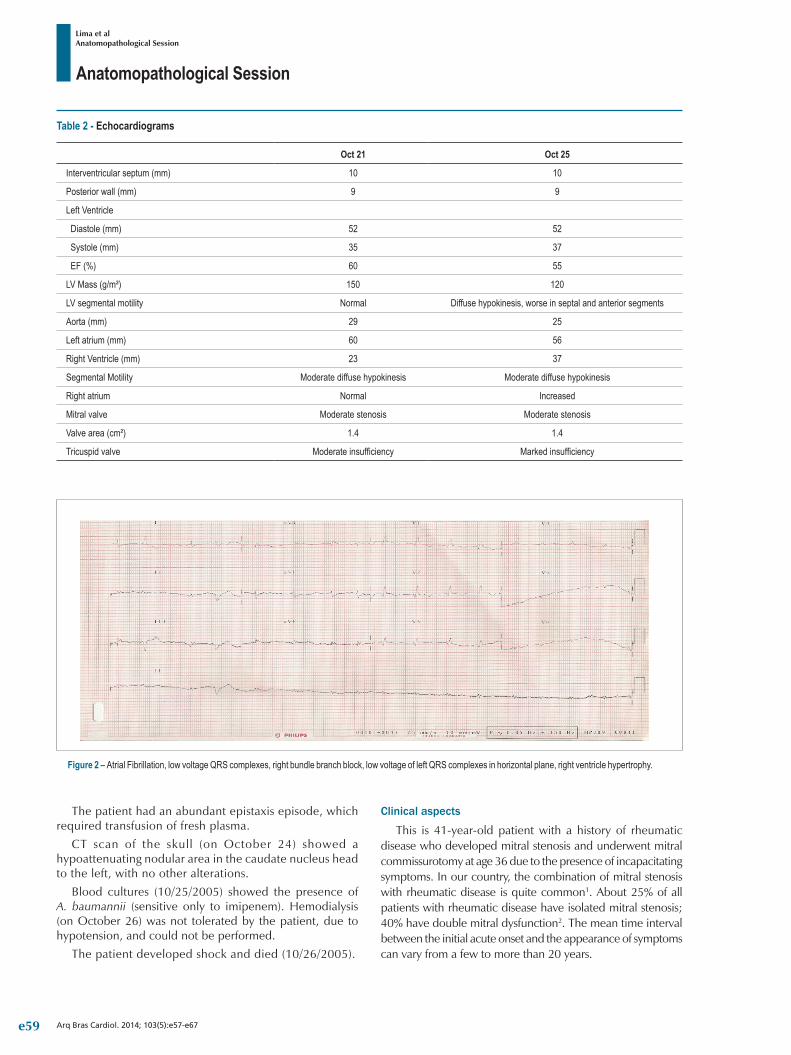
Anatomopathological Session
Lima et alAnatomopathological Session
Arq Bras Cardiol. 2014; 103(5):e57-e67
The patient had an abundant epistaxis episode, which required transfusion of fresh plasma.
CT scan of the skull (on October 24) showed a hypoattenuating nodular area in the caudate nucleus head to the left, with no other alterations.
Blood cultures (10/25/2005) showed the presence of A. baumannii (sensitive only to imipenem). Hemodialysis (on October 26) was not tolerated by the patient, due to hypotension, and could not be performed.
The patient developed shock and died (10/26/2005).
Clinical aspects
This is 41-year-old patient with a history of rheumatic disease who developed mitral stenosis and underwent mitral commissurotomy at age 36 due to the presence of incapacitating symptoms. In our country, the combination of mitral stenosis with rheumatic disease is quite common1. About 25% of all patients with rheumatic disease have isolated mitral stenosis; 40% have double mitral dysfunction2. The mean time interval between the initial acute onset and the appearance of symptoms can vary from a few to more than 20 years.
Table 2 - Echocardiograms
Oct 21 Oct 25
Interventricular septum (mm) 10 10
Posterior wall (mm) 9 9
Left Ventricle
Diastole (mm) 52 52
Systole (mm) 35 37
EF (%) 60 55
LV Mass (g/m²) 150 120
LV segmental motility Normal Diffuse hypokinesis, worse in septal and anterior segments
Aorta (mm) 29 25
Left atrium (mm) 60 56
Right Ventricle (mm) 23 37
Segmental Motility Moderate diffuse hypokinesis Moderate diffuse hypokinesis
Right atrium Normal Increased
Mitral valve Moderate stenosis Moderate stenosis
Valve area (cm²) 1.4 1.4
Tricuspid valve Moderate insufficiency Marked insufficiency
Figure 2 – Atrial Fibrillation, low voltage QRS complexes, right bundle branch block, low voltage of left QRS complexes in horizontal plane, right ventricle hypertrophy.
e59

Anatomopathological Session
Lima et alAnatomopathological Session
Arq Bras Cardiol. 2014; 103(5):e57-e67
The presence of symptoms of heart failure (classes III and IV of the New York Heart Association), together with echocardiographic data that confirm significant anatomic lesion, is crucial for intervention indication: balloon valvuloplasty or surgery (commissurotomy or valve replacement). Whenever possible, there is an attempt to correct the valve defect, keeping the patient’s valve system, postponing prosthesis implantation. In this case, commissurotomy was performed, which maintained the patient well for approximately five years, when she started to present symptoms again, when mitral valve repair was performed. This evolution in the rheumatic patient can occur due to repeated episodes of valvulitis, hence the need to maintain secondary prophylaxis with benzathine penicillin in patients with cardiac involvement, preferably throughout life or up to the fifth decade, when it is not possible1.
After the last surgical intervention, the patient remained asymptomatic for a short time, with dyspnea recurrence that developed into striking symptoms in about three months. The deterioration was attributed to drug discontinuation which, in our country, is a common cause of heart failure decompensation, regardless of the etiology.
On admission, the patient had respiratory distress with clean lungs, irregular heartbeat without incidental heart sounds, minor systolic murmur in the mitral area and mild lower-limb edema. These findings point to a syndromic diagnosis of right heart failure. The normal pulmonary symptomatology and the absence of additional heart sounds do not indicate left ventricular dysfunction the cause of decompensation. The irregular rhythm suggests uns atrial rhythm, which may be atrial fibrillation, a common association with mitral valve disease together with large atriums.
The patient’s initial laboratory tests did not exhibit significant alterations. The electrocardiogram (ECG) confirmed the presence of atrial fibrillation and alterations compatible with right ventricular overload, corroborating the aforementioned physical examination. Moreover, it showed low voltage complexes. The so-called dielectric effect is defined by the presence of QRS complexes with an amplitude < 0.5 mV in the frontal plane leads and < 1 mV in the precordial plane. The etiology is varied, including extracardiac factors (obesity, chronic obstructive pulmonary disease, hypothyroidism), pericardial diseases (pericardial effusion, constrictive pericarditis) and intrinsic myocardial diseases (rheumatic myocarditis, restrictive cardiac syndromes, arrhythmogenic right ventricular dysplasia).
The patient’s initial treatment was directed to heart failure due to systolic dysfunction, consisting of angiotensin-converting enzyme (ACE) inhibitors, diuretics, digitalis and full heparinization due to atrial fibrillation, considering the risk for thromboembolic events. After hospitalization, the patient developed low cardiac output syndrome with hypotension, convergent blood pressure and worsening of renal function, despite the use of inotropic agents (dobutamine). Moreover, there was worsening of the congestive symptoms, with worsening of edema and crackles in both lung. Given this clinical picture, the differential diagnosis includes diseases that present with predominantly right heart failure, leading to shock.
The most likely hypothesis is pulmonary thromboembolism (PTE). In the case of PTE, it would be possible to explain the clinical, electrocardiographic and evolution alterations (“shock with clean lungs”). It should be noted that the patient had risk factors for PTE, with heart failure, atrial fibrillation and valvular heart disease, plus the fact that this disease is responsible for approximately 15% of decompensated heart failure.
Echocardiography was crucial for the patient’s diagnosis. The valvular dysfunction with an area of 1.4 cm2 would hardly justify the patient’s clinical picture alone, or her evolution, considering the undertaken measures. The clear signs of right ventricular dysfunction, with evidence of large thrombus in the pulmonary artery, corroborate the clinical picture, pointing to the diagnosis of PTE. The pulmonary hypertension in this case can be a consequence of mitral valve disease as well as the PTE.
The differential diagnosis for the image of a large thrombus located in the pulmonary artery is the pulmonary artery sarcoma, or metastatic squamous cell tumor. Of these, the most frequent diagnostic error of pulmonary embolism is the pulmonary artery sarcoma. It is a rare tumor of the cardiovascular system, originated from the dorsal area of the pulmonary artery trunk or the right or left pulmonary arteries. Due to the insidious growth and the rarity of presentation, it is often inappropriately treated as PTE3. However, this possibility becomes unlikely in this clinical case, due to failure in identifying the lesion on the pulmonary arteriography.
Another differential diagnosis, when evaluating the presence of atrial fibrillation with thromboembolic phenomena associated with the dielectric effect on ECG, is cardiac amyloidosis. However, it has low clinical suspicion when one analyzes the history of the disease, as well as the echocardiographic results and subsequent clinical course.
The use of thrombolytic therapy has consensual indication in this case, considering the clinical signs of thromboembolic event. It is classified as massive PTE when there is hemodynamic instability. The therapy rationale is the thrombus dissolution, decreasing the right ventricular overload and the pulmonary artery pressure levels. There are reports in the literature on the acute resolution of large thrombi, decreasing the mechanical obstruction of the right ventricle2. However, the migration of thrombus fragments distally can impair the success of thrombolysis and the expected outcome in relation to clinical evolution might not be attained. In fact, although indicated, there is no evidence of reduction in mortality with the use of thrombolytic agents in cases of massive PTE4.
The patient’s unfavorable evolution, although the arteriography did not disclose a thrombus in the pulmonary artery system, leads us to reflect on what else contributed to the poor outcome. Here we face some relevant points.
The first is the fact that the patient developed coagulopathy followed by evident bleeding. The normal coagulation at admission leads us to a diagnosis of acquired coagulopathy. The thrombolysis carried out in the PTE treatment certainly played a role in the etiology of the coagulation disorder. Moreover, as we will see below, the patient developed
e60

Anatomopathological Session
Lima et alAnatomopathological Session
Arq Bras Cardiol. 2014; 103(5):e57-e67
bacterial infection and there may have been disseminated intravascular coagulation secondary to sepsis. There are no reports of other documented bleeding, in addition to epistaxis, but the sharp decrease in hemoglobin levels associated with the incoagulable activated partial thromboplastin time (APTT) suggests active bleeding. Thus, hemorrhagic shock together with the clinical picture is among the possibilities and it might be related, in addition to the epistaxis, to the vascular access complication.
The second point is related to infection confirmed by blood cultures positive for Acinetobacter baumannii. A mixed shock (cardiogenic and septic) justifies the patient’s poor prognosis and her refractoriness to the measures that were undertaken. In recent years, there has been an increase in the resistance of Acinetobacter baumannii to broad-spectrum antibiotics. This has coincided with the increased incidence of sepsis by this agent5. Risk factors associated with sepsis by Acinetobacter are: prior use of broad-spectrum antibiotics, use of urinary catheters, mechanical ventilation and previous surgery. The mortality in these cases is around 38%.
The main factors of poor prognosis related to sepsis by Acinetobacter are the use of inadequate antibiotics and mechanical ventilation5. This patient had both factors.
The third point that draws attention to this case is the worsening of left ventricular function, as demonstrated in the patient’s last echocardiogram. Some possibilities can be suggested: myocardial depression in sepsis, rheumatic myocarditis and coronary thromboembolism. Rheumatic myocarditis results from an immune cellular process and therefore may occur without humoral manifestations, such as arthritis and chorea. It is usually associated with valvulitis and has a transitory character. It can be observed, in this case, that there is rheumatic disease activity, considering the early post-valvuloplasty dysfunction. Interleukin-4 appears to play a critical role in modulating local immune response due to its anti-inflammatory properties1.
Myocardial depression in sepsis can be found in approximately 40% of septic patients due to several factors, including reduction of coronary flow, myocardial edema, direct action of cytokines (IL-1, TNF-alpha) and of nitric oxide, leading to reduced levels of intracellular calcium6. Both myocarditis and myocardial depression in sepsis usually involve the myocardium as a whole, not focusing on specific territories. There are cases, however, when these conditions may mimic myocardial infarction. This patient had diffuse left ventricular hypokinesis, but more pronounced in the anterior and septal regions.
Based on this information, one can consider myocardial ischemia as a possible diagnosis. Coronary lesions, even non-obstructive ones, may lead to myocardial ischemia due to hypoperfusion secondary to shock, sometimes culminating in myocardial infarction (currently classified as myocardial infarction type 2)7. Another possibility is coronary embolism as a result of systemic thromboembolic phenomenon secondary to atrial fibrillation.
In fact, there have been reports of this kind in the literature, involving both the right coronary artery as well as the anterior descending artery. It is noteworthy that, despite evidence
of spontaneous contrast in the left atrium, the presence of thrombus in the left atrium was not demonstrated. However, this fact does not exclude the hypothesis. Another possibility is coronary embolism resulting from paradoxical embolism. The present of patent foramen ovale is frequent, being estimated at about 15-20% of normal individuals. Thrombus in the venous system, right-left shunt, increased pressure in the right system and systemic embolism are conditions that make the diagnosis likely8. The patient had at least three such conditions. The fact that the echocardiogram did not identify the presence of patent foramen ovale can be a result of low sensitivity to identify this condition. However, this patient had already undergone two heart surgeries with valve manipulation, making this diagnosis unlikely.
As a last point, we have kidney failure, which progressed during patient evolution, with hemodialysis being indicated. This clinical picture can be easily explained by the mixed shock. However, one cannot rule out a possible thromboembolic etiology.
The patient died due to refractory shock, not tolerating dialysis. Considering what was discussed, we suppose that the patient did not adequately carry out the secondary prophylaxis of rheumatic fever, since the evolution of post-valvuloplasty. She had decompensated heart failure, related to medication discontinuation and pulmonary thromboembolism. She had an episode of massive PTE during hospitalization, which, despite adequate therapy, developed unfavorably. This evolution is due to sepsis by Acinetobacter and myocardial dysfunction, which may be related to sepsis and / or possibly acute myocardial infarction by coronary thromboembolism (Dr. Eduardo Gomes Lima, Dr. Ricardo D’Oliveira Vieira, Dr. Paula Bombonati).
Diagnostic hypothesis: Chronic rheumatic mitral valve disease, post-valvuloplasty mitral dysfunction, pulmonary thromboembolism and mixed shock (cardiogenic, septic) (Dr. Eduardo Gomes Lima, Dr. Ricardo D’Oliveira Vieira, Dr. Paula Bombonati)
NecropsyThe heart weighed 630 g (normal weight for women is
between 250-300 g), with mild hypertrophy and moderate left atrium dilation, with marked thickening of the endocardium (Figure 3). Seen from the atrial side, the mitral valve had the “fish mouth” aspect with reduced opening, commissural fusion and severe thickening of the cusps (Figure 3). There was also mild multifocal calcification and evidence of previous valve surgery as shown by the presence of surgical stitches in almost the entire valve circumference, largely included in the valve tissue and surroundings (signs consistent with prior valvuloplasty - Figure 3). From the ventricular side, the valve apparatus showed marked deformity and shortening, represented by cords exhibiting severe thickening, fusion and retraction (Figure 4).
At handling and maneuvering with water flow, valve mobility and cusp coaptation were significantly impaired, suggesting double valve lesion with stenosis greater than regurgitation as functional alterations. In the aortic valve, the semilunar showed diffuse thickening and mild collapse,
e61
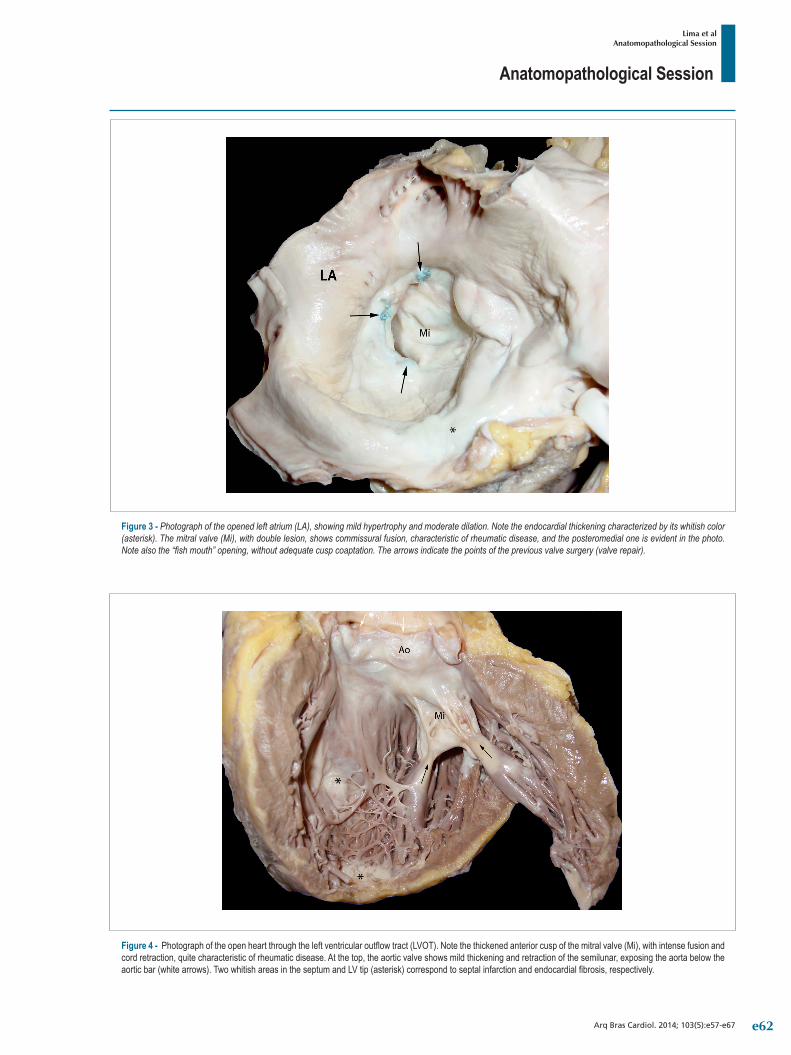
Anatomopathological Session
Lima et alAnatomopathological Session
Arq Bras Cardiol. 2014; 103(5):e57-e67
Figure 4 - Photograph of the open heart through the left ventricular outflow tract (LVOT). Note the thickened anterior cusp of the mitral valve (Mi), with intense fusion and cord retraction, quite characteristic of rheumatic disease. At the top, the aortic valve shows mild thickening and retraction of the semilunar, exposing the aorta below the aortic bar (white arrows). Two whitish areas in the septum and LV tip (asterisk) correspond to septal infarction and endocardial fibrosis, respectively.
Figure 3 - Photograph of the opened left atrium (LA), showing mild hypertrophy and moderate dilation. Note the endocardial thickening characterized by its whitish color (asterisk). The mitral valve (Mi), with double lesion, shows commissural fusion, characteristic of rheumatic disease, and the posteromedial one is evident in the photo. Note also the “fish mouth” opening, without adequate cusp coaptation. The arrows indicate the points of the previous valve surgery (valve repair).
e62
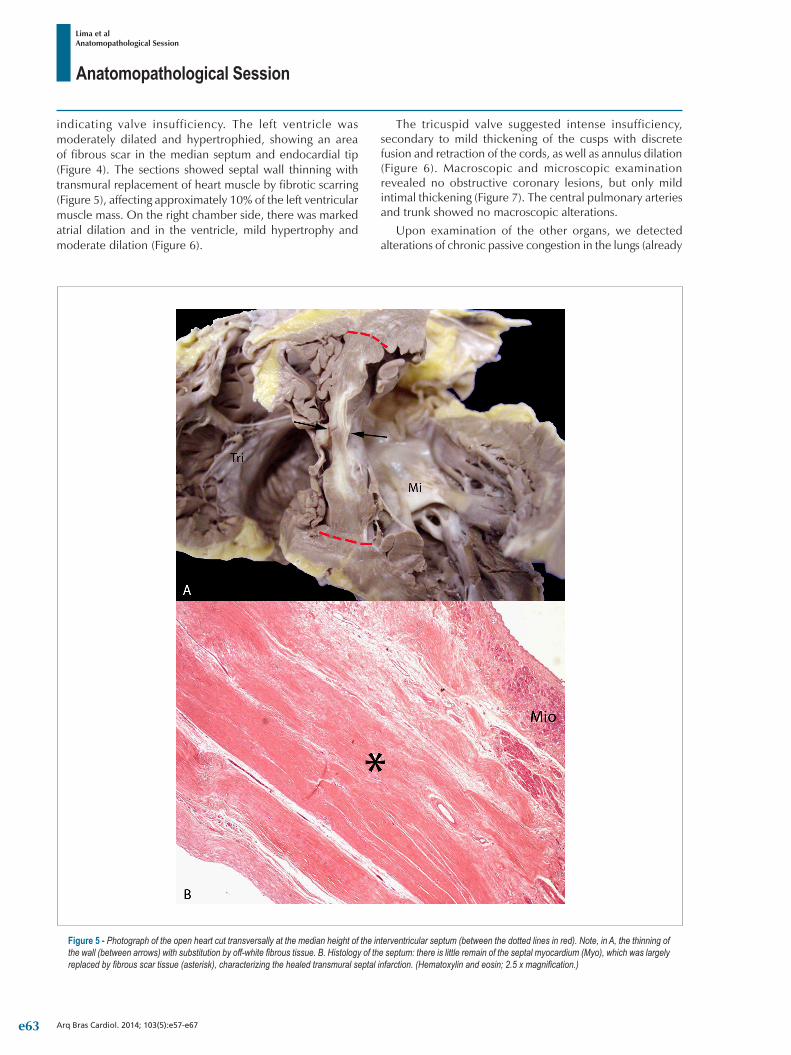
Anatomopathological Session
Lima et alAnatomopathological Session
Arq Bras Cardiol. 2014; 103(5):e57-e67
Figure 5 - Photograph of the open heart cut transversally at the median height of the interventricular septum (between the dotted lines in red). Note, in A, the thinning of the wall (between arrows) with substitution by off-white fibrous tissue. B. Histology of the septum: there is little remain of the septal myocardium (Myo), which was largely replaced by fibrous scar tissue (asterisk), characterizing the healed transmural septal infarction. (Hematoxylin and eosin; 2.5 x magnification.)
indicating valve insufficiency. The left ventricle was moderately dilated and hypertrophied, showing an area of fibrous scar in the median septum and endocardial tip (Figure 4). The sections showed septal wall thinning with transmural replacement of heart muscle by fibrotic scarring (Figure 5), affecting approximately 10% of the left ventricular muscle mass. On the right chamber side, there was marked atrial dilation and in the ventricle, mild hypertrophy and moderate dilation (Figure 6).
The tricuspid valve suggested intense insufficiency, secondary to mild thickening of the cusps with discrete fusion and retraction of the cords, as well as annulus dilation (Figure 6). Macroscopic and microscopic examination revealed no obstructive coronary lesions, but only mild intimal thickening (Figure 7). The central pulmonary arteries and trunk showed no macroscopic alterations.
Upon examination of the other organs, we detected alterations of chronic passive congestion in the lungs (already
e63

Anatomopathological Session
Lima et alAnatomopathological Session
Arq Bras Cardiol. 2014; 103(5):e57-e67
showing passive pulmonary hypertension) and liver, as morphological substrate of overall congestive heart failure associated with valvular heart disease. The right lung showed extensive lobar area with hardening and hemorrhage, macroscopically indicating a heart attack or “red-gray hepatization”, with lobar pneumonia being subsequently characterized through histology. This infectious picture was also associated with the presence of acute pyelonephritis, represented by multiple cylinders of polymorphonuclear neutrophils in renal pyramids, which also infiltrated the interstitium. The spleen was enlarged (250 g, normal weight
is approximately 150 g) at the expense of the red pulp, showing an acute splenitis pattern (Figure 8). Morphological changes related to shock, such as acute renal tubular necrosis, hepatic centrilobular necrosis and cerebral edema with herniation of the cerebellar tonsils were also observed and thus, septic shock was considered as the immediate cause of death. (Dr. Jussara Bianchi Castelli)
Anatomopathological diagnoses: Chronic rheumatic mitral-aortic-tricuspid valve disease; valvular heart disease
Figure 6 - Photograph of the open heart through the right ventricle (RV) inflow tract. Note in A, dilation of the cavities of the right atrium (RA) and right ventricle (RV), the latter also showing hypertrophy. The tricuspid valve (Tri) shows intrinsic insufficiency (by focal thickening and shortening of the cusp and cords) and also by secondary annulus dilatation. B. Detail of the tricuspid valve where the arrows indicate the alterations described.
e64
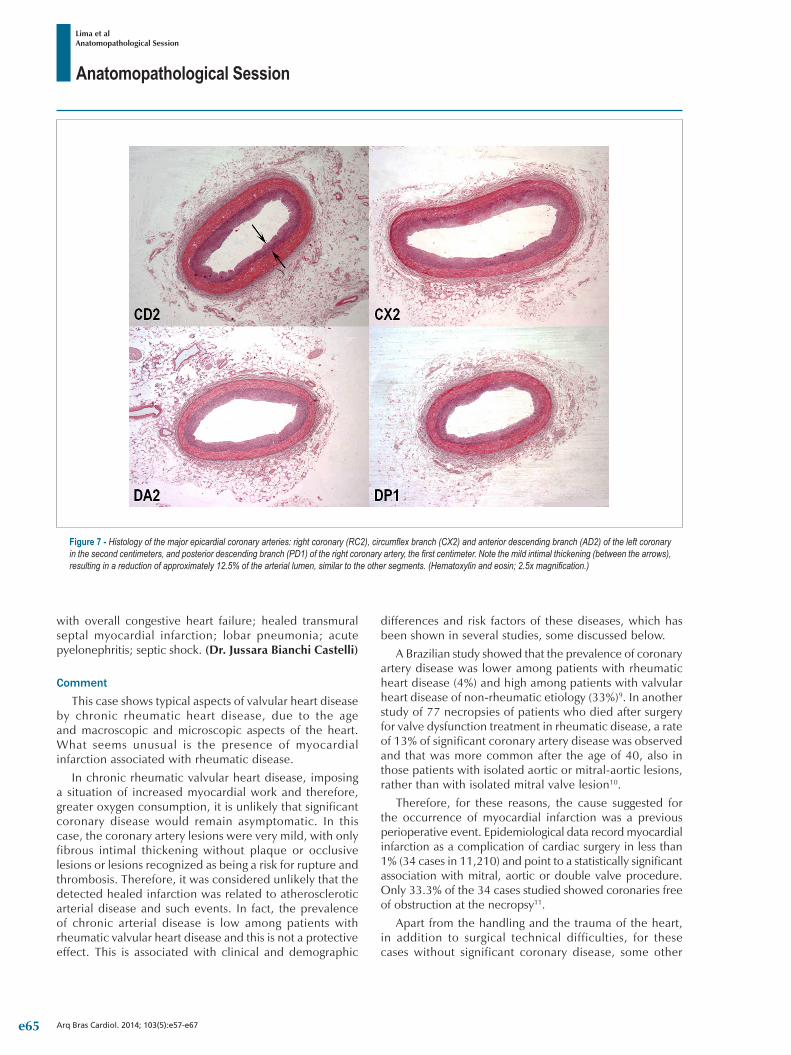
Anatomopathological Session
Lima et alAnatomopathological Session
Arq Bras Cardiol. 2014; 103(5):e57-e67
Figure 7 - Histology of the major epicardial coronary arteries: right coronary (RC2), circumflex branch (CX2) and anterior descending branch (AD2) of the left coronary in the second centimeters, and posterior descending branch (PD1) of the right coronary artery, the first centimeter. Note the mild intimal thickening (between the arrows), resulting in a reduction of approximately 12.5% of the arterial lumen, similar to the other segments. (Hematoxylin and eosin; 2.5x magnification.)
with overall congestive heart failure; healed transmural septal myocardial infarction; lobar pneumonia; acute pyelonephritis; septic shock. (Dr. Jussara Bianchi Castelli)
CommentThis case shows typical aspects of valvular heart disease
by chronic rheumatic heart disease, due to the age and macroscopic and microscopic aspects of the heart. What seems unusual is the presence of myocardial infarction associated with rheumatic disease.
In chronic rheumatic valvular heart disease, imposing a situation of increased myocardial work and therefore, greater oxygen consumption, it is unlikely that significant coronary disease would remain asymptomatic. In this case, the coronary artery lesions were very mild, with only fibrous intimal thickening without plaque or occlusive lesions or lesions recognized as being a risk for rupture and thrombosis. Therefore, it was considered unlikely that the detected healed infarction was related to atherosclerotic arterial disease and such events. In fact, the prevalence of chronic arterial disease is low among patients with rheumatic valvular heart disease and this is not a protective effect. This is associated with clinical and demographic
differences and risk factors of these diseases, which has been shown in several studies, some discussed below.
A Brazilian study showed that the prevalence of coronary artery disease was lower among patients with rheumatic heart disease (4%) and high among patients with valvular heart disease of non-rheumatic etiology (33%)9. In another study of 77 necropsies of patients who died after surgery for valve dysfunction treatment in rheumatic disease, a rate of 13% of significant coronary artery disease was observed and that was more common after the age of 40, also in those patients with isolated aortic or mitral-aortic lesions, rather than with isolated mitral valve lesion10.
Therefore, for these reasons, the cause suggested for the occurrence of myocardial infarction was a previous perioperative event. Epidemiological data record myocardial infarction as a complication of cardiac surgery in less than 1% (34 cases in 11,210) and point to a statistically significant association with mitral, aortic or double valve procedure. Only 33.3% of the 34 cases studied showed coronaries free of obstruction at the necropsy11.
Apart from the handling and the trauma of the heart, in addition to surgical technical difficulties, for these cases without significant coronary disease, some other
e65

Anatomopathological Session
Lima et alAnatomopathological Session
Arq Bras Cardiol. 2014; 103(5):e57-e67
Figure 8 - Histology of infectious alterations and secondary to septic shock observed in major organs. A. Lobar pneumonia characterized by dense alveolar filling with neutrophilic infiltration (asterisk). B. Detail of A at higher magnifications: Note the cellular composition, exclusively neutrophilic (asterisk) and the interalveolar septum (arrow). C. Acute pyelonephritis: kidney showing tubules filled with neutrophilic infiltration (arrow). D. Spleen showing acute splenitis with increased red pulp (asterisk). E. Liver with recent necrosis of zone 3 (arrow) observed in large areas. F. Rim, in another region, showing acute tubular necrosis: see more intense red color of the tubular lining cells (arrow). (Hematoxylin and eosin; magnification 2.5x, 40x, 20x, 10x, 5x and 40x, respectively.)
etiopathological mechanisms are considered as a cause of perioperative infarctions in cardiac surgery for valve replacement, such as coronary embolization (personal communication: e.g., we observed once, in a necropsy, calcium emboli to the coronaries in a case of mitral valve replacement that presented with severe dystrophic
calcification), coronary gas embolism, coronary vasospasm, topic hypothermia or inappropriate cardioplegia, among others. The prognosis of perioperative myocardial infarction is not necessarily bad, but its occurrence should warrant appropriate measures and prevention in surgical valve replacement6,12. (Dr. Jussara Bianchi Castelli)
e66

Anatomopathological Session
Lima et alAnatomopathological Session
Arq Bras Cardiol. 2014; 103(5):e57-e67
1. Grinberg M, Sampaio RO. Doença valvar. São Paulo: Manole; 2006.
2. Goldhaber SZ, Haire WD, Feldstein ML, Miller M, Toltzis R, Smith JL, et al. Alteplase versus heparin in acute pulmonary embolism: randomised trial assessing right-ventricular function and pulmonary perfusion. Lancet. 1993;341(8844):507-11.
3. Matto A, Fedullo PF, Kapelanski D, Iiowate JS. Pulmonary artery sarcoma: a case report of surgical cure and 5-year follow-up. Chest. 2002;122(2):745-7.
4. Almoosa K. Is thrombolitic therapy effective for pulmonary embolism? Am Fam Physician. 2002;65(6):1097-102.
5. Gomez J, Simarro E, Baños V, Requena L, Ruiz J, Garcia F, et al. Six year prospective study of risk and prognostic factors in patients with nosocomial sepsis caused by Acinetobacter baumannii. Eur J Clin Microbiol Infect Dis. 1999;18(5):358-61.
6. Okamura Y, Takeuchi Y, Gomi A, Nagashima M, Mori H, Hattori J. [Clinical evaluation of perioperative myocardial infarction as a complication of valve replacement]. Kyobu Geka. 1989;42(12):1012-5.
7. Thygesen K, Alpert JS, White HD, Jaffe AS, Apple FS, Galvani M, et al; Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction. Circulation. 2007;116(22):2634-53.
8. Ward R, Jones D, Haponik EF. Paradoxical embolism: an underrecognized problem. Chest. 1995;108(2):549-58.
9. Kruczan DD, Silva NA, Pereira BB, Romão VA, Correa Filho WB, Morales FE. Coronary artery disease in patients with rheumatic and non-rheumatic valvular heart disease treated at a public hospital in Rio de Janeiro. Arq Bras Cardiol. 2008;90(3):197-203.
10. Coleman EH, Soloff LA. Incidence of significant coronary artery disease in rheumatic valvular heart disease. Am J Cardiol. 1970;25(4):401-4.
11. Rotberg T, Macías R, Correa-Suárez R, Luna P, Malo R. [Trans and postoperative myocardial infarct in heart surgery]. Arch Inst Cardiol Mex. 1976;46(1):82-97.
12. Laurindo FR, Grinberg M, Campos de Assis RV, Jatene AD, Pileggi F. Perioperative acute myocardial infarction after valve replacement. Am J Cardiol. 1987;59(6):639-42.
References
e67

Case Report
Multiple Benefits of Rehabilitation in a Patient with Heart and Renal FailureCarlos Alberto Cordeiro Hossri1, Fernando José Pinho Queiroga Júnior1, Vitor Oliveira Carvalho1,2, Carlos Roberto Ribeiro Carvalho1,2, Andre Luis Pereira Albuquerque2
Hospital do Coração (HCor) Associação do Sanatório Sírio1; Instituto do Coração da Faculdade de Medicina da Universidade de São Paulo (InCOR-FMUSP)2 São Paulo, SP – Brazil
Mailing Address: Carlos Alberto Cordeiro Hossri •Rua Afonso De Freitas, Paraíso. Postal Code 040.06-052, São Paulo, RJ – Brazil.Email: [email protected]; [email protected] received October 9, 2013; revised December 28, 2013; accepted February 18, 2014.
KeywordsHeart Failure / rehabilitation; Exercise; Renal Insufficiency
/ rehabilitation; Exercise Therapy.
DOI: 10.5935/abc.20140127
IntroductionHeart failure is associated with high mortality and
significantly reduced exercise capacity in many cases, despite medical treatment. Patients may present also renal failure, one of the most important comorbidities, which contributes even more to a poor prognosis, especially in patients who are already attending dialysis sessions1. Reduction of renal function occurs in approximately 25% of patients with chronic heart failure, regardless the severity of left ventricular dysfunction1.
Exercise training is formally recommended as a safe non-pharmacological intervention in stable heart failure2,3. Nevertheless, many patients in severe stage are extremely symptomatic and consider themselves as incapable to attend an exerce training program. The association of heart failure and renal failure in use of continuous ambulatory peritoneal dialysis makes this attendance even more complicated. The physicians also are insecure and resistant to recommend cardiopulmonary rehabilitation for a patient with such important impairment.
This case report aims at describing the clinical and physiological effects of an exercising program in a severe heart failure patient with renal failure in peritoneal dialysis.
Patient is a 54-year-old male, with heart failure secondary to idiopathic etiology, NYHA functional class III-IV for 8 years with implantable defibrillator and cardiac resynchronization in the last 2 years. The electrocardiogram before the defibrillator showed left bundle branch block. He also had suffered from chronic renal failure for the last 6 years, in continuous ambulatory peritoneal dialysis (CAPD) for the last 3 years undergoing 21 sessions/week. He was referred to our hospital for exercise training because his pharmacological therapy has already been optimized 2 years before: (Furosemide 40 mg/d, Spironolactone 25 mg/d, Angiotensin Receptor Blocker 80 mg/d and β-blockers Carvedilol 50 mg/d) and he persisted being extremely limited in his daily activities.
Before and after rehabilitation, were assessed: left ventricular ejection fraction (LVEF, Simpsom’s method), maximal and
submaximal cardiopulmonary exercise tests (CPET), quality of life (SF-36 questionnaire) and urea/creatinine levels in the blood. The maximal CPET, with incremental protocol on treadmill, was used not only to obtain the exercise capacity but also to define the threshold of exercise training during the rehabilitation. Still in the maximal CPET, it was evaluated the VE/VCO2 slope during incremental phase and the drop of the heart rate in the first minute of recovery phase, which was used to investigate the autonomic system4.
The submaximal CPET at 80% of maximal exercise capacity was applied to measure the endurance tolerance and the changes in different systems (cardiovascular, ventilatory and peripheral muscles) pre and post intervention. In order to evaluate the efficiency of oxidative metabolism in the peripheral muscles after exercise program, we used the time constant of oxygen consumption to achieve the steady state of 63% peak VO2 (kinetics analysis) in both endurance tests5.
Exercise rehabilitation sessions (45 min, 4 times/week for 8 weeks) were always supervised. Aerobic exercises (20-30 min) were performed in treadmill and cycle ergometer at anaerobic threshold achieved in maximal CPT (VO2 = 4.7 ml.kg-1.min-1, 42% of VO2max), and resistance exercises for upper and lower limbs at 40% of maximal voluntary contraction, 3 series of 10 repetitions with 1 min of rest for each series6,7. As this patient has a severe heart failure, the maximal voluntary contraction was estimated using 12 to 15 voluntary repetitions reaching moderate degree of fatigue (11 to 13 on the original Borg perceived exertion scale), which represents approximately 30 to 40% of one repetition maximum (1-RM) for the upper limbs and 40 to 50% to the lower limbs being performed6.
The patient was monitored by a multichannel telemetry system during all exercises to verify possible arrhythmias.
DiscussionAfter 2 months of rehabilitation (Table 1), the patient
showed an important improvement in maximal exercise performance (distance and peak VO2), ventilatory efficiency (VE/VCO2 slope), increase of the systolic blood pressure delta, and higher LVEF. The renal function also improved substantially, decreasing the dialysis sessions from 21 to 4 per week. The patient became less symptomatic (NYHA II), the quality of life was substantially benefited in all domains of SF-36 and he returned to his job (office work).
The enhancement on exercise tolerance and symptoms is likely a consequence of the benefits over the body systems, taking into account mainly the cardiovascular, skeletal muscle, ventilatory and renal. In this case, exercise training
e68

Case Report
Hossri et al.Benefits of exercise for heart and renal failure
Arq Bras Cardiol. 2014; 103(5):e68-e71
Table 1 – Exercise, metabolic and hemodynamic variables obtained during maximal incremental test before and after cardiopulmonary rehabilitation
Before After
Incremental test
Time (min) 5.9 9.9
Distance (m) 330 660
Peak VO2 (ml/kg/min) 10.2 13.0
VE/VCO2 Slope 51 46
RER at peak 1.37 1.28
VO2 AT (ml.kg-1.min-1) 4.7 6.7
Peak O2 Pulse (ml.kg.-1min-1/bpm) 6.6 7.0
Peak Heart Rate (bpm) 94 123
Heart Rate Recovery 1stmin (bpm) 6 13
Delta Systolic BP (mmHg) 9 35
Clinical and functional responses
NYHA functional class III II
LVEF (%) 27 33
Urea (mg/dl) 188 75
Creatinine (mg/dl) 3.88 1.7
Dialysis per week 21 4
Physical Component (SF-36) 40 78
Mental Component (SF-36) 50 85
VO2: oxygen consumption; AT: anaerobic threshold; NYHA: New York Heart Association; LVEF: left ventricle ejection fraction. RER: respiratory exchange ratio; O2: pulse oxygen pulse
resulted in an augment on cardiac performance reflected even at rest by the higher LVEF. The reduction of minute ventilation (Figure 1b, lower VE/VCO2 slope), an index of greater ventilatory efficiency, is also a benefit of greater cardiac output since the anaerobic threshold was achieved later post rehabilitation, attenuating the ventilatory response.
Other afferent stimulus to the respiratory center is the CO2 produced in the skeletal muscles. Considering the endurance tests, after intervention, the patient was able to tolerate much more exercise with a significant lower CO2 production from the peripheral muscles (Figure 1a). This phenomenon reflects a better metabolic efficiency after training. It is already known the aerobic rehabilitation has relevant implications on muscle metabolism, mainly due to higher capillarization (higher oxygen output), increase of mitochondrial density and higher proportion of oxidative fibers3,7. The analysis of oxygen kinetics shows the behavior of muscle oxidative metabolism to exercise, with severe patients presenting a delay in this variable. The current case demonstrates an improvement on O2 kinetics, with a shorter time to achieve the steady state after rehabilitation (Figure 1d). Thus, in this case there was a clear gain in the peripheral muscles, considering that their energetic metabolism became more efficient after rehabilitation.
Not only was the lower ventilation relevant for this patient, but also the pattern of breathing (Figure 1b and 1c). Before the rehabilitation, in the incremental cardiopulmonary test there was a marked pattern of periodic ventilation during the phase of increment and also in the recovery. After the program, the periodic ventilation was not abolished but decreased significantly in the increment and recovery phases of cardiopulmonary test. Although the mechanisms of periodic breathing have not been fully elucidated yet, it is present exactly in patients with severe heart failure and, of note, has prognostic implications2,3. The improvement found in this patient was certainly related to the improved cardiac function post rehabilitation.
Finally, there was a benefit also in the renal failuresince the frequency of dialysis sessions decreased from 21 to 4/week. This represents an interesting effect of cardiopulmonary rehabilitation and is probably related to better balance in the autonomic system, likely more related to renin-angiotensin system. Previous studies have described a lower activity of sympathetic drive after exercise program, which is in agreement with the faster recovery of heart rate after incremental test, suggesting lower sympathetic activation post rehabilitation in this patient8. In addition, the reduction in the renin-angiotensin-aldosterone system is also a result of exercise program, leading to a higher blood flow into renal arteries and, in this way, a better filtration9,10.
e69
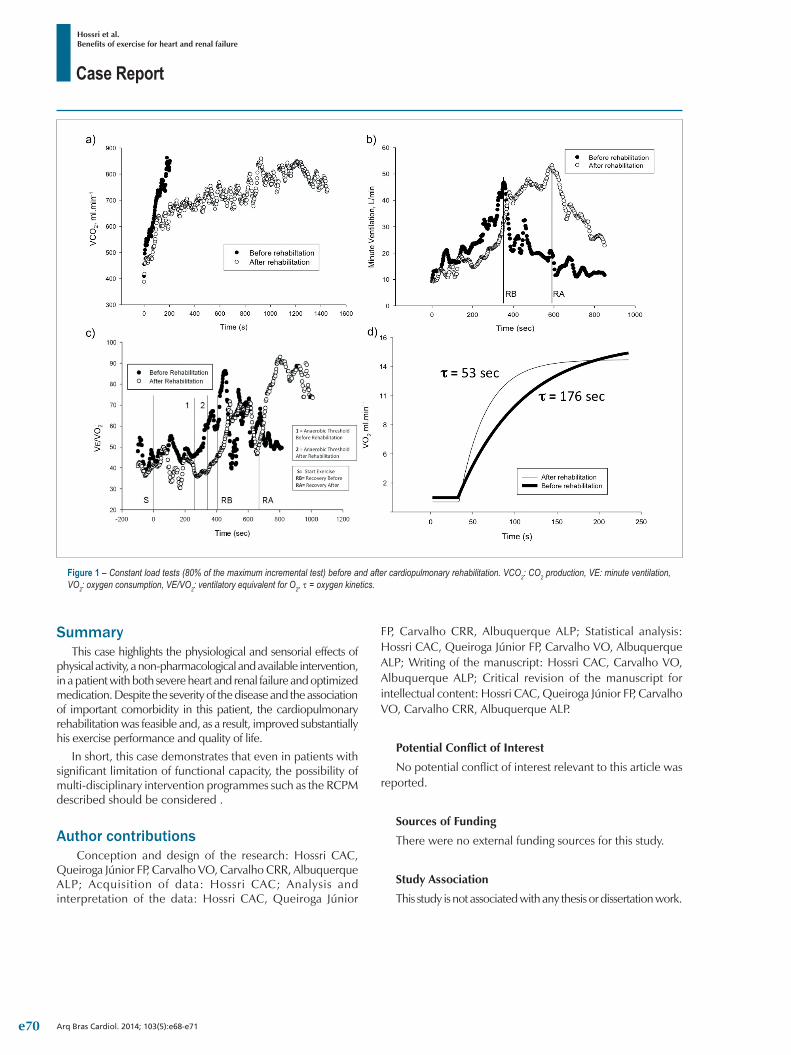
Case Report
Hossri et al.Benefits of exercise for heart and renal failure
Arq Bras Cardiol. 2014; 103(5):e68-e71
Figure 1 – Constant load tests (80% of the maximum incremental test) before and after cardiopulmonary rehabilitation. VCO2: CO2 production, VE: minute ventilation, VO2: oxygen consumption, VE/VO2: ventilatory equivalent for O2, τ = oxygen kinetics.
SummaryThis case highlights the physiological and sensorial effects of
physical activity, a non-pharmacological and available intervention, in a patient with both severe heart and renal failure and optimized medication. Despite the severity of the disease and the association of important comorbidity in this patient, the cardiopulmonary rehabilitation was feasible and, as a result, improved substantially his exercise performance and quality of life.
In short, this case demonstrates that even in patients with significant limitation of functional capacity, the possibility of multi-disciplinary intervention programmes such as the RCPM described should be considered .
Author contributions Conception and design of the research: Hossri CAC,
Queiroga Júnior FP, Carvalho VO, Carvalho CRR, Albuquerque ALP; Acquisition of data: Hossri CAC; Analysis and interpretation of the data: Hossri CAC, Queiroga Júnior
FP, Carvalho CRR, Albuquerque ALP; Statistical analysis: Hossri CAC, Queiroga Júnior FP, Carvalho VO, Albuquerque ALP; Writing of the manuscript: Hossri CAC, Carvalho VO, Albuquerque ALP; Critical revision of the manuscript for intellectual content: Hossri CAC, Queiroga Júnior FP, Carvalho VO, Carvalho CRR, Albuquerque ALP.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This study is not associated with any thesis or dissertation work.
e70

Case Report
Hossri et al.Benefits of exercise for heart and renal failure
Arq Bras Cardiol. 2014; 103(5):e68-e71
1. Harnett JD, Foley RN, Kent GM, Barre PE, Murray D, Parfrey PS. Congestive heart failure in dialysis patients: prevalence, incidence, prognosis and risk factors. Kidney Int. 1995;47(3):884-90.
2. Piña IL, Apstein CS, Balady GJ, Belardinelli R, Chaitman BR, Duscha BD, et al; American Heart Association Committee on exercise, rehabilitation, and prevention. Exercise and heart failure: a statement from the American Heart Association Committee on exercise, rehabilitation, and prevention. Circulation. 2003;107(8):1210-25.
3. Leite JJ, Mansur AJ, de Freitas HG, Chizola PR, Bocchi EA, Terra-Filho M, et al. Periodic breathing during incremental exercise predicts mortality in patients with chronic heart failure evaluated for cardiac transplantation. J Am Coll Cardiol. 2003;41(12):2175-81.
4. Cole CR, Foody JM, Blackstone EH, Lauer MS. Heart rate recovery after submaximal exercise testing as a predictor of mortality in a cardiovascular healthy cohort. Ann Intern Med. 2000;132 (7):552-5.
5. Koike A, Yajima T, Adachi H, Shimizu N, Kano H, Sugimoto K, et al. Evaluation of exercise capacity using submaximal exercise at a
constant work rate in patients with cardiovascular disease. Circulation. 1995;91(6):1719-24.
6. Carvalho VO, Mezzani A. Aerobic exercise training intensity in patients with chronic heart failure: principles of assessment and prescription. Eur J Cardiovasc Prev Rehabil. 2011;18(1):5-14.
7. Carvalho VO, Guimarães GV. An overall view of physical exercise prescription and training monitoring for heart failure patients. Cardiol J. 2010;17(6):644-9.
8. Yang HT, Prior BM, Lloyd PG, Taylor JC, Li Z, Laughlin MH, et al. Training induced vascular adaptations to ischemic muscle. J Physiol Pharmacol. 2008;59 Suppl 7:57-70.
9. Zucker IH, Patel KP, Schultz HD, Li YF, Wang W, Pliquett RU. Exercise training and sympathetic regulation in experimental heart failure. Exerc Sport Sci Rev. 2004;32(3):107-11. Erratum in Exerc Sport Sci Rev. 2004;32(4):191.
10. Wan W, Powers AS, Li J, Ji L, Erikson JM, Zhang JQ. Effect of post-myocardial infarction exercise training on the renin-angiotensin-aldosterone system and cardiac function. Am J Med Sci. 2007;334(4):265-73.
References
e71
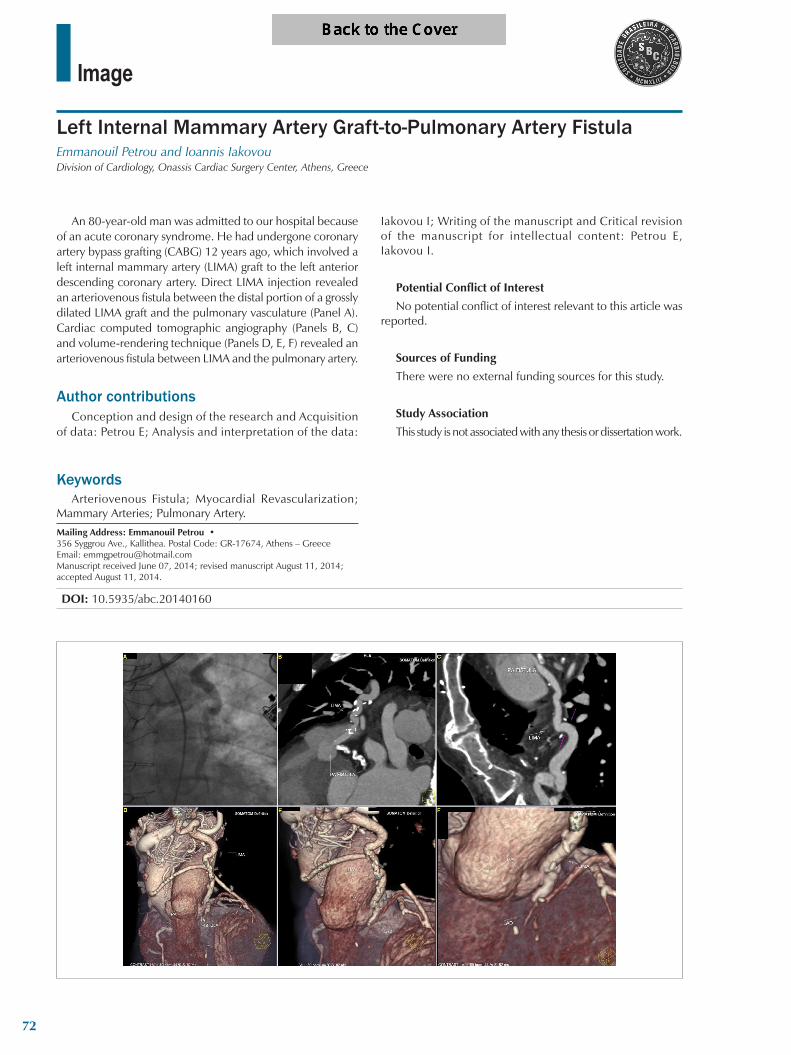
Image
Left Internal Mammary Artery Graft-to-Pulmonary Artery FistulaEmmanouil Petrou and Ioannis IakovouDivision of Cardiology, Onassis Cardiac Surgery Center, Athens, Greece
Mailing Address: Emmanouil Petrou •356 Syggrou Ave., Kallithea. Postal Code: GR-17674, Athens – GreeceEmail: [email protected] received June 07, 2014; revised manuscript August 11, 2014; accepted August 11, 2014.
KeywordsArteriovenous Fistula; Myocardial Revascularization;
Mammary Arteries; Pulmonary Artery.
DOI: 10.5935/abc.20140160
An 80-year-old man was admitted to our hospital because of an acute coronary syndrome. He had undergone coronary artery bypass grafting (CABG) 12 years ago, which involved a left internal mammary artery (LIMA) graft to the left anterior descending coronary artery. Direct LIMA injection revealed an arteriovenous fistula between the distal portion of a grossly dilated LIMA graft and the pulmonary vasculature (Panel A). Cardiac computed tomographic angiography (Panels B, C) and volume-rendering technique (Panels D, E, F) revealed an arteriovenous fistula between LIMA and the pulmonary artery.
Author contributionsConception and design of the research and Acquisition
of data: Petrou E; Analysis and interpretation of the data:
Iakovou I; Writing of the manuscript and Critical revision of the manuscript for intellectual content: Petrou E, Iakovou I.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This study is not associated with any thesis or dissertation work.
72