2011 johns hopkins bloomberg school of public health special populations: update stephen a. tamplin,...
TRANSCRIPT

2011 Johns Hopkins Bloomberg School of Public Health
Special Populations: UpdateSpecial Populations: Update
Stephen A. Tamplin, MSEDepartment of Health, Behavior and SocietyInstitute for Global Tobacco Control
2011 Johns Hopkins Bloomberg School of Public Health
Objective
To highlight new or recent developments related to tobacco control in “special populations” Tobacco and poverty Tobacco and youth Women and tobacco The role of nurses in tobacco control
2

2011 Johns Hopkins Bloomberg School of Public Health
Messages from Previous Lectures—Tobacco and Poverty
84% of smokers live in developing and transitional economy countries
The poor smoke the most and bear most of the economic and disease burden of tobacco use
Smoking prevalence among men is higher in low- and middle-income countries (about 50%)
Tobacco contributes to poverty at the individual and household levels: Opportunity cost Lost earnings due to
higher risk of illness Risks of tobacco
farming
3
2011 Johns Hopkins Bloomberg School of Public Health
Messages from Previous Lectures—Tobacco and Poverty
Tobacco contributes to poverty at the national level: High health care costs Lost productivity Loss of foreign
exchange Smuggling Environmental
degradation
Breaking the tobacco-poverty relationship requires consideration of: The local context Relationships and
partnerships Local champions The need to situate
interventions in the social development climate
Timing
4

2011 Johns Hopkins Bloomberg School of Public Health
New Knowledge Regarding Tobacco and Poverty
Meta-analysis involved the review of 9,500 references, of which 765 were included
Overall objective was to assess the association between income level and tobacco consumption, tobacco expenditures and morbidity, and mortality attributed to tobacco
Compared high-income groups with low-income groups on four factors: Prevalence of tobacco use Quantity of tobacco consumed Incidence of disease and death attributed to
tobacco Household expenditures on tobacco
5
Source: Ciapponi, A. (2011).

2011 Johns Hopkins Bloomberg School of Public Health
New Knowledge Regarding Tobacco and Poverty
The major conclusion: there is an inverse relationship between income level and tobacco use prevalence (particularly in the last two decades) and its related consequences Smoking prevalence: low-income people (both
genders) smoke more than high-income people Tobacco-attributable deaths and diseases: “…
statistically significant higher risk at decreasing income strata.”
Tobacco spending related to total expenditures: “… an inverse relationship … between income level and the proportion of tobacco spending related to total expenditures.”
6
Source: Ciapponi, A. (2011).
2011 Johns Hopkins Bloomberg School of Public Health
New Knowledge Regarding Tobacco and Poverty
Causes for disparity are “… still under discussion …” but several factors are alluded to: Relative deprivation inside societies Tobacco as a marker of social status Tobacco price structures
Greater efforts to reduce tobacco use among the poor are needed
The association between tobacco and poverty should be repeatedly assessed as implementation of the WHO’s FCTC is likely to modify the current situation
7
Source: Ciapponi, A. (2011).

2011 Johns Hopkins Bloomberg School of Public Health
Messages from Previous Lectures—Tobacco and Youth
The majority of all long-term tobacco users start as youth Nearly one-fourth have their first cigarette before age
10
There is no single image of youth tobacco use
“Tobacco is a communicated disease … through advertising and sponsorship ….” (WHO, 2000)
The tobacco industry targets youth by selling “coolness,” “independence,” and “lifestyle”
8
2011 Johns Hopkins Bloomberg School of Public Health
Messages from Previous Lectures—Tobacco and Youth
We know how to reduce youth tobacco use: Smoke-free laws Increasing taxes and retail prices Strong sustained public education campaigns Powerful graphic health warnings Curtailing tobacco marketing Expanding access to cessation Involving the community and health care professionals
9

2011 Johns Hopkins Bloomberg School of Public Health
New Knowledge Regarding Tobacco and Youth
The Global Tobacco Surveillance System Atlas (2009), Global Youth Tobacco Survey (GYTS), 1999-2008 12% of boys and nearly 7% of girls currently smoke
cigarettes Susceptibility to initiate cigarette smoking is higher than
current smoking rates in most regions 19% said they were susceptible to start smoking
within the next year 12% of boys and 8% of girls use other tobacco (e.g., pipes,
water pipes, cigars, smokeless tobacco, and bidis) besides cigarettes
In relation to boys, 8 of 165 countries surveyed reported a prevalence ≥ 30%
In relation to girls, 6 of the surveyed countries reported a prevalence ≥ 30%
10
Source: U.S. Centers for Disease Control and Prevention. GYTS Data. (2008).
2011 Johns Hopkins Bloomberg School of Public Health
New Knowledge Regarding Tobacco and Youth
The Global Tobacco Surveillance System Atlas (2009), Global Youth Tobacco Survey (GYTS), 1999-2008 (surveys of students aged 13-15 years): 55% of the students surveyed reported exposure to
secondhand smoke in public places during the previous week
Fewer than 5% of people are protected by comprehensive smoke-free laws
4 in 10 youth were exposed to secondhand smoke in their homes with 43% having at least one smoking parent
8 in 10 students favor a ban on smoking in public places and 69% of current youth smokers would like to quit
11
Source: U.S. Centers for Disease Control and Prevention. GYTS Data. (2008).

2011 Johns Hopkins Bloomberg School of Public Health
Messages from Previous Lectures—Women and Tobacco
12% of women smoke (22% in high-income countries; 9% in low- and middle-income countries) By 2025, about 20% of women will smoke
Smoking has negative effects on nearly every system of a woman’s body
Tobacco farming and processing exploit the labor of women and girls
The tobacco industry targets women by selling “coolness,” “independence,” “sex appeal,” and “lifestyle”
12

2011 Johns Hopkins Bloomberg School of Public Health
Messages from Previous Lectures—Women and Tobacco
13
Policy recommendations
Ratify and implement the FCTC
Design empowering messages and ads for improving women’s health
Promote tobacco control policies that address social and economic issues
Monitor women’s and men’s tobacco use rates
Conduct further research on the health effects of tobacco use on women
Build capacity and engage women and girls in conducting tobacco control research
Program recommendations
Implement gender- and age-specific tobacco control programs
Provide information on occupational health and safety for women and girls
Engage women in designing and delivering programs

2011 Johns Hopkins Bloomberg School of Public Health
New Knowledge Regarding Women and Tobacco
Women comprise about 20% of the world’s 1+ billion smokers
In half the countries surveyed by the Global Youth Tobacco Survey, there is no difference in rates of youth smoking based on gender
Smoking is responsible for 12% of male deaths and 6% of female deaths in the world
In a recent retrospective study (Oberg, M. et. al., 2011) of the world burden of disease from exposure to secondhand smoke, the authors concluded that women comprised almost 50% of the deaths attributable to secondhand smoke in 2004
14
Source: U.S. Centers for Disease Control and Prevention. GYTS Data. (2008); Oberg et. al., (2011).
2011 Johns Hopkins Bloomberg School of Public Health
New Knowledge Regarding Women and Tobacco
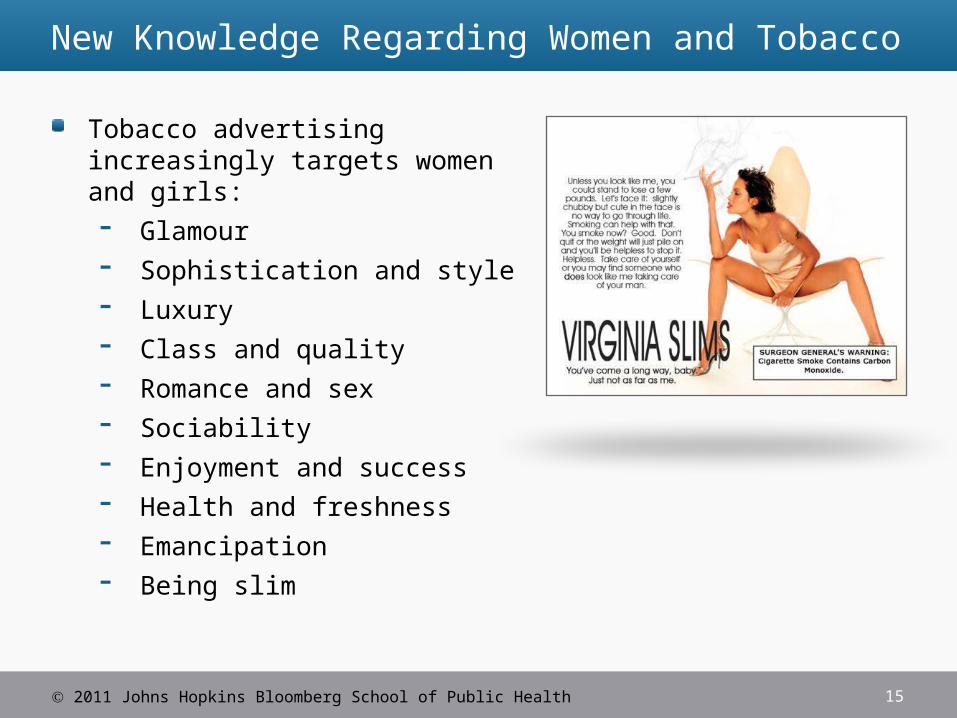
Tobacco advertising increasingly targets women and girls: Glamour Sophistication and style Luxury Class and quality Romance and sex Sociability Enjoyment and success Health and freshness Emancipation Being slim
15

2011 Johns Hopkins Bloomberg School of Public Health
Specialty Packs Aimed at Women
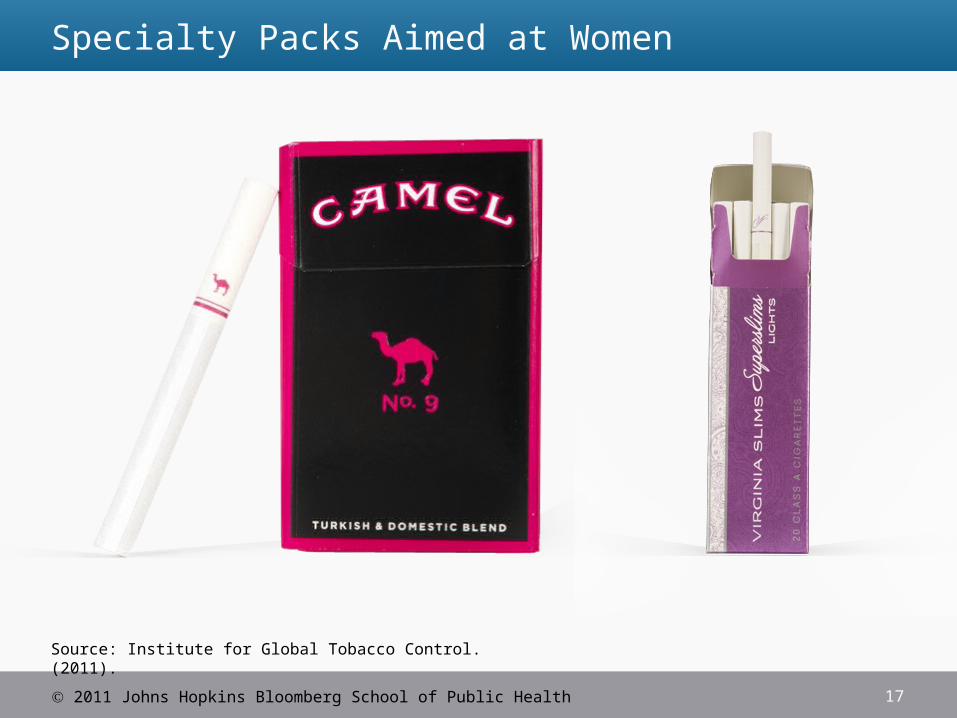
Specialty packs and formulations (“light,” “slim,” and “super-slim”) target the female market For example, about 100 special women’s brands have
been introduced to the Russian market where the prevalence of smoking among women is increasing rapidly
16
2011 Johns Hopkins Bloomberg School of Public Health
Specialty Packs Aimed at Women
17
Source: Institute for Global Tobacco Control. (2011).

2011 Johns Hopkins Bloomberg School of Public Health
New Knowledge Regarding Women and Tobacco
While policy design may be gender-neutral, the policies may affect women and men very differently It is important that the WHO FCTC be implemented
through a gender perspective as part of a country’s political and development agenda:
Monitor tobacco use by gender Protect girls and women of all ages from tobacco
smoke Offer help to assist women in quitting tobacco use Warn women and girls about the dangers of tobacco Enforce bans on tobacco advertising, promotion, and
sponsorship by empowering women to identify and counter these influences
Raise taxes on tobacco, with the active participation of women leaders
18

2011 Johns Hopkins Bloomberg School of Public Health
Messages from Previous Lectures—The Role of Nurses
Over 11 million nurses in the world have the power to make a huge difference
Nurses enjoy public trust and can be pivotal partners
Barriers to nursing involvement in tobacco control: Smoking status of nurses themselves Limited tobacco control content in nursing school
education Not traditionally a part of nursing practice Lack of knowledge and fear of causing patient/visitor
stress Lack of professional leadership
19

2011 Johns Hopkins Bloomberg School of Public Health
Messages from Previous Lectures—The Role of Nurses
Opportunities for involvement in tobacco control: Nurses need to move beyond bedside care to influence
the policy making process Become advocates and get involved—World No
Tobacco Day, supporting smoke-free public places, etc. Integrate tobacco control interventions into current
practice Implement curriculum changes in nursing schools Create workplace committees to enhance awareness Include “smoking status” as a vital sign on patient
records Support improving the quality of cessation treatment
20

2011 Johns Hopkins Bloomberg School of Public Health
New Knowledge Regarding the Role of Nurses
There are now over 17 million nurses worldwide
Research indicates that tobacco cessation activities can be effectively provided by nurses (Rice and Stead, 2008)
Continuous declines in smoking rates among nurses have been documented in countries where regular data has been recorded over time (e.g., the United States, New Zealand, and Australia)
However, research conducted among nursing students in some countries has found contemporary tobacco usage rates higher than that of the general population (Smith and Takahashi, 2008)
21

2011 Johns Hopkins Bloomberg School of Public Health 22
New Knowledge Regarding the Role of Nurses
Challenges (Smith, 2010): The rate of smoking among nurses remains
unacceptably high in some countries Strategic directions for tobacco control in nursing are
needed The provision of educational programs in the workplace
and the addition of tobacco control programs to the nursing education curricula
Further research is needed to determine the most effective educational strategies
2011 Johns Hopkins Bloomberg School of Public Health
Summary
While progress has been made in controlling tobacco use among special populations, the tobacco industry remains relentless in its pursuit of new customers among the poor, youth, and women
The overall burden of the tobacco epidemic is increasingly being borne by the poor
Controlling the tobacco epidemic among special populations requires a concerted, collaborative effort across sectors In this context, the leadership of a fully engaged, non-smoking,
100% smoke-free health sector is essential
23